Article Text

Abstract
Objective The Outreach distal access catheter (DAC; Concentric Medical, Mountain View, California, USA) has been designed to assist the Merci device (Concentric Medical) with clot retrieval in the setting of acute stroke. Its application for coil embolization of intracranial aneurysms was investigated.
Methods Between December 2008 and January 2010, 150 aneurysms were treated with endovascular methods. In 18 cases of small aneurysms and/or increased parent vessel tortuosity, the DAC was used for additional support. Merits and complications related to the use of this catheter are reviewed.
Results The mean aneurysm size was 7.1 mm (range 3.5–25). In each case, the DAC was used as an intracranial platform catheter in close proximity to the target aneurysm. This catheter (outer diameter 3.9 or 4.3 French) increased the stability and reduced the redundancy of the microcatheter. As a result, handling and control of the microcatheter were improved. In three cases, the coiling procedure could not be completed because of difficulties not related to the DAC. Aneurysms in the remaining patients were treated successfully with complete (n=12) or near complete (n=3) angiographic occlusion.
Conclusion For smaller or distal intracranial aneurysms with difficult access, use of the DAC as an additional platform in close proximity to the target aneurysm subjectively enhanced microcatheter control and safety.
Statistics from Altmetric.com
Introduction
The Outreach distal access catheter (DAC; Concentric Medical, Mountain View, California, USA) is a small diameter catheter designed to work in conjunction with the Merci Retrieval System (Concentric Medical) during mechanical thrombectomy intervention for acute ischemic stroke.1 In cases of tortuous vessel anatomy, the DAC may provide system stabilization and allow for a proper force vector to be applied to the thrombus. We proposed that the same concept could be applied to the endovascular treatment of intracranial aneurysms. The DAC can be positioned intracranially close to the target aneurysm. As a result, the DAC, as a second platform catheter, reduces force vectors acting on the microcatheter and microwire during manipulation. This may result in enhanced control and possibly increased safety of the endovascular procedure. In this report, we summarize our preliminary experience with the use of DAC technology for the endovascular treatment of select intracranial aneurysms.
Methods
The DAC has been available for endovascular use at Millard Fillmore Gates Hospital since its release in October 2008. Chart review revealed that from December 2008 to January 2010, 150 patients were treated with endovascular coil embolization of intracranial aneurysms. Eighteen cases involved DAC use during the course of treatment. The DAC was used in these patients in an attempt to create a stable platform as a basis for micronavigation in close proximity to the aneurysm and thus to overcome anticipated difficulties secondary to small aneurysm size and/or increased parent vessel tortuosity. A retrospective analysis of these 18 cases was undertaken. The institutional review board at the University at Buffalo approved the study and a standard Health Insurance Portability and Accountability Act compliant protocol was followed.
Procedures and interventions
All study patients underwent a standard digital subtraction angiogram (DSA) and rotational angiography with three dimensional reconstructions to characterize aneurysm and parent artery anatomy. All procedures involved the use of a femoral artery sheath and a 6 French (Fr) or 7 Fr guide catheter. The selection of the microcatheter–microwire system was based on the anatomy of the aneurysm–parent vessel configuration. Typically, a Synchro-2 microwire (Boston Scientific, Natick, Massachusetts, USA) and an SL-10 microcatheter (Boston Scientific) were chosen. In unruptured aneurysms, the procedure was performed under systemic heparinization with an activated coagulation time ranging between 250 and 350 s. In cases of ruptured aneurysms, the patient received a maximum of 2000 units of heparin initially and was heparinized to an activated coagulation time of >250 s after placement of the first coil. For aneurysm coiling, the DAC was used as part of a triaxial system (guide catheter, DAC, microcatheter). The DAC is manufactured with outer diameters of 3.9 and 4.3 Fr. Each component of the triaxial system was connected to its own flush line. After introduction of the guide catheter into the cervical segment of the parent vessel using a 0.035 inch glide wire, the DAC, microcatheter and microwire were advanced in a telescoped fashion towards the target aneurysm. The DAC then served as a new platform catheter placed as close as possible to the target aneurysm (within 1.5–2.5 cm proximal to the aneurysm in most cases). The degree of aneurysm occlusion was based on the angiographic imaging studies performed immediately after coiling. The degree of occlusion was graded as complete (100% without any residual), near complete (90–99% occlusion, small neck or small dome residual) and none (endovascular treatment was aborted).
Results
Patient, aneurysm and procedural characteristics
Mean patient age was 57.8 years (range 38–84); 16 patients (89%) were women. The mean aneurysm size was 7.1 mm (range 3.5–25). Aneurysm locations included the basilar artery (superior cerebellar artery (SCA), n=1), vertebral artery (VA) (posterior inferior cerebellar artery (PICA), n=3 and vertebrobasilar junction (VBJ), n=1) and internal carotid artery (ICA) (ophthalmic artery, n=3; superior hypophyseal artery, n=1; posterior communicating artery (PcomA), n=1; anterior choroidal artery (AchA), n=1; anterior cerebral artery (ACA), n=1; anterior communicating artery (AcomA), n=4; pericallosal artery, n=1; and middle cerebral artery (MCA), n=1) (table 1). Eight patients (47%) presented with subarachnoid hemorrhage (SAH). Intracranial placement of the DAC in close proximity to the target aneurysm was established in all cases. For posterior circulation aneurysms (SCA, PICA, VBJ), the DAC was positioned in the intracranial VA or basilar artery. The DAC was positioned in the intracranial ICA for anterior circulation aneurysms (ophthalmic artery, PcomA, AchA, AcomA and ACA) and was advanced into the proximal MCA segment in the case of an MCA aneurysm and up to the ICA bifurcation in the case of a pericallosal artery aneurysm (failed to track into the ACA).
Patient, aneurysm and procedural characteristics
Using the DAC, aneurysm microcatheterization was straightforward in 17 cases, with endovascular coiling accomplished in 15 patients. In three cases, coiling could not be completed although positioning of the DAC was successful. The coils did not remain within the confines of a wide necked aneurysm in two patients. In these cases, the coils were retrieved uneventfully and the procedure was aborted. In the third patient, we attempted stent assisted coiling for the residual of a giant PcomA aneurysm. The patient (whose age was in the mid-80s) had extreme vessel tortuosity and a tight carotid siphon, preventing navigation of the stent beyond the siphon with or without DAC support. Ultimately, the patient developed a thromboembolic complication with acute occlusion of the ACA. Successful treatment was performed with mechanical wire manipulation and intra-arterial tissue plasminogen activator injection. The patient remained asymptomatic and the procedure was aborted. This technical complication was likely unrelated to the DAC but instead a consequence of repeated catheterization of the partially thrombosed aneurysm with probable mobilization of intra-aneurysmal clot. In another case (patient No 8), roadmap imaging was compromised using a 6 Fr Envoy guide catheter (Cordis, Warren, New Jersey, USA) in combination with the larger 4.3 Fr DAC. The DAC was removed and the aneurysm was coiled without DAC support. Since this experience, we use the 6 Fr Envoy in combination with the 3.9 Fr DAC and the 7 Fr guide catheter with the 4.3 Fr DAC so as not to compromise the roadmap or ongoing DSA quality.
Among the 18 study patients, complete (100%) angiographic occlusion of the aneurysm was achieved in 12 cases and near complete (90–99%) occlusion was achieved in three cases. In three patients, the procedure was aborted; in one of these patients, the aneurysm was later clipped successfully. None of the patients suffered any permanent neurological deficits.
DAC assessment
The DAC was used during the endovascular procedure in all 18 cases studied. As mentioned, aneurysm microcatheterization was straightforward and uneventful in 17 cases. With the DAC as an additional platform catheter within the intracranial compartment placed in the VA or ICA, we were able to significantly shorten the length of the unsupported microcatheter between the platform catheter and the target aneurysm. As a result, microcatheter handling was markedly improved, similar to the application of the DAC as an adjunct to the Merci device. With the enhanced microcatheter control, we felt that some of the technical challenges in cases of small aneurysms with increased parent vessel tortuosity could be overcome using the DAC, ultimately adding to the safety of the procedure. It was also apparent that microcatheter behavior in and around the aneurysm translated to manipulations of the microwire from the vascular access site (groin) much closer to the 1:1 optimal ratio. Further, once the microcatheter was in place within the aneurysm, the kickback from coils appeared reduced, which was likely secondary to enhanced stability of the microcatheter within the DAC. Overall, the DAC appeared to provide the neurointerventionists with improved control in and around the aneurysm. In one case, we were able to simply advance the microcatheter through the DAC without the need for microwire catheterization of a very small aneurysm. This maneuver made it safer to catheterize and prevented possible intraprocedural rupture from microwire perforation. It is difficult to quantify such qualitative experiences but the use of this tool essentially simplified the coiling procedure in cases typically associated with increased technical difficulty—namely, small aneurysms and tortuous access by enhancing the neurointerventionist's control over microcatheter and wire behavior.
Illustrative case
A patient (age in the late 50s) presented with a 1 week history of confusion and worsening headache and lethargy. A non-contrast cranial CT scan revealed SAH primarily within the left sylvian fissure (figure 1), and a CT angiogram revealed a small left MCA aneurysm consistent with the hemorrhage. The patient was intubated and an external ventricular drain was placed. A diagnostic DSA revealed a 3.5×3.1 mm aneurysm of the left anterior temporal artery (figure 2). After discussion with the patient's family, the decision was made to perform direct coiling of the aneurysm under general anesthesia. After obtaining guide catheter access to the left ICA, the microcatheter and microwire were advanced into the distal MCA. A 038/125 cm (3.9 Fr outer diameter) DAC was advanced into the M1 segment of the left MCA (figure 3). The added stability allowed for catheterization of the aneurysm without advancement of the microwire beyond the microcatheter tip and hence without going into the aneurysm. The aneurysm was coiled successfully and the anterior temporal artery was preserved (figures 4 and 5). The patient was extubated on postoperative day 3. The external ventricular drain was removed a few days later and the patient was transferred to the neurosurgical ward. Subsequently, the patient had worsening headaches and confusion, and imaging revealed progressive hydrocephalus. A ventriculoperitoneal shunt was inserted and the patient made a good recovery and was discharged home.
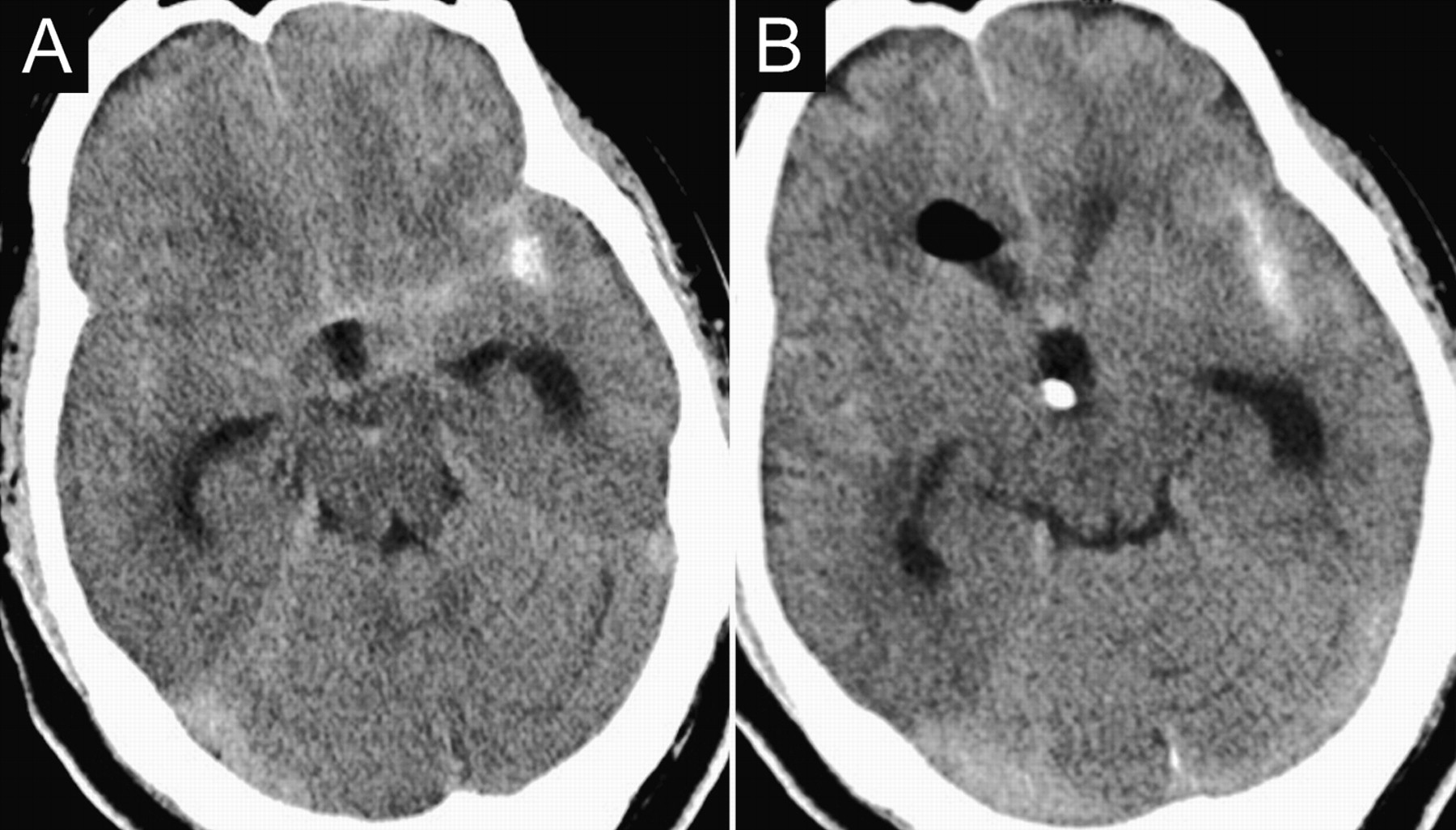
(A, B) Serial axial sections on non-contrast cranial CT imaging demonstrate subarachnoid hemorrhage predominantly in the left sylvian fissure. A right frontal external ventricular drain has been placed for hydrocephalus.

Anteroposterior digital subtraction angiogram demonstrates a 1.5×1.3 mm aneurysm at the left anterior temporal artery origin (arrow).
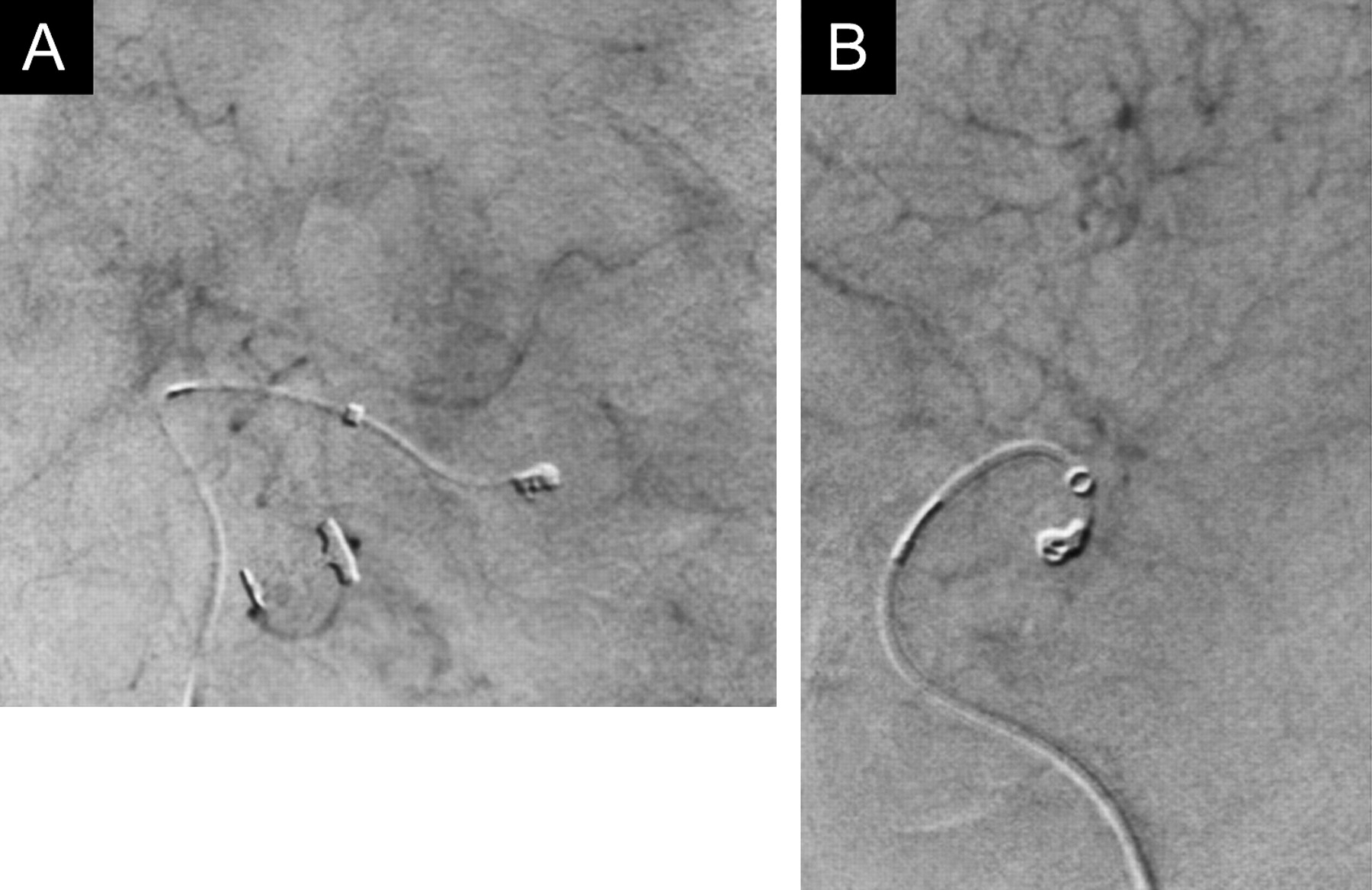
(A) Anteroposterior and (B) lateral digital subtraction angiogram demonstrates the distal access catheter (DAC) proximal to the aneurysm and the microcatheter in the aneurysm for coiling. Due to the stability provided by the DAC, this ruptured aneurysm was catheterized without the microwire.
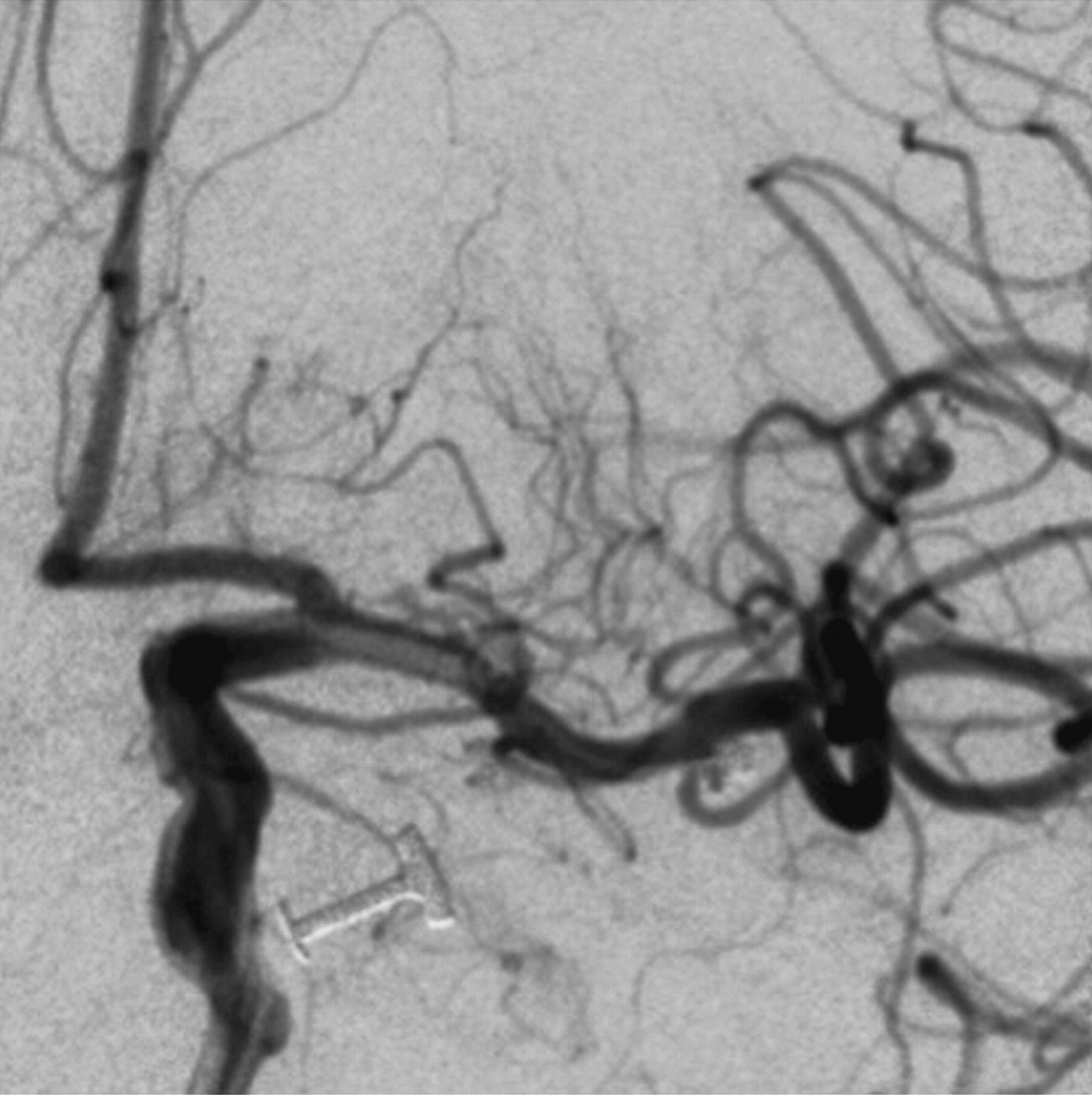
Anteroposterior digital subtraction angiogram of the anterior temporal artery after coiling demonstrates aneurysm obliteration and preservation of the anterior temporal artery.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Final anteroposterior run again demonstrates a well coiled aneurysm with preservation of the left anterior temporal artery.
Discussion
The DAC, originally designed to create a stable platform for thrombectomy in stroke, may be beneficial for the endovascular treatment of intracranial aneurysms, particularly in cases with difficult access or small or more distal aneurysms. In our experience, the DAC established increased system stability by moving the platform catheter closer to the target aneurysm. As a result, precision and control over microcatheter behavior were subjectively improved. With a conventional platform catheter positioned extracranially, the operator needs to navigate the microcatheter through parent vessel turns both intra- and extracranially. Each additional turn adds force vectors counteracting the fine control over the microcatheter. Although an advanced operator should be able to negotiate a microcatheter from a more proximal guide position through multiple parent vessel turns with precise control, it still remains a concern, especially in smaller and more distal aneurysms or for aneurysms with increased parent vessel tortuosity. With ‘elimination’ of multiple parent vessel turns between the microcatheter tip and the platform catheter as well as with reducing that distance by advancing the platform catheter further intracranially, the number of these various impeding force vectors associated with every parent vessel turn is reduced.
A similar concept is realized using a 6 Fr Neuron guide catheter (Penumbra, Inc, San Leandro, California, USA), as previously described by Park and colleagues.2 The Neuron guide catheter is designed with a more flexible distal tip allowing for more distal extra- or intracranial placement closer to the lesion. Park et al successfully treated seven patients with various intracranial pathologies with the Neuron catheter; three of those patients had intracranial aneurysms. Equivalent to indications for using the DAC, Park et al selected patients deemed to have either tortuous supra-aortic, intracranial and/or extracranial vasculature, or to require additional microcatheter support as the result of lesion location. Similar to our experience, Park et al concluded that distal intra- or extracranial placement of a specially designed compliant guide catheter can improve access and microcatheter stability in patients with tortuous vessels or difficult to reach lesions.
An inherent disadvantage associated with the use of the DAC is the need for an additional co-axial catheter system with an additional flush line, which involves more complex handling and additional cost. The selection of a practical combination of guide catheter and DAC is critical. If a DAC size is chosen that results in near occlusion of the primary guide catheter (such as in patient No 8), the ability to obtain high quality roadmaps for microcatheter navigation and intraprocedural angiographic runs may be impaired. We recommend the use of a 6 Fr primary guide catheter, such as the 6 Fr Envoy catheter (Codman and Shurtleff, Raynham, Massachusetts, USA) in combination with a 3.9 Fr DAC. Conversely, this modular system has its advantages over a single catheter system, such as the Neuron guide catheter. The 6 Fr primary guide provides a robust ‘sheath’ for the DAC with ultimately more rigidity proximally, which may improve ‘pushability’ for the DAC. The more flexible DAC then can be advanced distally (independent of the less flexible support catheter) to the desired position. As with any other larger catheter, careful manipulation with good clinical judgment is advised to avoid possible catheter related complications, such as dissections.
Conclusion
The DAC, originally designed for stroke interventions, is a useful adjunct in the treatment of select intracranial aneurysms, specifically smaller or distal aneurysms with increased parent vessel tortuosity. The DAC serves as an intracranial platform catheter and thus enhances microcatheter control by advancing the guide platform closer to the lesion.
Key messages
The Outreach distal access catheter (DAC; Concentric Medical, Mountain View, California, USA) was originally designed to facilitate clot retrieval in the setting of acute stroke.
We used the DAC as an additional support catheter during the treatment of 18 intracranial aneurysms.
Our initial experience suggests the DAC may enhance microcatheter control and overall safety, particularly for the treatment of smaller or distal aneurysms with difficult access.
Acknowledgments
The authors thank Paul Dressel, BFA, for help with preparation of the illustrations and Debra J Zimmer, AAS CMA-A, for editorial assistance.
Footnotes
Competing interests LNH receives research study grants from Abbott (ACT 1 Choice), Boston Scientific (CABANA), Cordis (SAPPHIRE WW) and ev3/Covidien Vascular Therapies (CREATE), and a research grant from Toshiba (for the Toshiba Stroke Research Center); has an ownership/financial interest in AccessClosure, Boston Scientific, Cordis, Micrus and Valor Medical; serves on the Abbott Vascular Speakers' Bureau; receives honoraria from Bard, Boston Scientific, Cordis and from the following for speaking at conferences: Complete Conference Management, Cleveland Clinic and SCAI; receives royalties from Cordis (for the AngioGuard device); serves as a consultant to or on the advisory board for Abbott, AccessClosure, Bard, Boston Scientific, Cordis, Gore, Lumen Biomedical, and Toshiba; and serves as the conference director for Nurcon Conferences/Strategic Medical Seminars LLC. EIL receives research grant support (principal investigator: Stent-Assisted Recanalization in acute Ischemic Stroke, SARIS), other research support (devices) and honoraria from Boston Scientific and research support from Codman and Shurtleff, Inc and ev3/Covidien Vascular Therapies; has ownership interests in Intratech Medical Ltd and Mynx/Access Closure; serves as a consultant on the board of scientific advisors to Codman and Shurtleff, Inc; serves as a consultant per project and/or per hour for Codmann and Shurtleff, Inc, ev3/Covidien Vascular Therapies and TheraSyn Sensors, Inc; and receives fees for carotid stent training from Abbott Vascular and ev3/Covidien Vascular Therapies. EIL receives no consulting salary arrangements. All consulting is per project and/or per hour. AHS has received research grants from the National Institutes of Health (co-investigator: NINDS 1R01NS064592-01A1, Hemodynamic induction of pathologic remodeling leading to intracranial aneurysms) and the University at Buffalo (Research Development Award); holds financial interests in Hotspur, Intratech Medical, StimSox, and Valor Medical; serves as a consultant to Codman & Shurtleff, Inc., Concentric Medical, ev3/Covidien Vascular Therapies, GuidePoint Global Consulting, and Penumbra; belongs to the speakers' bureaus of Codman & Shurtleff, Inc. and Genentech; serves on an advisory board for Codman & Shurtleff; and has received honoraria from Abbott Vascular, American Association of Neurological Surgeons' courses, an Emergency Medicine Conference, Genentech, Neocure Group LLC, and from Abbott Vascular and Codman & Shurtleff, Inc. for training other neurointerventionists in carotid stenting and for training physicians in endovascular stenting for aneurysms. AHS receives no consulting salary arrangements. All consulting is per project and/or per hour.
Ethics approval The institutional review board at the University at Buffalo approved the study, and a standard Health Insurance Portability and Accountability Act (HIPAA) compliant protocol was followed.
Provenance and peer review Not commissioned; externally peer reviewed.
Unlabeled use of products The use of the distal access catheter (DAC, Concentric Medical) for the treatment of intracranial aneurysms is considered an off-label United States Food and Drug Administration application because this catheter has specifically been designed to work with the Merci retrieval system (Concentric Medical) to aid in clot removal.