Article Text

Abstract
Introduction Intracranial dural arteriovenous fistulas (dAVFs) with perimedullary drainage are an uncommon but well-recognized lesion that can lead to spinal cord edema. The authors present a case of a foramen magnum dAVF with unilateral arterial supply from the ascending pharyngeal artery.
Presentation A 49-year-old male presented with a 1-year history of slowly progressive lower extremity weakness and underwent a two-level cervical corpectomy for presumed spondylotic myelopathy. On further workup, he was found to have a dAVF arising from the ascending pharyngeal artery.
Intervention Selective angiography revealed the origin of the neuromeningeal trunk, which was proximal to the arteriovenous fistula. The microcatheter was advanced into the neuromeningeal trunk past the origin of the inferior tympanic artery and origin of the hypoglossal artery. A 4×7 mm Hyperform balloon (EV3, Irvine, California, USA) was then delivered past the origin of the vessel supplying the skull base cranial nerves, but proximal to the microcatheter tip. The balloon was inflated and Onyx embolization was employed to obliterate the fistula with controlled penetration. The patient showed immediate postprocedural improvement in motor function.
Discussion Embolization of branches of the ascending pharyngeal artery carries risks of inadvertent embolization of branches of the neuromeningeal trunk as well as the risk for extracranial to intracranial anastamoses. An awareness of the highly variable anatomy of the ascending pharyngeal artery is necessary for the safe treatment of lesions supplied by this artery. This is, to the authors' knowledge, the first report of balloon-augmented embolization of an arteriovenous fistula arising from the neuromeningeal trunk.
- Arteriovenous fistula
- embolization
- balloon
- ascending pharyngeal
- foramen magnum
Statistics from Altmetric.com
Introduction
Spinal dural arteriovenous fistulas (dAVFs) are the most common vascular malformation that can lead to myelopathy from spinal cord edema and are classically found in the thoracolumbar region. The arterialization of the recipient vein results in venous hypertension and chronic ischemia. Intracranial dAVFs with perimedullary drainage arise much less commonly, but can also lead to cord edema and are found in the foramen magnum and may be fed from vertebral, occipital and ascending pharyngeal artery feeders.1–6 Patients may present with myelopathy or subarachnoid hemorrhage.7–9 To achieve obliteration of a foramen magnum region dAVF, the shunt site may be targeted either by microsurgical clipping10 11 or by superselective embolization via an endovascular approach.12–14 It is not known which method of obliteration is more effective and carries the lowest likelihood of recurrence, so each case should receive an individualized plan by a team capable of performing both approaches. We present a case of a foramen magnum dAVF with unilateral arterial supply from a branch arising from the ascending pharyngeal artery that drained into veins within the foramen magnum, over the cerebellum, and ultimately into the anterior spinal vein. It was successfully treated with a balloon-augmented technique for Onyx embolization (EV3 Neurovascular, Irvine, California, USA). Knowledge of the anatomy of the ascending pharyngeal branch of the external carotid artery including the neuromeningeal trunk is vital to performing endovascular interventions of lesions in the foramen magnum arising from this feeder to avoid cranial nerve injury.
Presentation
A 49-year-old male presented with a 1-year history of slowly progressive lower extremity weakness requiring assistance for ambulation. Over the past 3 weeks, he developed gait instability and progressive upper extremity weakness, right arm greater than left. Urinary incontinence began 2 days prior to presentation. He was evaluated with an MRI of the cervical spine at an outside hospital and given a presumptive diagnosis of transverse myelitis (figure 1A). He underwent lumbar puncture and developed acute onset quadriparesis. The patient was taken emergently for a C4, C5 anterior cervical corpectomy and fusion (figure 1B). Postoperatively, the patient was found to have a further deterioration in motor function, with no motor function in the lower extremities. At this point, in light of the flow voids in the region of the foramen magnum and the disproportionate amount of signal change in the cord compared with the degree of degenerative disease present, a cervicocerebral angiogram was emergently performed. A selective right external carotid angiogram demonstrated an enlarged and torturous ascending pharyngeal artery with early venous opacification at the level of the foramen magnum extending to a vein positioned in the midline traveling along the clivus in a cephalad direction initially, then turning and traveling caudally along the upper cervical spine (figure 2A,B). The lesion was low flow with evidence of venous congestion. There were no other abnormal vessels identified.

(A) and (B) In addition to the degenerative changes involving the cervical spine, the T2-weighted magnetic resonance images demonstrate cord enlargement and diffuse hyperintensity from C2 to C6. There are abnormal vascular structures at the level of the foramen magnum dorsally (white arrow) and at the level of the pontomedullary junction ventrally.

(A) Selective right external carotid angiogram demonstrates an ascending pharyngeal artery with early venous opacification at the level of the foramen magnum extending to a cervical radicular vein (B). (C) A microcatheter (white arrow) angiogram demonstrates the neuromeningeal trunk (black arrow) and the fistulous connection. (D) Angiogram with the microcatheter (white arrow) navigated distal to the hypoglossal and jugular branches of the neuromeningeal trunk. (E) The balloon (red arrow) is inflated distal to the hypoglossal and jugular branches of the neuromeningeal trunk and Onyx embolization proceeds with excellent penetration and minimal reflux (F) (balloon position: red arrow). (G) Post-embolization cast is seen on this native view at the level of the foramen magnum.
Intervention
The patient was placed under general endotracheal anesthesia, and fully heparinized. A 0.070 Neuron guide catheter (Penumbra, Alameda, California, USA) was placed into the proximal external carotid artery and a Marathon microcatheter (EV3, Irvine, California, USA) was navigated over a 0.010″ Xpedion microwire (EV3) into the distal ascending pharyngeal. Angiography revealed the origin of the neuromeningeal trunk, which was proximal to the arteriovenous fistula (figure 2C). The microcatheter was advanced into the neuromeningeal trunk immediately adjacent to the site of arteriovenous shunting (figure 2D), into the odontoid arcade and past the origin of the inferior tympanic artery and probable origin of the hypoglossal artery. A 4×7 mm Hyperform balloon (EV3) was then delivered past the origin of the vessel supplying the skull base cranial nerves, but proximal to the microcatheter tip (figure 2E). The balloon was inflated and Onyx embolization was employed to obliterate the fistula with excellent, controlled penetration (figure 2F,G). Only a small amount of Onyx refluxed proximal to the microcatheter at the site of the balloon. Follow-up angiography revealed complete obliteration of the fistula with preserved opacification of the inferior tympanic artery.
The patient showed immediate postprocedural improvement in motor function with full strength in his left arm and proximal right arm, but persistent right handgrip weakness of 0/5. More noticeably, his left leg had return of function to 2/5 strength, while his right lower extremity had immediate recovery to 2/5 proximal strength but 0/5 distally.
At 3 months follow-up, he continues to have a distinct right sided hemiparesis, but with marked improvement from the time of his discharge. He ambulates with the assistance of a walker and an ankle–foot orthotic. He is able to grasp and manipulate objects with his right hand, with a minimum of 4/5 strength in all right arm muscle groups. His left side has returned to full strength.
Discussion
We have described a balloon-augmented Onyx embolization of a dAVF arising from the neuromeningeal trunk of the ascending pharyngeal artery. It is important to realize that making this diagnosis can be difficult, especially in the setting of a patient that is acutely deteriorating and has extensive degenerative disease involving the affected region. Given the recent two-level cervical corpectomy and the location of the lesion, a far lateral approach in park-bench position would have been necessary for a surgical approach for therapy. The surgical positioning risks weighed heavily in the decision by our multidisciplinary neurointerventional team to attempt to treat the lesion with an endovascular approach. Endovascular embolization of branches of the ascending pharyngeal artery carry risks of inadvertent embolization of branches of the neuromeningeal trunk that supply the vasa nervorum of cranial nerves, as well as the risk for extracranial to intracranial anastamoses that might result in inadvertent embolization of branches of the internal carotid artery.
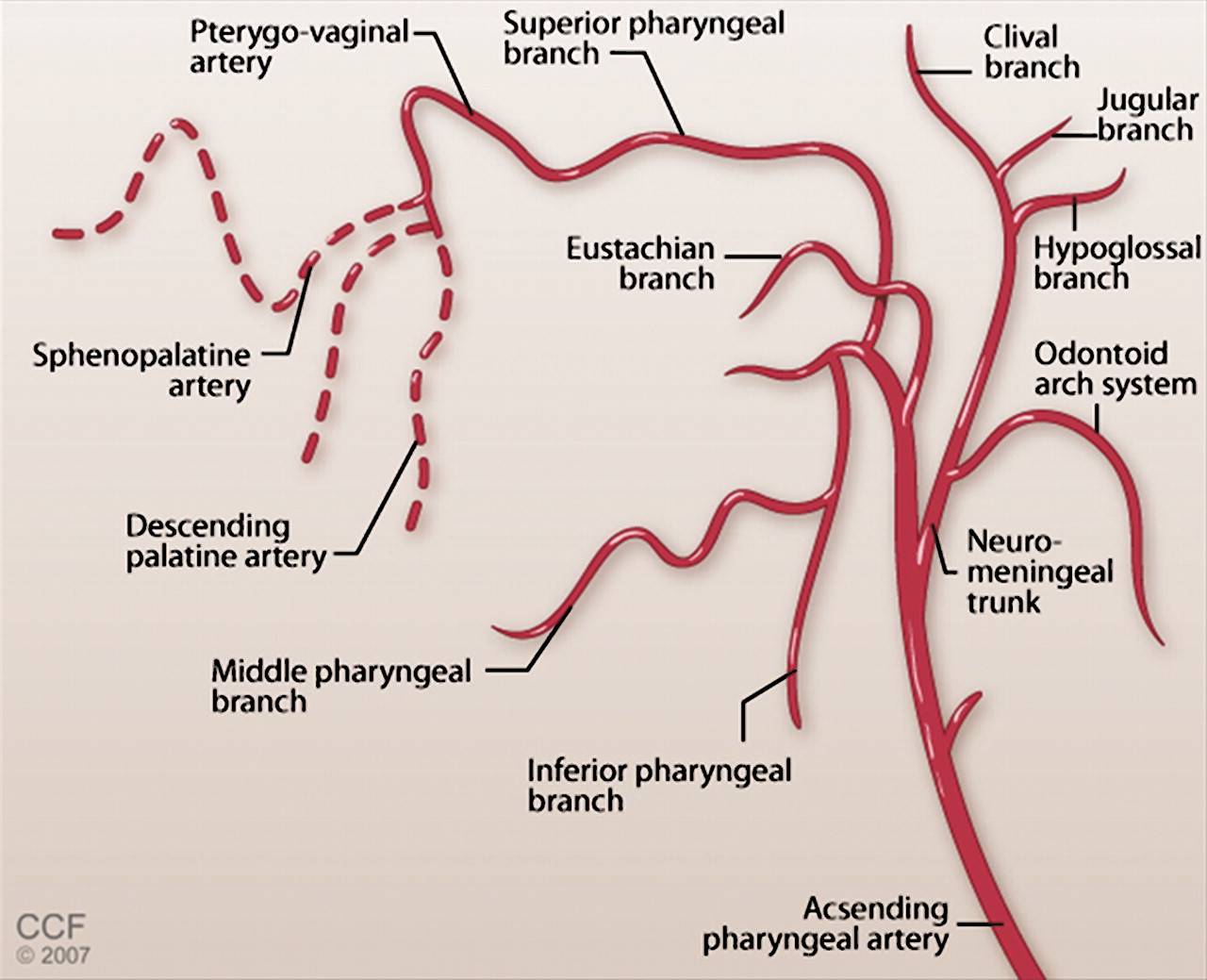
An awareness of the highly variable anatomy of the ascending pharyngeal artery11 15 is necessary for safe treatment of lesions supplied by this artery. The ascending pharyngeal artery has two major branches: the pharyngeal trunk is extracranial, while the neuromeningeal trunk enters the foramen magnum where it branches further to supply the vasa nervorum of cranial nerves IX, X, XI and XII (figure 3).15 Its main branches include the hypoglossal, jugular, internal auditory canal and clival branches. To avoid neurological complications, nontargeted delivery of embolisate to the vasa nervoruma of these vessels must be avoided at all cost. In our case, we performed superselective angiography with a microcatheter to “map out” the branches of the distal ascending pharyngeal. This was crucial to the identification and preservation of the key neuromeningeal trunk branches (the hypoglossal and jugular arteries). Once the anatomy was delineated, a balloon was positioned distal to the take-off of the branches intended to be preserved and inflated proximal to the microcatheter, to reduce the likelihood of reflux into the branch, as well as serve as a proximal “plug” for the Onyx. This resulted in an efficient forward push of the Onyx material with excellent penetration across the low flow, high-pressure fistulous connection. We chose Onyx as the embolization material because of its compatibility with existing balloon systems, and the relatively high conspicuity of small volumes of the embolisate. Success with Onyx in the treatment of dAVFs has been reported previously16 17 and balloon assistance has been reported for high flow arteriovenous fistulas employing glue18 as well as craniofacial arteriovenous malformations.19 This is, to our knowledge, the first report of balloon-augmented embolization specifically of an arteriovenous fistula arising from the neuromeningeal trunk. It is unclear whether the presence of the balloon assisted in protection of the neuromeningeal trunk branches to the cranial nerve vasa nervorum. Indeed, proximal occlusion may result in distal indirect, invisible collaterals that might paradoxically increase the risk of artery to artery embolization near or at the level of the vasa nervorum. Without randomized trials, it would be difficult to determine whether surgical or endovascular approaches are safer and more efficacious. Careful evaluation of the anatomy is essential to minimize the risks to the patient, particularly with regard to the preservation of cranial nerve function. In this case, however, the patient had improvement in motor function postprocedurally and preserved lower cranial nerve function.

{kind=link}
{kind=link}
{kind=link}
Schematic illustration of the anatomy of the ascending pharyngeal artery. Note that this anatomy can be variable.
Key messages
Embolization of dural arteriovenous fistulae arising from the neuromeningeal trunk of the ascending pharyngeal can be challenging.
We present a novel method of balloon-augmented Onyx embolization to treat such a lesion.
References
Footnotes
Competing interests None declared.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Cleveland Clinic.
Provenance and peer review Not commissioned; externally peer reviewed.