Article Text

Abstract
Introduction Carotid sacrifice remains a valuable tool in the treatment of select vascular lesions. Neurointerventionalists have relied on coil embolization as their primary means of carotid sacrifice, a procedure that can be lengthy and expensive with long fluoroscopy times. We investigated a novel technique for carotid sacrifice in a swine model using temporary balloon occlusion to achieve proximal flow arrest in the carotid artery while embolizing the vessel with a liquid embolic agent.
Methods A total of 10 common carotid artery sacrifices were performed in pigs under fluoroscopic guidance. Various balloons were employed to achieve near total proximal flow arrest to allow an Onyx cast to accumulate in the target vessel.
Results The technique for sacrifice was modified during the experiment with the final procedures yielding successful sacrifice using Onyx through a dimethylsulfoxide-tolerant catheter (Echelon 14) with the assistance of two fibered coils and a 5 mm×30 mm Hyperglide balloon resulting in a 2.5 cm long cast.
Conclusion Carotid artery sacrifice using commercially available non-adhesive liquid embolic agents is feasible with balloon assistance, allowing for reduced radiation and material costs. Coils may be beneficial in providing an anchor point for liquid embolic deposition, as well as reducing the volume of liquid embolysate required to achieve vessel occlusion.
- Balloon
- balloon assistance
- carotid sacrifice
- Onyx
- vessel sacrifice
Statistics from Altmetric.com
Introduction
Occlusion of the carotid artery has long been a mainstay in the treatment of cerebrovascular disease. Originally described in the late 1700s for the treatment of penetrating injuries to the neck, carotid ligation was first used to treat an intracranial aneurysm in 1885 by Sir Victor Horsley,1 2 who performed a craniotomy for a suspected middle fossa tumor, but instead found a large aneurysm. Arterial ligation was popularized in the 1800s by John Hunter, who demonstrated safe and reproducible means of ligating certain peripheral arteries.3 4 It was not until 1928, however, that the first planned internal carotid artery (ICA) ligation was performed for the sole purpose of treating a non-traumatic saccular aneurysm.5 With the development of microsurgical techniques in the 1960s and technical advances in surgical clips, aneurysm clipping quickly became the accepted method of cerebral aneurysm treatment. However, some aneurysms are not amenable to surgical clipping due to their size, shape, configuration and location, and surgical ligation of the carotid artery remained an accepted treatment for unclippable carotid artery aneurysms.
As endovascular and open surgical techniques for aneurysm occlusion continue to advance, fewer aneurysms need to be treated via carotid sacrifice. The technique has utility, however, in the treatment of giant ICA aneurysms, particularly those involving the cavernous segment.6 7 Other indications include treatment of carotid–cavernous fistulae not amenable to endovascular treatment and as part of the preoperative management of skull base neoplasms,8 as well as a rescue method for treating carotid blow-outs from trauma9 or following radiation therapy for head and neck malignancies.10 11 The development of techniques that can accomplish the same goal safely while reducing radiation dose and material costs is a worthwhile endeavor. We investigated the technical feasibility of endovascular carotid sacrifice using the ethylene vinyl alcohol copolymer Onyx (eV3 Neurovascular, Irvine, California, USA). We report our results from a proof of concept study wherein various techniques were employed to achieve carotid sacrifice in a porcine model using Onyx with temporary proximal flow arrest.
Methods
The study protocol received approval from the Institutional Review Board and the Institutional Animal Care and Use Committee. A total of 10 vessels were sacrificed in pigs. Vessel diameter ranged from 4 to 5 mm. Each animal was placed under general anesthesia with inhaled agents administered via an endotracheal tube by a veterinarian using standard veterinary technique. The pigs were bolused with 2000 IU of heparin and given maintenance boluses of 500 IU hourly to achieve procedural anticoagulation. Percutaneous access to the arterial system was achieved using standard micropuncture and Seldinger technique over the medial aspect of the pig knee using manual palpation of the superficial femoral artery; femoral artery surgical cut-down was necessary to access one vessel. A 7F sheath was introduced. Under fluoroscopic guidance, a 7F guiding catheter was advanced over a 0.035-inch glidewire into the right or left common carotid artery. A double Tuohy–Borst rotating hemostatic valve (RHV) was attached to the hub of the guiding catheter.
An over-the-wire balloon was placed through one side-port of the RHV and advanced over a microwire into the common carotid artery. A Hyperglide balloon (eV3 Neurovascular) was employed in eight vessels; an Ascent balloon (Micrus Neurovascular, San Jose, California, USA) was used in two. An Onyx-compatible microcatheter (Echelon or Rebar; eV3 Neurovascular) was then advanced through the second side-port of the RHV over a 0.010-inch microwire to a position adjacent or just distal to the balloon. In vessels 1 and 2, the catheter tip was positioned just distal to the balloon. In vessels 3–6, the catheter tip was positioned at the junction of the middle and distal thirds of the balloon. In vessels 7–10, adjunctive coil deployment was employed and the catheter was positioned distal to the balloon within the coil mass. The balloon was inflated and in each case contrast injected through the guiding catheter to confirm flow arrest. Onyx was then slowly injected under blank roadmap guidance into the common carotid artery through the microcatheter until a dense Onyx cast was visualized; Onyx HD-500 was used in the first four vessels and Onyx 34 used in the last six vessels. Once the desired result was obtained, the microcatheter was removed, and then the balloon was deflated and removed under fluoroscopic guidance. Follow-up angiography was performed following each procedure to verify complete occlusion. In five vessels, one or two coils were detached through the microcatheter, distal to the balloon, prior to Onyx embolization. In one vessel, Onyx embolization was done directly through an Ascent balloon catheter, which was also used to achieve flow arrest. The pigs were killed following the procedure, and the occluded vessels harvested.
Results
The materials, technique and results of the carotid sacrifices are detailed for each vessel in table 1.
Summary of the 10 carotid artery sacrifices with listing of the technical details and results
Vessels 1 and 2
The microcatheter was positioned just distal to a 5 mm Hyperglide balloon. There was incomplete balloon occlusion resulting in streaming of Onyx HD-500 into distal territory, yielding non-target embolization. The non-target emboli were small streams of Onyx.
Vessels 3 and 4
Successful occlusion was obtained when a 5-mm Hyperglide balloon was used and the microcatheter tip was positioned at the junction of the middle and distal thirds of the balloon. No contrast streaming was visualized, confirming complete flow arrest. With the microcatheter in this position, Onyx was allowed to reflux along the balloon in order to form the proximal plug. Once this proximal plug was formed, Onyx was slowly injected and allowed to flow distally to form a short cast in the vessel just distal to the balloon. This technique was used with Onyx HD-500, without adjunctive use of coils (figure 1).
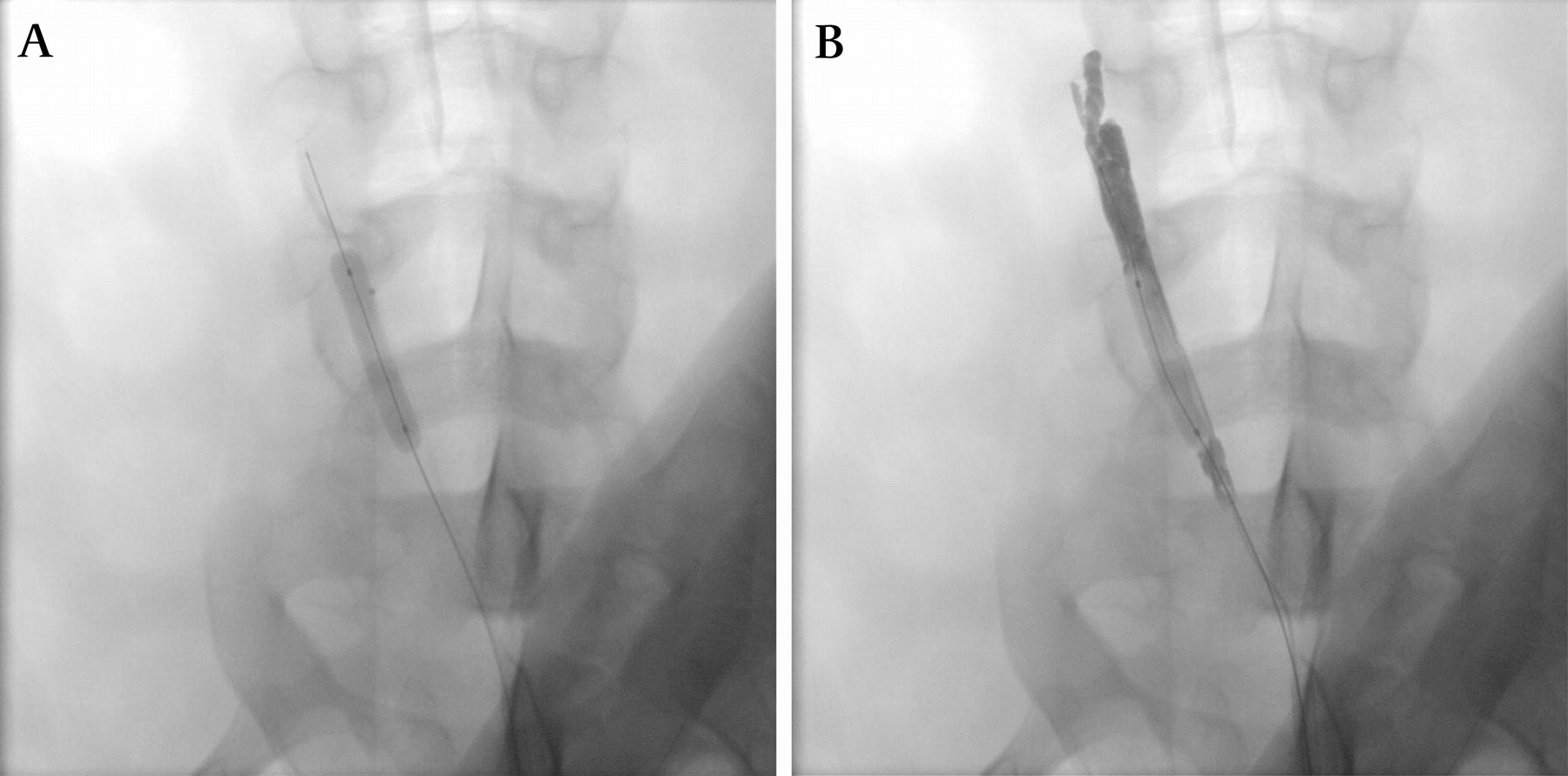
Fluoroscopic image of an Onyx embolization plug in the left common carotid artery of one of the animals. Complete occlusion was achieved with a Hyperform balloon and microcatheter. Note the extension of Onyx proximally.
Vessel 5
Two 6 mm×20 mm fibered coils (eV3) were deployed distal to the balloon, to act as an anchor point for the Onyx cast. We then used the same technique of forming a proximal Onyx plug around the balloon, followed by distal embolization of Onyx into the coils to form the Onyx cast. Onyx 34 was used in this case.
Vessel 6
Onyx 34 was employed without adjunctive use of coils. During the embolization, an adequate Onyx plug and cast formed with complete flow arrest. However, the morphology of the Onyx cast implied underlying vasospasm, as the plug was decreased in caliber as compared with the pre-embolization vessel diameter. Upon follow-up fluoroscopy, as the vasospasm had resolved, the increase in vessel diameter resulted in distal embolization of the Onyx cast. The Onyx cast migrated en masse into the distal common carotid at a bend in the vessel.
Vessel 7
Two 6 mm×20 mm fibered coils (eV3) were deployed distal to the Hyperglide balloon prior to Onyx. The microcatheter tip was placed just distal to the balloon and within the coil mass. Onyx 34 was injected directly into the coil mass.
Vessel 8
An Ascent balloon occlusion catheter was employed to achieve flow arrest. A single 7 mm×200 mm fibered coil (eV3) was deployed prior to Onyx 34 embolization. Vasospasm resulted in deformation of the coil and Onyx cast, and migration of the coil and plug once the vasospasm resolved. The Onyx cast migrated en masse into the distal common carotid at a bend in the vessel.
Vessel 9
An Ascent balloon occlusion catheter was employed to achieve flow arrest. An Echelon microcatheter was placed just distal to the balloon and deployed two platinum coils, 7 mm×300 mm and 7 mm×200 mm (eV3). With the catheter tip within the coil mass we proceeded with Onyx 34 embolization. This technique resulted in successful vessel occlusion.
Vessel 10
A 5-mm Hyperglide balloon was employed to achieve flow arrest with a microcatheter placed just distally through which two coils were deployed (two 7 mm×200 mm platinum coils; eV3). With the catheter tip again within the coil mass we proceeded with Onyx 34 embolization, achieving successful vessel occlusion with a fluoroscopy time of 13 min.
Discussion
Although rarely indicated in contemporary neurovascular practice, carotid sacrifice remains a valuable technique in the treatment of giant ICA aneurysms, carotid–cavernous fistulae and carotid blowouts. With detachable balloons no longer being available in the USA, most neurointerventionalists have relied on coil embolization as their primary means of carotid sacrifice, a procedure that can be lengthy and expensive due to the large volume of coils necessary to achieve vessel occlusion. The costs of the embolic materials used to occlude a vessel vary with the number of coils used. It is not uncommon to use 20–30 coils or more during a vessel sacrifice, with 10–15 coils at bare minimum. The use of Onyx following the deposition of two to three coils proves to be very cost effective (table 2). Additionally, fluoroscopy times are typically long and radiation doses high during sacrifice with coil use alone. The development of faster and more efficient techniques is desirable.
Cost comparison for endovascular carotid sacrifice using the prices available at our institution, reflected as a ratio of its cost relative to the cost of 15 coils
We describe the development of a novel technique for carotid sacrifice in a swine model using temporary balloon occlusion to achieve proximal flow arrest in the carotid artery while embolizing the vessel primarily with the liquid embolic agent Onyx with or without adjunctive coil deployment. This technique achieves vascular occlusion with reduced material costs and shorter fluoroscopy times as compared with coil embolization. We identified valuable technical aspects of this approach.
Liquid embolic agent density
In our initial experiments, Onyx HD-500 was employed due to its higher viscosity. In subsequent experiments, we opted to attempt the technique with Onyx 34. We found no difference between the two agents with regard to ease of delivery, vessel occlusion success rate or complications. Fluoroscopic times were slightly higher when employing HD-500.
Microcatheter position
Microcatheter position relative to the balloon proved to be quite important in terms of achieving flow arrest. In our initial experiments, the catheter tip was placed at or just distal to the distal tip of the balloon. Upon contrast injection through the guide catheter to test for occlusion with this catheter position, there was minimal streaming of contrast around the balloon along the catheter track. This was presumably related to tenting of the balloon by the microcatheter, thereby preventing complete wall apposition by the balloon (figure 2). When Onyx embolization was initiated from this position, there was sufficient streaming around the balloon to cause distal streaming of the Onyx, resulting in unwanted distal and non-target embolization (vessels 1 and 2). Additionally, this undesired effect resulted in the longest fluoroscopy times.
{kind=link}
{kind=link}
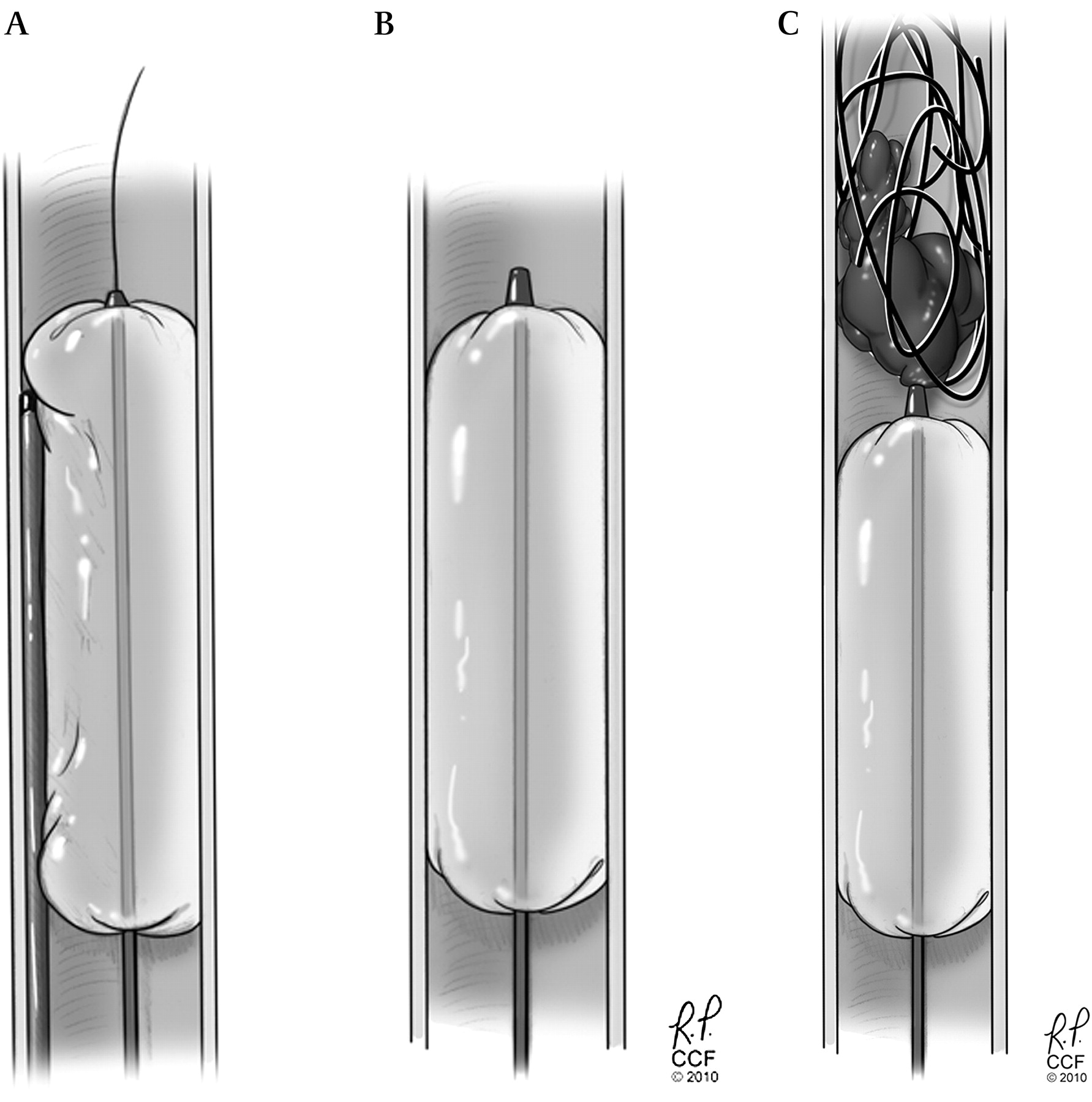
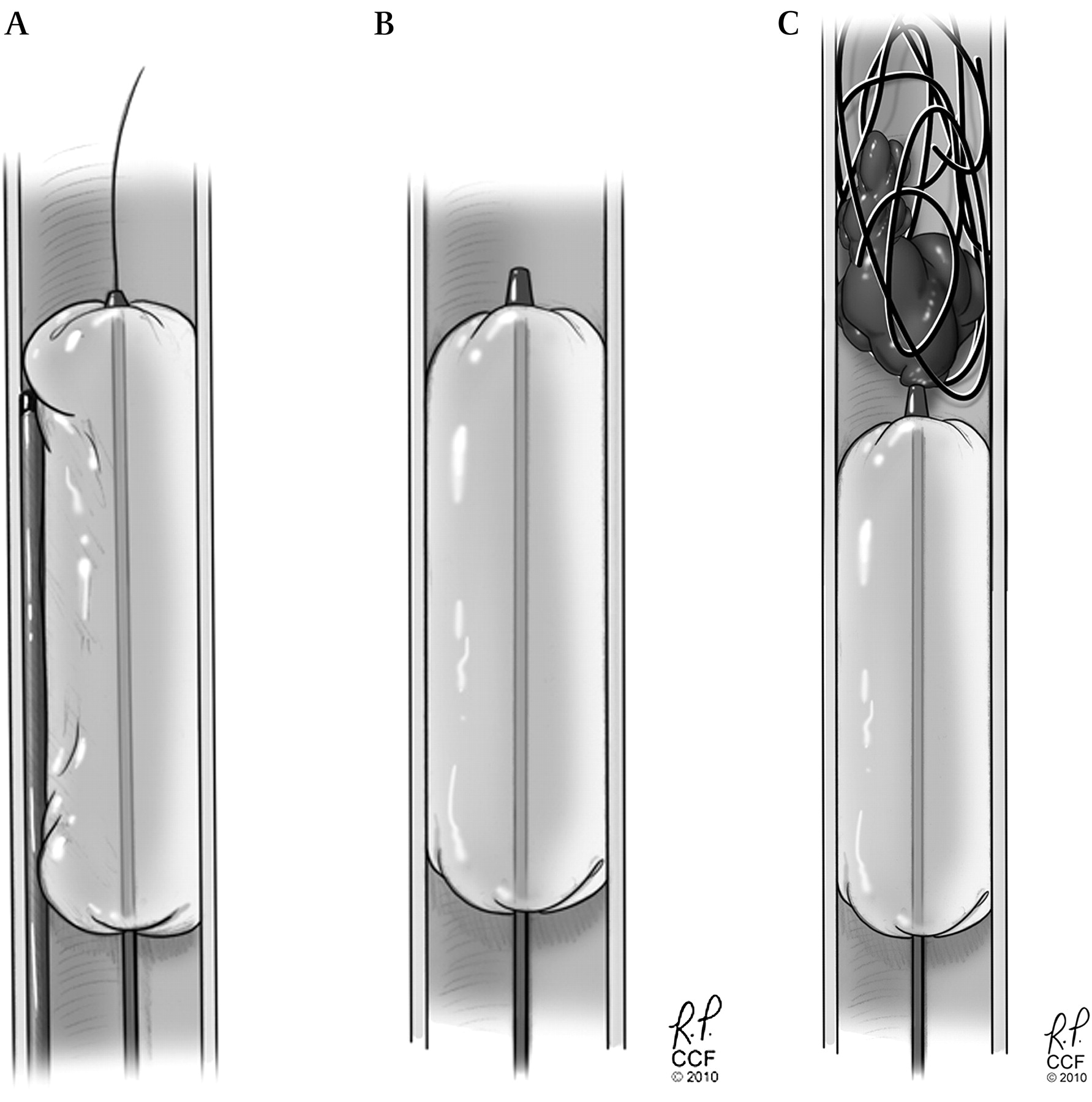
Illustration depicting the merits of the Ascent balloon during balloon-augmented embolization. (A) The use of a Hyperglide balloon and microcatheter in parallel resulted in the undesired effect of incomplete vessel occlusion and streaming around the microcatheter, resulting in embolizate proximal to the balloon position. (B) With the Ascent balloon occlusion catheter, the balloon and microcatheter work in series rather than in parallel since the catheter allows the balloon to be inflated while the working central lumen is available for use in Onyx delivery, thus eliminating all migration of Onyx proximal to the occlusion balloon. (C) The distal end of the working channel is at a fixed distance (3 mm) from the balloon. Two or three anchor coils can be deployed followed by Onyx embolization to achieve occlusion.
On the other hand, when the catheter was retracted so as to position its tip at the junction of the middle and distal thirds of the balloon thereby allowing the distal third of the balloon to circumferentially appose the vessel wall, no further contrast streaming was visualized, confirming complete flow arrest. With the microcatheter in this position, Onyx was allowed to reflux along the balloon in order to form the proximal plug. Once this proximal plug was formed, Onyx was slowly injected and allowed to flow distally to form a short cast in the vessel just distal to the balloon. Successful occlusion was obtained in vessels 3 and 4 using this technique with Onyx HD-500, without adjunctive use of coils. Fluoroscopy times were reduced as well.
Adjuvant coil deployment
In some instances, fibered coils were deployed distal to the balloon to act as an anchor point for the Onyx cast. We then used the same technique of forming a proximal Onyx plug around the balloon, followed by distal embolization of Onyx into the coils to form the Onyx cast. We were able to achieve vessel occlusion with fluoroscopy times comparable to those of cases in which Onyx HD-500 was employed. In another vessel, following the deployment of two fibered coils we placed the microcatheter tip just distal to the balloon and within the coil mass itself and injected the Onyx 34 directly into the coil mass rather than forming a proximal plug around the balloon first. This technique was successful in achieving vessel occlusion with a further reduction in fluoroscopy time.
The most severe complication occurred in a vessel that was sacrified with Onyx 34 without adjunctive use of coils. While an adequate Onyx plug and cast was formed with complete flow arrest, this was done in the setting of underlying catheter-induced vasospasm which occurred during cast formation and was identified due a discrepancy of the Onyx embolization cast and the vessel caliber size on the roadmap control image. With resolution of the vasospasm the Onyx cast embolized distally due to an inadequate amount of purchase. It is unclear whether this would have been averted with the adjunctive use of coils as this complication also occurred in vessel 8, in which two coils were deployed prior to Onyx embolization. The second migration also occurred in the setting of catheter-induced vasospasm. Initial relative overinflation of the balloon may have caused waisting of the target vessel. Subsequently, more careful inflation reduced the occurrence of vessel narrowing/spasm around the balloon. Initial embolization attempts focused on hyperinflation to reduce perimicrocatheter flow. It became apparent that this was not achievable, thus resulting in proximal placement of the microcatheter, allowing complete wall apposition by the balloon distally. The Ascent balloon allowed complete occlusion without hyperinflation and has thus become our technique of choice in humans.
Balloon features
As described earlier, the use of a Hyperglide balloon and microcatheter in parallel resulted in the undesired effect of incomplete vessel occlusion and streaming around the microcatheter, resulting in embolizate proximal to the balloon position. In the last set of vessels, the Ascent balloon occlusion catheter was employed to achieve flow arrest. This technique allows for the balloon and microcatheter to work in series rather than in parallel, since the catheter allows the balloon to be inflated while the working central lumen is available for use in Onyx delivery, thus eliminating all migration of Onyx proximal to the occlusion balloon. While we have found that Hyperglide balloons are generally more flexible and track over a microwire more readily than does the Ascent balloon, this feature is likely not a critical factor as most vessel sacrifices will involve relatively proximal and more accessible vessels.
The major drawback to the use of the Ascent balloon catheter is that it limits the ability to inject Onyx directly into the coil mass since the distal end of the working channel is at a fixed distance (3 mm) from the most distal confines of the balloon. If coil deployment occurs such that the coil mass does not form immediately adjacent to the balloon, this represents a major limitation by introducing a working distance between the working lumen tip and the coil mass, likely necessitating formation of an Onyx plug. However, redeployment of the coil typically allows the operator control of coil location. Moreover, the presence of a space either within the coil mass, or between the coil mass and the balloon, allows a target zone for complete Onyx occlusion. If the coil mass is densely packed, the radio-opacity of the coils limits Onyx visualization, leading to the possibility of inadvertent distal embolization as the first evidence of Onyx injection.
Choice technique
The best technique will be that which combines the highest success rate, technical ease and lower complication rates and radiation exposure. As the technique was developed based on the experiences at each sequential experiment, the most effective and efficient technique for vessel sacrifice was the deployment of two coils distal to the balloon, and Onyx 34 embolization directly into the coil mass to form a dense cast. The Ascent balloon provides the advantage of working channels in series, thereby minimizing any streaming around the balloon. The deployment of coil prior to the initiation of embolization eliminated the need to form a proximal Onyx plug, a technique that can require extensive fluoroscopy time. We were able to achieve vessel occlusion with a median time of 13 min using this technique. When using Onyx 34 without coils or with a single coil, we experienced some difficulty with vasospasm in two vessels, which ultimately resulted in plug migration as the vasospasm resolved. We were able to achieve vessel occlusion without the use of coils in two vessels with Onyx HD-500, but the fluoroscopy times were also slightly higher (16–17 min) and this material may not be as readily available in all neurointerventional labs.
Conclusion
We have described an effective and efficient technique for vessel sacrifice in a pig model using the commercially available liquid embolic agent Onyx, with temporary proximal flow arrest using balloon occlusion and the adjunctive use of coils. The procedure can be performed much more rapidly than the widely accepted method of coil embolization alone, with reduced radiation doses and material costs. However, catheter-related vasospasm resulted in migration of the Onyx cast in 2 out of 10 procedures. Advances in technique and materials will be required to make this procedure safe. Until these refinements take place, we are reminded that surgical suture–ligation remains a viable option for carotid sacrifice.7
Key messages
Sacrificing the internal carotid artery is still a viable option to treat certain lesions and can be performed surgically and endovascularly
Traditionally, an endovascular sacrifice can be a costly and lengthy procedure
We present a novel method of carotid sacrifice tried on a pig model using Onyx supported by coils, which is shorter and less expensive
Footnotes
Funding eV3 and Micrus provided material support for this study. We have no financial interest in the materials mentioned in this paper.
Competing interests None.
Ethics approval The study protocol received approval from the Cleveland Clinic Institutional Review Board and the Institutional Animal Care and Use Committee.
Provenance and peer review Not commissioned; externally peer reviewed.