Article Text

Abstract
Introduction Stent assisted coiling (SAC) of aneurysms has been adopted with potential mechanical, hemodynamic and biologic properties imparting an advantage over coil embolization alone. The purpose of this investigation is to compare the various techniques of SAC at a single institution with regards to clinical, technical and angiographic complications and success.
Methods Patients who underwent SAC between 2003 and 2010 were identified. Clinical charts, procedures, angiographic and non-invasive radiological images were analyzed to determine the anatomical and procedural details and adverse events. Immediate post-procedural angiograms as well as follow-up imaging were studied to assess the degree of aneurysm occlusion.
Results 260 aneurysms were identified. The ‘coil through’ technique was employed in 37.3%, ‘balloon stent’ in 36.2%, ‘jailing’ in 10.8% and the ‘coil stent’ technique in 7.7%. Overall rate of adverse events was higher with the ‘coil stent’ and ‘jailing’ techniques compared with the ‘balloon stent’ technique. The ‘coil through’ technique was associated with a significantly lower packing density (31.4±20%) than all other techniques (‘coil stent’ 45.4±22%, ‘jailing’ 42.2±20%, ‘balloon stent’ 44.3±22%). Among ‘coil stent’ patients, an initial Raymond class 1 was achieved in 40%, compared with 57% of ‘jailing’, 28% of ‘coil through’ and 63% of ‘balloon stent’ cases.
Conclusion Balloon assisted coil embolization followed by adjunctive stent deployment across the aneurysm neck appears to be the superior technique among stent assisted coiling methods at our institution. It combines a lower rate of thrombotic and coil related complications with a high rate of complete occlusion on initial and follow-up imaging.
Statistics from Altmetric.com
Introduction
Since the International Symptomatic Aneurysm Trial study firmly established endovascular therapy as a valid method for treating intracranial aneurysms, development of new techniques has broadened the scope of practice to allow for the treatment of geometrically complex aneurysms.1–6 One such advance has been the development of intracranial stents, which expanded the indications of endovascular therapy to both wide necked and fusiform aneurysms.
The technique of stent assisted coiling (SAC) in the clinical setting was first described in 1997.7 Soon after, the availability of new flexible, self-expanding intracranial stents allowed for increasing application of this technique and observation of its benefits. Stents were quickly adopted as promising adjuncts with potential mechanical, hemodynamic and biologic properties, imparting an advantage over coil embolization alone.8 Stent deployment provides mechanical support to prevent coil prolapse, may serve as a conduit to divert flow and provides a scaffold for endothelial growth and vessel healing.8–10 Since the first clinical applications in the late 1990s, several studies have proven SAC to be a feasible, safe and effective method.11–20
Most aneurysms treated with SAC are geometrically complex and pose a technical challenge. Several strategies have emerged within the technique of SAC which differ with regards to timing of stent deployment and use of other adjuncts such as balloon remodeling. The purpose of this investigation is to evaluate and compare each of these techniques employed in SAC at a single institution with regards to clinical, technical and angiographic complications and success.
Methods
An institutional review board approved prospective database is maintained at Cleveland Clinic for all patients undergoing neuroendovascular procedures. This database was reviewed retrospectively to identify those patients with intracranial aneurysms who underwent embolization utilizing stents between 2003 and 2010, prior to which digital data were not available. The inpatient and outpatient clinical charts, procedural reports, and angiographic and non-invasive radiological images were analyzed to determine the anatomical and procedural details and adverse events.
Stenting technique
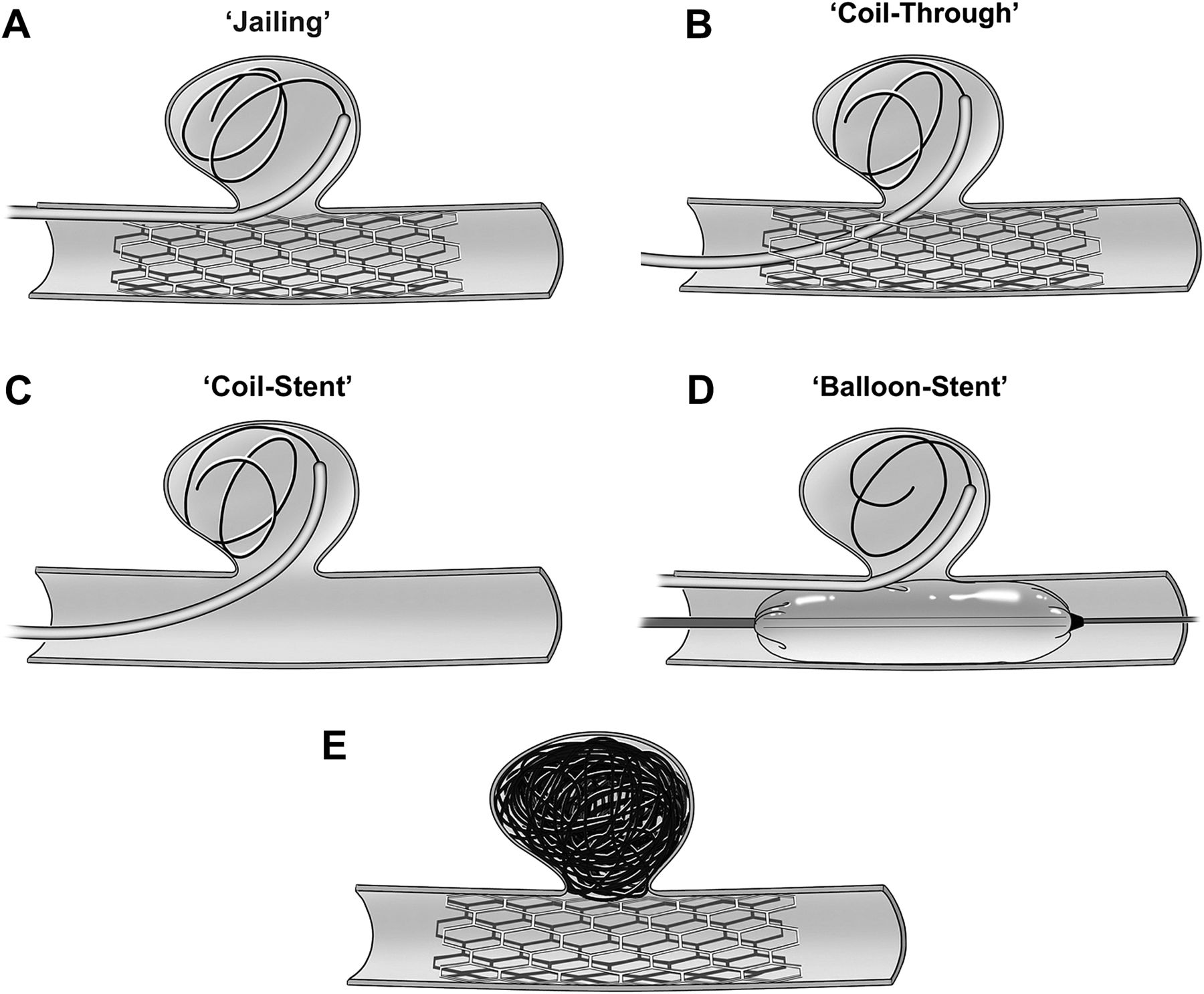
Several techniques were employed (figure 1). The first is ‘jailing’ of the microcatheter in which a stent is deployed after the aneurysm is catheterized but before coil deployment. The microcatheter is effectively pinned between the intima and outer confines of the stent and the coils are kept within the aneurysm and outside of the reconstructed vessel lumen. A second strategy is the ‘coil through’, in which a stent is first fully deployed across the aneurysm neck and then the aneurysm is catheterized by navigating through the tines of the stent. Third, the ‘coil stent’ technique involves an unassisted coil embolization to completion, immediately followed by stent deployment, potentially to capitalize on the biologic benefit of vascular remodeling or to constrain a prolapsed coil loop. Lastly, the ‘balloon stent’ method involves a stent placement after completion of a balloon assisted embolization. Other potential techniques were utilized less frequently as demanded by the individual clinical situation. These alternate techniques included coiling with ‘Y stent’21–23 configuration for basilar tip aneurysms and depositing single or multiple stents for flow diversion to treat blister dorsal carotid wall aneurysms.24
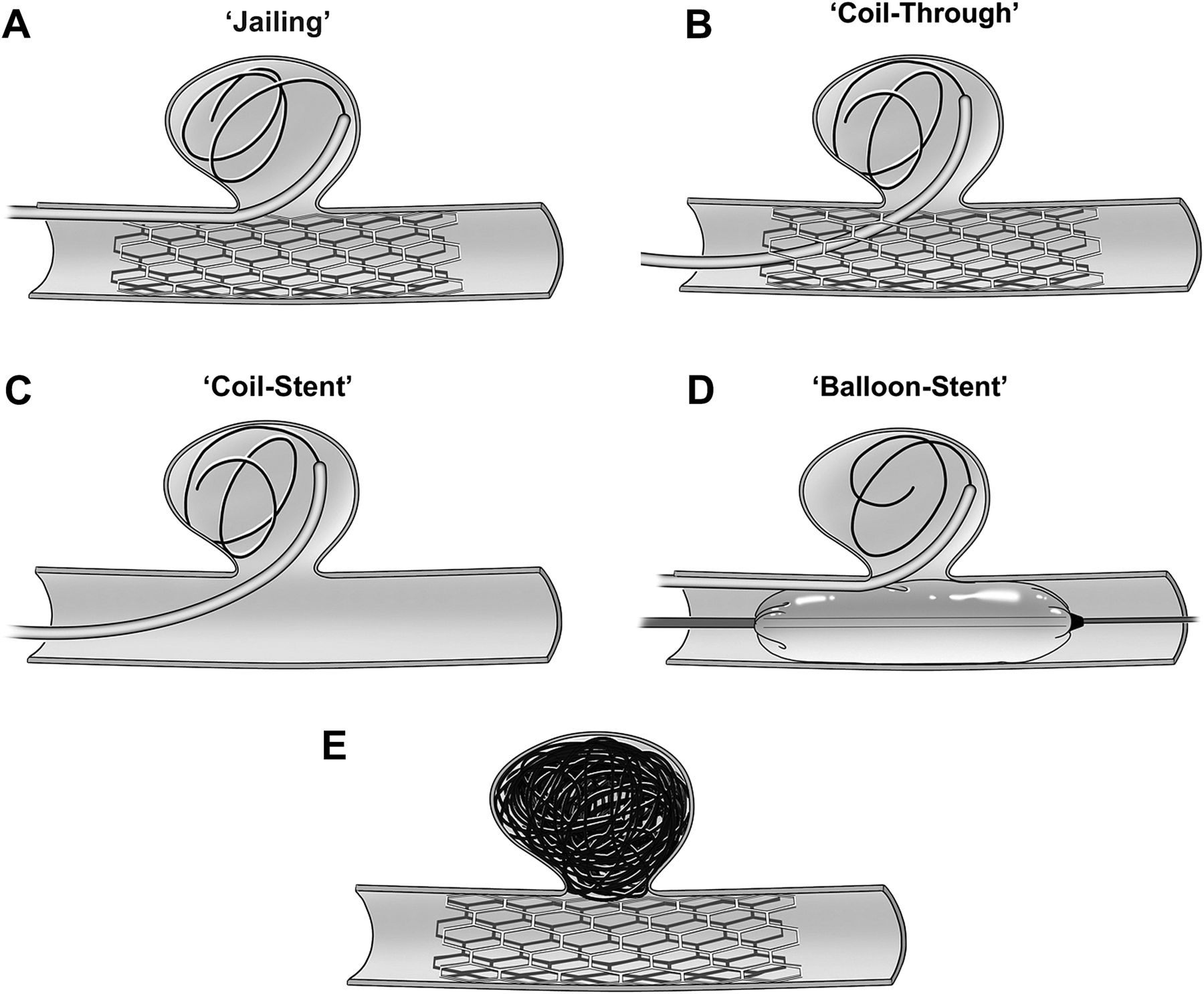
Several techniques of stent assisted aneurysm coil embolization are illustrated. (A) The first is ‘jailing’ of the microcatheter in which a stent is deployed after the aneurysm is catheterized but before coil deployment. The microcatheter is effectively pinned between the intima and outer confines of the stent and the coils are kept within the aneurysm and outside of the reconstructed vessel lumen. (B) A second is the ‘coil through’, in which a stent is first fully deployed across the aneurysm neck and then the aneurysm is catheterized by navigating through the tines of the stent. (C) Third, the ‘coil stent’ technique involves an unassisted coil embolization to completion, immediately followed by stent deployment, potentially to capitalize on the biologic benefit of vascular remodeling or to constrain a prolapsed coil loop. (D) Fourth, the ‘balloon stent’ method involves a stent placement after completion of a balloon assisted embolization. (E) Final treatment result, irrespective of technique.
Adverse events
Occurrences that represented any deviation from an idealized procedure, whether or not they were associated with clinical sequelae, were carefully documented. Several classes of adverse events were defined, including those involving access difficulty such as inability to catheterize aneurysm through stent (first time or on attempted re-entry) or difficulty manipulating microcatheter within aneurysm. Mechanical stent related events included stent migration, misplacement or failed deployment, and mechanical coil related events included coil loop herniation and aneurysm perforation. Thrombotic events included thrombus on stent or coil mass, asymptomatic diffusion restriction on postoperative MRI and clinical evidence of stroke. Remaining events included iatrogenic parent vessel dissection or catheter induced vasospasm requiring intra-arterial vasodilator infusion.
Aneurysm type
In addition to the traditional classification and nomenclature of intracranial aneurysms, aneurysms were categorized by anatomic ‘type’ into three groups: those arising at a bifurcation (n=86; eg, middle cerebral artery, internal carotid terminus, anterior communicating artery, basilar tip), those arising from the sidewall of a straight parent vessel (n=55; eg, mid basilar trunk, posterior communicating artery (PcoA)) or those arising from the sidewall of a curved parent vessel (n=119; eg, ophthalmic artery aneurysms (OAA), superior hypophyseal artery).
Coil packing density
Coil packing density was calculated using the AngioCalc LLC available at http://www.angiocalc.com by determining a best fit of the aneurysms' three-dimensional shape (sphere, ovoid, etc) and entering its dimensions and all of the coils that were deposited into the aneurysm. For bilobed aneurysms, the calculation was determined for each of the lobes considered separately.
Aneurysm occlusion
Immediate post-procedural angiograms as well as follow-up imaging were studied to assess the degree of aneurysm occlusion by the Raymond classification scheme.25
Statistical analysis
Patient groups were compared by χ2 test. Two tailed p values were reported, testing whether the correlation was different from 0. All analyses were performed in SAS V.9.2. A significance level of 0.05 was used to determine significance.
Results
Patients and technique
Two hundred and sixty aneurysms were identified. Aneurysms measured 310±727 mm3, with a neck width of 4.7±2.7 mm and an average maximum dimension of 6.8 mm. A wide range of aneurysm locations were treated with stenting (table 1). The ‘coil through’ technique was employed in 97/260 (37.3%), the ‘balloon stent’ in 94/260 (36.2%), the ‘jailing’ in 28/260 (10.8%) and the ‘coil stent’ technique in 20/260 (7.7%). Additional techniques identified included coiling with ‘Y stent’ configuration for basilar tip aneurysms and depositing single or multiple stents for flow diversion to treat blister dorsal carotid wall aneurysms (n=21, 8.1%) and were excluded from the more detailed analysis as the number of each such procedure was small. The majority of aneurysms were treated electively with only 34 (13.1%) embolized in the setting of subarachnoid hemorrhage.
Distribution of stenting techniques employed for stent assisted coil embolization of the aneurysms included in this study
All procedures were done under general anesthesia with paralysis. All patients in whom stenting was anticipated received aspirin (325 mg daily) and clopidogrel (75 mg daily) for at least 5 days prior to the procedure and underwent testing with platelet aggregometry 1–2 days before the procedure and further loading doses of aspirin and/or clopidogrel administered as necessary. In the event that a stent was required and its use had not been anticipated, the patient was loaded with intravenous or intra-arterial abciximab intraprocedurally and then loaded and maintained on aspirin and clopidogrel. Systemic heparinization was performed prior to introducing the guide catheter and anticoagulation was monitored with a target activated clotting time of 2–2.5 greater than baseline. Intracranial stents used include the Enterprise (Codman and Shurtleff Inc, Raynham, Massachusetts, USA) and Neuform, Neuroform2 and Neuroform3 (Boston Scientific, Massachusetts, USA).
Adverse events
The overall adverse event rate for the various stent techniques was 42% (table 2). These adverse events represented any deviation from an idealized procedure. This was no different for the patients who were treated in the setting of subarachnoid hemorrhage. However, the true complication rate was 4.6% (seven clinically evident strokes, four aneurysm perforations). Among the four primary stenting techniques, 132 adverse events occurred in 106 patients. Overall rate of adverse events was higher with the ‘coil stent’ (p=0.005) and ‘jailing’ (p=0.01) technique compared with the ‘balloon stent’ technique. Access difficulty was significantly more likely to occur with the ‘coil through’ technique (p<0.001) and the ‘jailing’ technique (p=0.001) compared with the ‘balloon stent’. The ‘coil through’ technique demonstrated a trend towards higher likelihood than the ‘coil stent’ technique (p=0.06). None of the other relationships achieved near statistical significance.
Summary of the intraprocedural adverse events categorized by stenting technique
There were no statistically significant differences in rates of mechanical stent or coil related complications such as aneurysm dome perforation, herniation of coil into the parent vessel or stent malposition or migration for the various stenting strategies. Also, the rates of iatrogenic parent vessel dissection and catheter induced vasospasm were similar among the various stenting techniques.
Overall thromboembolic events were higher among the ‘coil stent’ cases compared with ‘coil through’ (p=0.003) and ‘balloon stent’ (p<0.001). In-stent thrombus or clot on coil was significantly more likely to occur with the ‘coil stent’ technique than any of the others. Diffusion weighted imaging abnormalities were least likely to be found on post-procedural MRI in the ‘balloon stent’ group compared with all of the others. A clinical stroke was most likely to follow a ‘coil stent’ and ‘jailing’ procedure as opposed to a ‘balloon stent’ (p=0.04 and p=0.001, respectively). None of the other relationships was found to be significantly different. The rates of iatrogenic complications, including parent vessel dissection or catheter induced vasospasm requiring vasodilator infusion, were equal among all stenting techniques.
Anatomic considerations
Adverse events were studied by aneurysm location but no pattern of complication was clear for the individual techniques. The large number of different aneurysm locations resulted in relatively small sample sizes in each category with the exception of OAA which represented the single largest group of aneurysms that were treated with stent assisted coil embolization (n=82), basilar tip (n=40) and PcoA (n=24) aneurysms. The most frequently employed strategy to treat OAA was ‘balloon stent’ (48%) followed by ‘coil through’ (23%) whereas for basilar tip aneurysms the ‘coil through’ was most frequently used (80%). For PcoA aneurysms, the ‘coil through’ and ‘balloon stent’ techniques were nearly equally utilized.
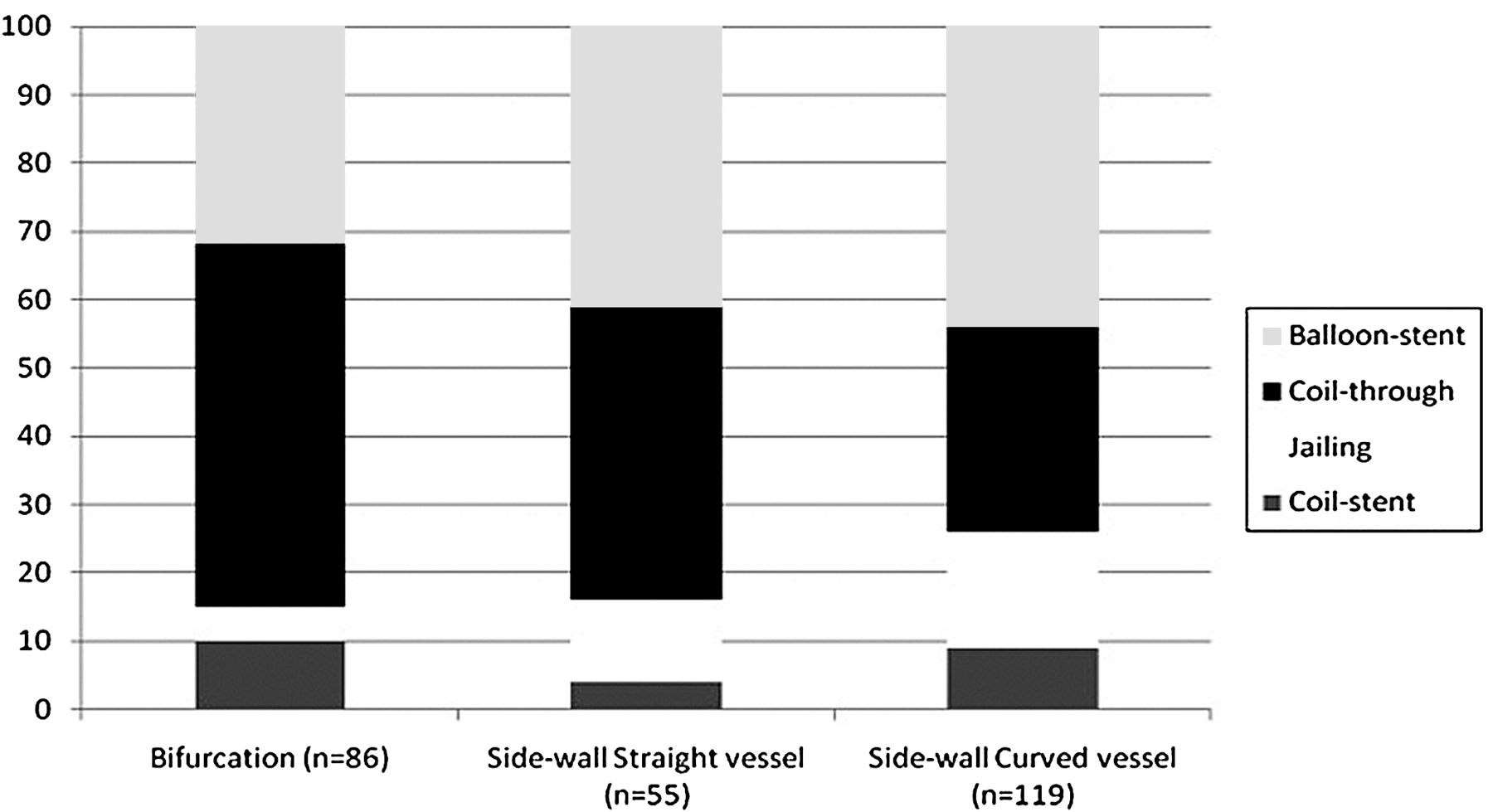
Figure 2 displays the frequency of stent technique employed for the three anatomical types of aneurysms. For aneurysms arising at a major bifurcation (n=86), the ‘coil through’ method was used most commonly while the ‘jailing’ technique was used least frequently. For side wall aneurysms arising from a straight vessel (n=55), the ‘balloon stent’ and ‘coil through’ techniques were employed with similar frequencies. Lastly, for side wall aneurysms arising from a curved vessel (n=119), the ‘balloon stent’ was most frequently used. The rate of adverse events for aneurysms of the bifurcation anatomic type was 49% compared with 38% for straight side wall and 38% for curved sidewall. These rates were not significantly different.

{kind=link}
{kind=link}
Relative frequencies expressed as percentages of stenting techniques employed for the treatment of the three anatomic types of aneurysms.
Coil packing density
The ‘coil through’ technique was associated with a significantly lower packing density (31.4±20%) than all other techniques (‘coil stent’ 45.4±22%, p=0.006; ‘jailing’ 42.2±20%, p=0.003; ‘balloon stent’ 44.3±22%, p<0.001).
Initial angiographic occlusion
Complete aneurysm occlusion (Raymond grade 1) was achieved in 113/260 (43%) of all stent assisted cases while a residual neck (Raymond grade 2) was found in 113/260 (43%) and aneurysm filling (Raymond grade 3) observed in 33/260 (13%). Among ‘coil stent’ patients, an initial Raymond 1 was achieved in 8/20 (40%) compared with 16/28 (57%) of ‘jailing’, 27/97 (28%) of ‘coil through’ and 59/94 (63%) of ‘balloon stent’ cases. Among these, the ‘balloon stent’ had a significantly higher rate of Raymond 1 compared with ‘coil through’ (p<0.001); none of the other relationships reached statistical significance.
Follow-up angiographic occlusion
The mean duration of imaging follow-up was 16±12 months. Forty-five patients did not have follow-up imaging available for review, most commonly because follow-up imaging was performed at an outside hospital and unavailable for direct review. Among patients in whom follow-up imaging was available (n=194, table 3), complete occlusion was observed in 72% of all stent assisted cases while a residual neck persisted in 19% and aneurysm filling was observed in 8.5%. The ‘coil through’ stenting technique was associated with the lowest rate of complete occlusion on follow-up (Raymond 1: 44/76; 57.9%) and the highest rate of residual aneurysm neck filling on follow-up imaging (Raymond 2: 22/76; 28.9%). This was related to a lower likelihood of complete occlusion on initial treatment (21/76; 27.6%). All other techniques had equivalent rates of achieving complete occlusion on follow-up imaging. There was a significantly higher likelihood of having residual aneurysm filling on follow-up imaging in the ‘jailing’ versus ‘balloon stent’ group (13.2 vs 2.5%; p=0.01). With respect to durability of initial angiographic occlusion, the ‘coil through’ technique had a significantly lower rate of initial Raymond 1, remaining completely occluded on follow-up imaging compared with ‘balloon stent’ (p<0.001) and ‘jailing’ (p=0.003).
Immediate and follow-up angiographic results according to the Raymond classification for each of the four stent assisted coil embolization techniques
Discussion
We have reviewed our contemporary experience with employing stents as adjuncts to coil embolization of intracranial aneurysms. Specifically, we studied the four main techniques employed at our institution (‘coil stent’, ‘jailing’, ‘coil through’ and ‘balloon stent’) with respect to technical and neurological complications and aneurysm occlusion rates on initial and follow-up imaging and coil packing density. As with all technical considerations, operator comfort level, training background and experience with different techniques will play a major factor in guiding which technique to employ. Although the overall adverse event rate of 42% may appear high, this represents any deviation from an idealized procedure and should not be mistaken for a true complication rate. This cannot be used for comparison with the microsurgical literature, as intraoperative technical challenges are not reported. By comparison, this might include clip repositioning, need for temporary clip application, frontal sinus invasion requiring exoneration or additional clips. These might even be considered routine even though they are deviations from an idealized craniotomy. Similarly, there is no intention for this to be used for comparison with the endovascular literature either. However, we chose to report all events whether they resulted in a clinical complication, technical complication or even insignificant deviations from the ideal. Unanticipated events might contribute to clinical complications, increased procedure length, premature abortion, etc, and for this reason we openly identify this for the varied techniques, making a comparison between stent assisted coiling techniques more meaningful. When considering clinical complications only, as is reported more commonly in the surgical and endovascular literature, the complication rate calculated for our series, which would include aneurysm perforations and clinically evident strokes, was 4.6%, highly comparable with the reported literature rate.11 ,19 ,20 ,26 ,27
We summarize our experience treating aneurysms with adjunctive stent deployment at a single, high volume tertiary care center with eight different interventionalists operating over this period of time.
‘Coil stent’
‘Coil stent’ represented the least frequently employed technique and is the strategy most likely to have been unanticipated. In the majority of cases, stent deployment was preceded by unassisted coiling as the primary method of aneurysm obliteration. Stents were then deemed necessary in the event of an unstable growing coil mass or coil loop prolapse into the parent vessel. Thus it is not surprising that this method was associated with the highest risk of thrombotic complications, including clot formation on the coil mass. This technique also had the highest rate of in-stent thrombosis which could be related to the fact that pre-procedure pharmacologic platelet inhibition was not anticipated and may not have been immediately therapeutic. A limitation of this study is that due to its retrospective nature, the exact number of planned versus unintended coil stent cases cannot be determined. This technique was employed in a uniform minority fashion across all aneurysm types. Although it had a relatively low rate of complete occlusion on initial treatment, it was as effective as any other in achieving a follow-up Raymond 1 classification. It can be conceptualized as a stent across the parent vessel holding a relatively oversized coil mass within the confines of the aneurysm.
‘Jailing’
This technique was also used more infrequently than ‘balloon stent’ and ‘coil through’. This strategy has the advantage of affixing or ‘pinning’ the microcatheter between the outer confines of the stent and the lining of the parent vessel. This achieves a more stable microcatheter position within the aneurysm and theoretically minimizes the risk of premature kick back of the microcatheter out of the aneurysm during coil deployment. Perhaps it is for this reason that ‘jailing’ was associated with the highest rate of complete occlusion at the time of treatment although the rates of complete occlusion on follow-up were comparable with other techniques. It was utilized most frequently in aneurysms arising from a curved vessel such as an OAA, presumably because of the perception that this technique results in a stable microcatheter position and that attempting to navigate through the stent, as in the ‘coil through’ technique, would be challenging or risk moving the stent while catheterizing the aneurysm. The drawback is that once the stent is deployed and the microcatheter is ‘jailed’ in place, repositioning of the tip of the microcatheter within the aneurysm during coiling is restricted to withdrawing of the catheter to a more proximal position.
‘Coil through’
This was the most commonly employed technique. The drawback to this strategy is that the microcatheter must be navigated between the tines of the deployed stent to access the aneurysm. Not surprisingly, it was associated with the highest rate of access difficulties, including inability to catheterize the aneurysm either on the first attempt or on attempted re-entry. It also had the highest rates of procedure abortion due to stent migration during attempted aneurysm re-catheterization. Important nuances for this particular technique include selection of open versus closed cell designed stents and microcatheter outer diameters. When deployed across an aneurysm arising on the outer convexity of a curved vessel, an open cell design stent such as the Neuroform will have larger apertures to navigate through than a closed cell design stent such as the Enterprise. Microcatheters range in size and flexibility; theoretically, a more trackable microcatheter with smaller outer diameters should also pass more readily through a stent. In the event of a stent migration among our cases, further attempts to navigate through the stent were halted and the patient was brought back for coiling 6–8 weeks later to allow the stent to scar down to the intima. This possibly contributes to the inferior packing density observed compared with all other techniques and the lowest rate of complete occlusion on both initial and follow-up imaging and why it was least frequently employed in the setting of an aneurysm arising from a curved parent vessel.
‘Balloon stent’
This strategy is used to reinforce balloon assisted coil embolization and was used very commonly. The use of balloon remodeling involves the temporary inflation of a balloon across the neck of an aneurysm allowing for coil deployment into aneurysms with unfavorable neck to dome ratios. As coils are inserted, a stable three-dimensional coil structure ultimately forms, thereby holding the coil mass within the aneurysm in cases in which coil herniation into the parent vessel is a primary concern. An advantage of coil introduction with adjunctive balloon use is that the microcatheter is stabilized, preventing premature kickback in a similar fashion to the ‘jailing’ stenting technique. There are two theoretical drawbacks: first, as the microcatheter is firmly pinned within the aneurysm it prevents recoil when excessive pressure is applied on a deployed coil, thereby directing the pressure to the aneurysm dome, potentially contributing to perforation, and second, balloon inflation leads to local anterograde flow potentially risking ischemia. However, a recent meta-analysis demonstrated that while balloon use was associated with superior initial and follow-up angiographic occlusion rates, there was not an increased risk of either intraprocedural aneurysm perforation or ischemic events compared with unassisted coiling.28 Balloon inflation can be performed intermittently, allowing reperfusion of the distal vascular territory in addition to unconstrained manipulation of the microcatheter within the aneurysm itself, even after coiling has been initiated. For this reason, this technique was associated with fewer difficulties repositioning the microcatheter during the embolization.
Stents provide mechanical support of the coil mass, may serve as flow diverters and provide a scaffold for endothelial growth and vessel healing. Once balloon assisted embolization is complete, the balloon catheter must be withdrawn and a stent delivery catheter must be navigated distal to the aneurysm in preparation for deployment of the stent across the neck. These added procedural steps, in particular movement of catheters back and forth across a broad aneurysm neck that has been packed with coils, could theoretically result in a risk of mechanical coil related complications such as inadvertently dragging coils into the parent vessel. However, we did not find an increased risk of coil related complications with this technique.
The ‘balloon stent’ strategy was used slightly less commonly at bifurcations, likely relating to the fact that even with a compliant balloon such as the Hyperform (ev3 Endovascular Inc, Plymouth, Minnesota, USA), a bifurcation presents a challenge to completely occlude the neck of the aneurysm. Instead, balloon inflation at a bifurcation may result in a functional narrowing of the neck with an orifice at the aneurysm shoulder. On the other hand, balloon remodeling is best suited for side wall aneurysms in which complete occlusion of the neck can be readily achieved and it is in this setting that this technique was most frequently employed.
‘Balloon stent’ has the lowest associated thrombotic complication rate and is associated with the second highest rate of complete occlusion on initial treatment and a rate of complete occlusion on follow-up comparable with the highest rate achieved by any other technique. Packing densities were superior to the ‘coil through’ technique and equivalent to the other techniques employed.
Conclusion
Balloon assisted coil embolization followed by adjunctive stent deployment across the aneurysm neck appears to be the superior technique among stent assisted coiling methods at our institution. It combines a lower rate of thrombotic and coil related adverse events with a high rate of complete occlusion on initial and follow-up imaging.
Key messages
-
There are various techniques to employ stent assisted coiling of aneurysms.
-
The ‘coil through’, ‘coil stent’, ‘balloon stent’ and ‘jailing’ techniques are four of the most commonly employed strategies.
-
Among these techniques, the balloon assisted coil embolization followed by stent deployment across the aneurysm neck (‘balloon stent’) has proven superior.
Acknowledgments
The authors are very grateful to Christine Moore for editorial proofing and help in preparation of this manuscript.
References
Footnotes
-
Competing interests None.
-
Ethics approval The Cleveland Clinic IRB approved the study.
-
Provenance and peer review Not commissioned; externally peer reviewed.