Article Text

Abstract
Background Pericallosal artery aneurysms at the bifurcation represent a special endovascular technical challenge given their distal location, commonly wide-neck morphology, small parent vessel diameter and potentially high recurrence rate after coiling given the bifurcation location. Y-configuration stent-assisted coil embolization techniques have been reported for the treatment of wide-neck aneurysms located at other vascular bifurcations and only rarely with A2 bifurcation aneurysms.
Methods A neurointerventional database was reviewed for identification of all cases of A2 bifurcation aneurysms that were treated with Y-stent configuration. The authors report clinical, technical and outcome data on four patients with pericallosal aneurysms who were treated with a Y-configuration stent-assisted coil embolization technique.
Results A Y-configuration stent placement in the anterior cerebral artery/A2 bifurcation was successfully achieved in all four patients without significant technical difficulties. One patient presented with a previously ruptured and partially treated aneurysm and three patients with incidentally found aneurysms. All four patients had a Y-configuration stent placement in one setting. The Y-configuration allowed for complete occlusion of all four aneurysms with no recurrence or arterial occlusion on mean angiographic follow-up of 13.5 months (6–28).
Conclusion Treating wide-neck pericallosal artery aneurysms at the bifurcation with Y-configuration stent placement is feasible and effective. This technique may be considered as a therapeutic option for wide-neck aneurysms that pose a difficult technical challenge.
- Aneurysm
- angiography
- angioplasty
- arteriovenous malformation
- stroke
- brain
- thrombectomy
- balloon
- thrombolysis
- artery
- complication
- catheter
Statistics from Altmetric.com
- Aneurysm
- angiography
- angioplasty
- arteriovenous malformation
- stroke
- brain
- thrombectomy
- balloon
- thrombolysis
- artery
- complication
- catheter
Background
Pericallosal artery aneurysms are relatively uncommon, accounting for 2–9% of all intracranial aneurysms.1–4 Because of their distal location and small parent vessel diameter size, pericallosal aneurysms pose a technical therapeutic challenge for endovascular therapy, with potential high recurrence rate as seen in most bifurcation cerebral aneurysms.5
Pericallosal artery aneurysms represent a special challenge for microsurgical clipping given the difficult exposure via an interhemispheric approach, interhemispheric adhesions, difficulty in controlling the parent artery and the unfavorable orientation of the aneurysm fundus.6
Endovascular therapy emerged as a promising therapeutic technique for aneurysms at this location. Early reports described the technical challenge in reaching the distal location given the tortuous and limited supportive access systems.7 The introduction of new microcatheter and microwires improved the ability to reach distal cerebral arteries and treat small aneurysms.6 The advent of stent-assisted coil embolization has also improved the endovascular management of complex intracranial aneurysms and has been used successfully in pericallosal aneurysms.8 ,9 The advantage of stent-assisted coiling with one or two stents (Y) provides the potential benefits of flow diversion and increase in metal density at the aneurysm neck, which may reduce the likelihood of aneurysm recurrence. Y-configuration stent-assisted coil embolization techniques have been described in multiple case reports and case series for the treatment of wide-neck aneurysms.10–12 However, placing overlapping stents in a Y-configuration is rare in more distally located aneurysms originating from smaller diameter size vessels.
We report four cases of wide-neck anterior cerebral artery (ACA) bifurcation aneurysms (pericallosal-callosomarginal bifurcation aneurysm) treated with Y-configuration stent-assisted coil embolization. Using a Y-configuration in coil embolization for treating pericallosal-callosomarginal aneurysm was reported in a single case report by Rohde et al in 2010.13 To our knowledge, this is the largest case series using Y-configuration stent-assisted coil embolization in treating pericallosal-callosomarginal aneurysms.
Technique
All unruptured aneurysms and re-embolization patients were treated with aspirin 325 mg daily and clopidogrel 75 mg 1 week prior to the procedure. All procedures were performed under general anesthesia with the patients in a supine position. For every protocol, patients were systemically heparinized to maintain an activated clotting time (ACT) level of 250–300 s. A Neuron (0.070) guide catheter (Penumbra Inc, San Leandro, California, USA) was placed in the petrous segment of the internal carotid artery ipsilateral to the aneurysm. Subsequently, an Excelsior SL-10 microcatheter (Boston Scientific, Natick, Massachusetts, USA) was advanced over a Synchro-2 (0.014″) microwire and positioned distal to the aneurysm neck (Boston Scientific). Next, the microwire was removed and an exchange length Transcend 300 Floppy microwire (Boston Scientific) was introduced. The microcatheter was then removed and a Neuroform stent (Boston Scientific) appropriately sized to the vessel was prepared in a standard fashion and then advanced over the exchange length microwire into the callosomarginal or pericallosal branch. The first stent was deployed across the aneurysm neck. Similar steps were performed to access the other branch crossing the first stent struts. The initial plan was to attempt aneurysm neck remodeling with a single stent; however, unstable coil positioning within the aneurysm required a second stent in a Y-configuration to allow safe detachment. The first stent was appropriately sized to the vessel diameter and the second stent was sized slightly larger to ensure adequate radial force at the point of stent intersection and wall apposition. Subsequently, the SL-10 microcatheter (Boston Scientific) was advanced over a Synchro-2 (0.014″) microwire to access the aneurysm lumen through the stent struts (figure 1). After positioning the microcatheter in the aneurysm, lumen detachable coils were used to occlude the aneurysm.

Lateral projection digital subtraction angiogram (A) and representative illustration (B) of Y-configuration stent implantation for coil embolization of a pericallosal-callosomarginal artery bifurcation aneurysm.
Patients
This is a retrospective review of a prospectively collected database. Local ethics board approval was obtained. We report four patients with pericallosal aneurysms who presented to our facility between January 2009 and August 2010.
Four pericallosal aneurysms in four patients were included in our series (table 1). The age ranged between 47 and 60 years; three of the patients were women. One aneurysm was found incidentally, and was treated previously; however, imaging follow-up showed recanalization; another aneurysm was previously ruptured and partially treated after subarachnoid hemorrhage, and one case was identified after intraparenchymal hemorrhage secondary to an arterio-venous malformation. Alternatives were offered to the patients including observation and close monitoring versus microsurgical intervention and endovascular treatment was felt to be the best option given the patient comorbidities, aneurysm location and patient's preference.
Patients and aneurysm characteristics
All four aneurysms were at the pericallosal-callosomarginal bifurcation and were treated with Neuroform stents (Boston Scientific Corporation) using a Y-configuration technique to provide stability of the coil mass, flow diversion and higher metal density at the aneurysm neck to promote endothelialization.
A Y-configuration stent placement in the ACA bifurcation was successfully achieved in all four patients without significant technical difficulties. Two events occurred in our case series. Coil migration in case 2 and coil herniation and thrombus formation in case 4, which was treated with an intravenous infusion of Abciximab with complete resolution of the thrombus. These events led to the decision of using the Y-configuration stent to manage the complications and to prevent further events. None of the patients developed any symptomatic neurological deficit. Mean clinical and imaging follow-up was 13.5 months (6–28 months) (table 2). Clinically, patients remained stable with no changes in clinical examination. Angiogram follow-up was performed on three of the four patients and 1-year magnetic resonance angiography (MRA) follow-up was performed on all four patients. Imaging follow-up showed complete occlusion of the pericallosal aneurysm according to Raymond criteria without residual aneurysm or recanalization and with preserved patency in the Y-configuration stent showing no significant in-stent stenosis or intimal hyperplasia (figure 2).

{kind=link}
{kind=link}
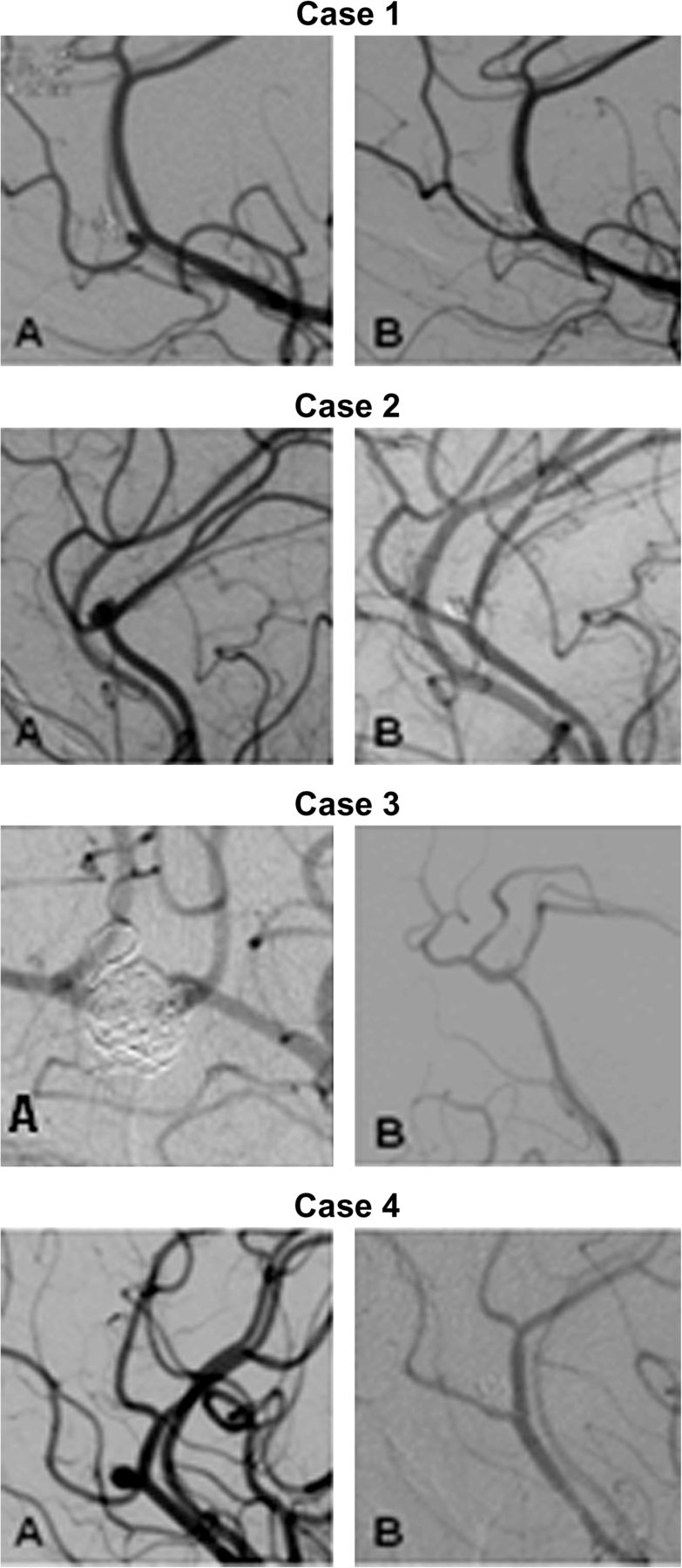
Cerebral angiography of all four cases showing the pericallosal artery aneurysm before treatment (A) and after a Y-configuration stent implantation with coil embolization (B).
Immediate results and imaging follow-up
Discussion
We report the use of Y-configuration stent-assisted coil embolization for the treatment of pericallosal-callosomarginal artery bifurcation aneurysms. This aneurysm location poses technical challenge due to coil instability at the bifurcation, an often small aneurysm size, difficulty with stent navigation and small caliber parent vessel size.
Pericallosal aneurysms are relatively uncommon.1–4 They are usually small in size and are associated with multiple cerebral aneurysms more frequently than other intracranial aneurysms. They result in intracerebral hemorrhage in more than one-half of cases when ruptured.3 As a result, patients with pericallosal artery aneurysms were reported to have a higher morbidity and mortality when compared with patients with other supratentorial aneurysms.1 Endovascular treatment for pericallosal aneurysms is complex, given their small sizes, relatively wide neck, distal location and small caliber of the parent artery.3 Aneurysms with branches originating close to the base, such as pericallosal-callosomarginal bifurcating aneurysms might represent more technical difficulties. Early case series of coiling ruptured pericallosal aneurysms reported low success rates and high technical difficulty.3 ,7 Pierot et al reported a coiling success rate of only 25% (two of eight patients) and concluded that endovascular therapy was at best an adjunct to surgery.7 Nearly a decade ago, Menovsky et al reported 100% success rate in treating pericallosal aneurysms with endovascular techniques and attributed the success to the development of new microcatheters and microwires.6 Subsequent case series reports have similar technical success rates, which are likely in part due to continued advances in endovascular devices and techniques.5 ,9 ,14 ,15 The most recent case series (Vora et al) reported good technical and clinical outcomes comparable with good surgical results.9
The availability of balloon and stent assistance has increased the endovascular options for wide-neck lesions. Hypercompliant balloons for temporary parent vessel occlusion are smaller and exhibit increased trackability; which may also improve safety in coil embolization of distal vessel aneurysms. We report an additional option for safe and effective treatment of technically challenging ACA aneurysms. Y-configuration stent-assisted coil embolization has been reported in multiple case reports and case series for the treatment of wide-neck aneurysms located at a vascular bifurcation.10 The purpose of Y-configuration stent implantation is to provide a scaffold across the aneurysm neck to stabilize the coil mass, change the vessels morphology with possible flow diversion and increase metal density across the neck to promote endothelialization. Y-configuration stent-assisted coil embolization has been used successfully in wide-neck aneurysms at the basilar tip10 ,11 and middle cerebral artery bifurcation10–12 and was described previously in a single case report for the treatment of a wide-neck ACA bifurcation aneurysm.13
Conceivable limitations of this technique include stent navigation into small distal vessels, stent compatibility with the small caliber of small intracranial vessels, and technical feasibility of intersecting stent implantation in small distal vessels. In our small series, we encountered only minimal stent trackability resistance consistent with what would be expected and all cases resulted in successful stent positioning as intended. Stent size compatibility is an important consideration in stent-assisted techniques in small caliber distal intracranial vessels. The average size of a pericallosal artery and callosomarginal artery is 2.5–2.6 mm.16 The smallest Neuroform stent opens to a maximal diameter of 2.5 mm and per manufacture recommendations can be used in vessels as small as 2 mm. We experienced no difficulty in stent size compatibility within the vessels and achieved good angiographic wall apposition of stent tines in all cases. Intersecting stent implantation also poses technical challenge related to strut microcatheterization. Intracranial stent interstices opening size can range from approximately 2 Fr to 2.5 Fr (Boston Scientific Corporation). Difficulty in microcatheter access through these narrow interstices will be present in positioning of the second stent, as well as at the time of aneurysm catheterization. In our series, multiple microwire passes were needed for trans-strut catheterization in one case and for trans-strut aneurysm catheterization in another case; ultimately this did not limit success in stent positioning or coil delivery. An adjunctive technique could be jailing of a microcatheter into the aneurysm fundus with the first stent to avoid difficulty with trans-stent catheterization after stents have been deployed.
Adverse events during primary coil embolization in two of the cases led to the decision to use Y-configuration stent-assisted embolization. Coil migration in case 2 and coil herniation into the parent vessel with thrombus formation in case 4. All cases had successful stent implantation and trans-stent aneurysm embolization. Overall, there were no clinical complications related to the stent technique.
Two of the four patients had follow-up with digital subtraction angiography which demonstrated complete occlusion of the pericallosal aneurysm without residual aneurysm or recanalization and showed no evidence of significant intimal hyperplasia or in-stent stenosis. One of the four patients could not have a digital subtraction angiography given his complicated medical co-morbidity, which was the initial reason of choosing endovascular therapy over microsurgery. Another patient did not have an angiographic follow-up as per her preference. A non-invasive follow-up with MRA was performed on all four patients and showed stability of the coil mass without neck residual or recanalization and preserved patency of the parent vessel. Although MRA provides limited data on mild to moderate in-stent stenosis, it provides good data about recanalization of the aneurysm and for excluding vessel occlusion.
Conclusions
We report the application of Y-configuration stent implantation for coil embolization of pericallosal-callosomarginal artery bifurcation aneurysms. This series demonstrates feasibility of this technique in small caliber distal intracranial vessels harboring small aneurysms that pose challenge for endovascular therapy.
References
Footnotes
-
Competing interests None.
-
Ethics approval Ethics approval was provided by the institutional review board of the Medical College of Wisconsin.
-
Provenance and peer review Not commissioned; externally peer reviewed.