Article Text

Abstract
Physician spending is complex and intrinsically related to national health care spending, government regulations, health care reform, private insurers, physician practice and patient utilization patterns. Consequently, since the inception of Medicare programs in 1965, several methods have been used to determine the amounts paid to physicians for each covered service. The sustainable growth rate (SGR) was enacted in 1997 to determine physician payment updates under Medicare part B with an intent to reduce Medicare physician payment updates to offset the growth and utilization of physician services that exceeds the gross domestic product growth. This is achieved by setting an overall target amount of spending for physicians' services and adjusting payment rates annually to reflect differences between actual spending and the spending target. Since 2002, the SGR has annually recommended reductions in Medicare reimbursements. Payments were cut by 4.8% in 2002. Since then, Congress has intervened on 13 separate occasions to prevent additional cuts from being imposed. This manuscript describes certain important aspects of the 2012 physician fee schedule.
Statistics from Altmetric.com
Introduction
On July 6, 2011, the Centers for Medicare and Medicaid Services (CMS) issued its proposed changes to the 2012 Medicare physician fee schedule, including a long feared plan to cut Medicare pay to physicians by 30%.1 CMS is required to issue the fee schedule based on current payment rules using the sustainable growth rate (SGR) formula now in effect. As of July 6, 2011, physicians were scheduled for a nearly 30% decrease in reimbursement beginning in 2012. Apart from the proposed cuts, the rule also included various other measures to reduce Medicare expenditures. Subsequently, in November 2011, payment policies under the physician fee schedule and other revisions to part B for 2012 were published with a comment period of January 3, 2012.2 However, the projected 30% payment cut for physicians from Medicare was reduced to 27.4%.
The Medicare Payment Advisory Commission (MedPAC), the National Commission on Fiscal Responsibility and Reform and the debt commission provided multiple recommendations on physician payment fix—that is, a permanent correction of the fatally flawed SGR formula.1 However, none of the proposals was accepted. Towards the end of 2011, Congress agreed to a temporary 2 month SGR fix. The final passage with a price tag of $20 billion extends the fix for the remaining 10 months.
The physician payment system is complex and intricately related to national healthcare spending, government regulations, healthcare reform, private insurers, physician practice patterns and patient utilization patterns. This manuscript will review various aspects of physician payments and changes published in the revised 2012 CMS schedule.2–12
Physician payment system
According to MedPAC,13 as of October 2011, among the 1 million clinicians in Medicare's registry, approximately 50% are physicians who actively bill Medicare. Payments for physicians' services were approximately $62 billion in 2010, accounting for 12% of total Medicare spending. MedPAC data also show that in 2009, almost all (90%) of the beneficiaries enrolled in Medicare fee for service received at least one physician service, based on a list of services and their payment rates—physician fee schedule, physician services include office visits, surgical procedures and a broad range of other diagnostic and therapeutic services, furnished in all settings, including offices, hospitals, surgical centers, skilled nursing facilities and various other settings, including beneficiaries' homes.3 ,5 ,8 ,13
In determining payment rates for each service on the fee schedule, CMS considers the (1) amount of work required to provide that service, (2) expenses related to maintaining a practice and (3) liability insurance costs. The value of the three components are adjusted on a yearly basis with a combination of total multiplied by a standard dollar amount, called the fee schedules conversion factor, which was $33.98 in 2011, to arrive at the payment amount. This factor will stay the same unless the 27.4% cut of the SGR takes place or CMS enacts further reductions.
Since the inception of Medicare programs in 1965, several methods have been used to determine the amounts paid to physicians for each covered service. Initially, payment systems compensated physicians on the basis of their charges and allowed physicians to balance their books by billing beneficiaries for the full amount above what Medicare paid for each service, which was short lived. In 1975, just 10 years after the inception of the Medicare program, payments changed so as not to exceed the increase in the medical economic index.1 ,14 ,15 This policy failed to curb increases in costs, leading to the determination of a yearly change in fees by legislation from 1984 to 1991.
Since January 1, 1992, Medicare has paid for physicians' services based on national uniform relative value units (RVUs), based on the relative resources used in furnishing services. The national RVUs are established for physician work, practice expenses (PE) and malpractice expense.1 ,13–15 Since 2009, CMS has been reviewing the rates annually under the agency's potentially misvalued service initiative.1 ,3 ,4 ,15 This annual review impacts some specialties far more than others—for example, radiology. Finally, adjustments to RVUs are required to be budget neutral. Budget neutrality is based on physician work, PE and liability insurance component and are represented as 52.5%, 43.6% and 3.9%.1 ,3 ,4 ,15
Sustainable growth rate
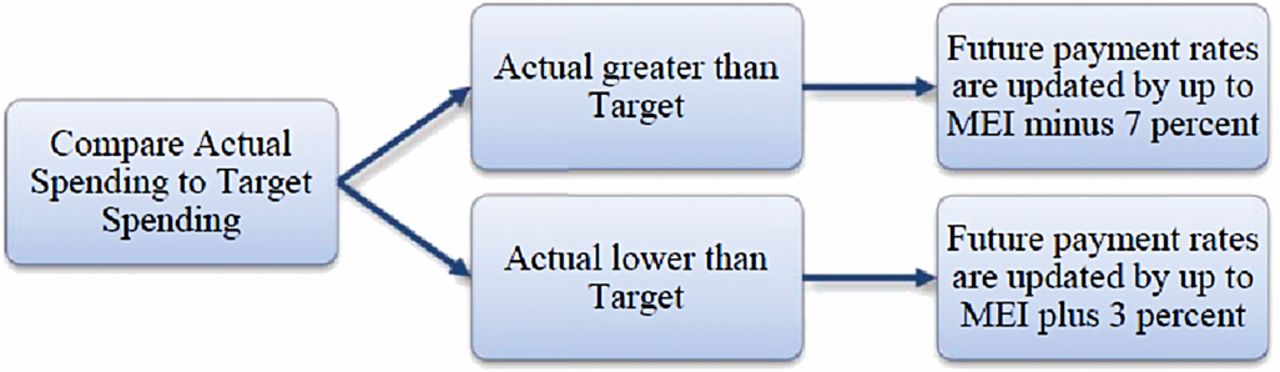
The SGR was enacted in 1997 to determine physician payment updates under Medicare part B. The intent was to reduce Medicare physician payment updates to offset the growth and utilization of physician services that exceed the gross domestic product (GDP) growth.16 This is achieved by setting an overall target amount of spending for physicians' services and adjusting payment rates annually to reflect differences between actual spending and the spending target. The target is the product of the growth in fee for service enrollment; inflation based update factors; real GDP per capita; and changes in law or regulation. Actual growth and spending on physician services is compared with a cumulative target growth rate linked to GDP, using 1996 as the base year. The formula also limits the amount of an increase in payment rates to inflation plus 10% and it limits a decrease in payment rates to inflation minus 7%, as illustrated in figure 1, with inflation being measured by the Medicare Economic Index (MEI). MEI measures changes in the costs of physicians' time and operating expenses; it is awaited some of the prices of inputs in those two categories. Changes in the cost of physicians' time are measured using changes in non-form labor costs and changes in ‘all factor’ productivity. However, since 2002, spending measured by the SGR has consistently been above the targets established by the formula, requiring future payment reductions.16 The formula limits these future reductions to MEI minus 7%, thus excess spending will take many years to be recaptured.

Comparison of actual spending to target spending. Source: Medicare's payments to physicians: the budgetary impact of alternative policies. Congressional Budget Office, June 14, 2011.16 http://www.cbo.gov/ftpdocs/122xx/doc12240/SGR_Menu_2011.pdf. MEI, Medicare Economic Index.
Despite congressional interventions to set aside steep SGR mandated physician payment cuts, utilization growth in recent years has been relatively low although very unpredictable. As illustrated in figure 2, at the inception of SGR in the late 1990s, annual volume/intensity growth in Medicare physician fee services ranged from 1.9% to 2.9%. The growth accelerated in 2000 and 2001, reaching a plateau during 2001 to 2004, with annual growth ranging between 4.6% and 5.8%. The deceleration of growth started in 2005, ranging from 3% to 3.7% from 2006 to 2009, and dipping to 2.4% in 2010.1

Trends in volume growth since sustainable growth rate inception. Source: Statement of the American Medical Association before the House Energy and Commerce Committee Subcommittee on Health Presented by Cecil B Wilson, MD, May 5, 2011. MFS, Medicare physician fee.
Since 2002, the SGR has annually recommended reductions in Medicare reimbursements. Payments were cut in 2002 by 4.8%.1 ,3 ,15 Since then, Congress has intervened on 13 separate occasions to prevent additional cuts from being imposed. In 2003, there was a proposed cut of 4.4%.1 ,3 ,15 However, Congress intervened and averted the projected 4.4% cut and increased the payment for physician services by 1.6%.1 ,3 ,15 In 2004 and 2005, with the enactment of the Medicare Modernization Act, scheduled rate reductions were replaced with an increase of 1.5%.1 ,3 ,15 The Deficit Reduction Act in 2006 held 2006 payment rates at their 2005 level, overriding an additional impending 4.4% reduction.1 ,3 ,15 In 2007, Congress again approved holding the 2008 payments at the 2005 level, thereby avoiding a proposed additional 5.1% reduction.1 ,3 ,15 Since then, multiple measures were applied repeatedly. In 2010 alone, five separate bills were passed to stop a 22% cut.1 ,3 ,15 On 13 occasions, Congress has not provided the funding necessary to reform the flawed SGR formula, resulting in steeper cuts in subsequent years. Consequently, the 10 year cost of a long term solution has grown from $48 billion in 2005 to nearly $300 billion today, and it is expected to grow another 5%, resulting in an approximately 35% cut in 2013.17
Medicare spending on physician services
Medicare spending for fee for service for beneficiary for physician services has increased annually. During the 10 year period ending in 2009, Medicare spending for physician services—per beneficiary—increased 61%. However, during the 10 year period from 2000 to 2010, spending for fee schedule services grew from $37 billion in 2000 to $64 billion in 2010—an increase of 72%. Thus Medicare spending on physician services has been described as growing much more rapidly over this period than both the payment rate updates and the MEI.17 However, this may be arguable. Overall physician fee schedule payment updates totaled 7% during the 10 year period ending in 2009 whereas the MEI increased 20%. Thus the contributions of growth are secondary to growth in volume of services than payment rate updates. Both factors (namely updates and volume growth) combined to increase physician payments and expenses for Medicare.
The volume of physician services per beneficiary has continued to grow from year to year, with some services growing much more than others. As shown in figure 3 from 2002 to 2009, the volume of physician services grew by 47%. However, by specific types of services, imaging, tests and other procedures (procedures other than major procedures) each grew at a rate of 65% or more.17 The comparable growth rates for major procedures and evaluation and management services were 34% and 32%, respectively. However, the volume growth results show some positive trend.

{kind=link}
{kind=link}
{kind=link}
Continued growth in volume of physician services per beneficiary, 2000–2009. Source: National Healthcare and Medicare Spending. In: A data book: healthcare spending and the Medicare program. MedPAC, 2010:3–17.17 http://www.medpac.gov/chapters/Jun10DataBookSec1.pdf
Analysis of 2012 Medicare physician payment schedule
In November 2011, the Medicare physician payment ‘final rule’ of 2012 was released.2 This 1235 page document, despite its name, is still undergoing revisions. As the length of the final rule document suggests, the authors of this manuscript need to be selective in what points are to be covered in this analysis. MedPAC18 and the American Medical Association (AMA)19 provided detailed analysis of the proposed rule and with final comments from AMA on the final rule.1
The American Society of Neuroradiology (ASNR), where one of the authors of this article is the Relative Value Update Committee (RUC) advisor, in its analysis of the final rule focused on:
-
The expansion of the Multiple Procedure Payment Reduction (MPPR) rule to the professional component of advanced diagnostic imaging.
-
The physician work for CT spine codes (72125, 72128 and 72131).
-
The physician work for kyphoplasty and vertebroplasty codes (22520-22525).
Separately, ASNR had commented on the Physician Quality Reporting System (PQRS) Radiology Measures Group in its comment on the proposed rule submitted in August 2011.
Potentially misvalued services under the physician fee schedule
This issue was addressed by MedPAC, as well as AMA. Misvalued codes can be a major drain on Medicare revenues and also cause substantial impact to practitioners. The Affordable Care Act includes a section addressing the identification of potentially misvalued services, the collection of data to facilitate appropriate adjustments and validation of RVUs.4 In addition, CMS is required to review and revise the relative ranking of all physician services at least every 5 years. Further, CMS also annually assigns values to new services, adjusts ranking for certain existing services and makes other changes to the physician fee schedule. CMS has historically followed recommendations from the AMA specialty society RUC, and others in making these changes.
The proposed physician payment schedule for 2011 addresses identifying, reviewing and validating the RVUs of potentially misvalued services under the fee for services. The issue of potentially misvalued services dates back to March 2006 to the report of MedPAC which noted that misvalued services can distort the price signals for physicians' services, as well as for other healthcare services that physicians order, such as hospital services.2 ,20 ,21 The reasoning provided for misvalued codes was that when a new service is added to the physician fee schedule, it may be assigned a relatively high value because of the time, technical skill and psychological stress that are often required to furnish that service. Over time, the work required for certain services would be expected to decline as physicians become more familiar with the service and more efficient in furnishing it. Thus the amount of physician work needed to furnish an existing service may decrease when new technologies are incorporated. Further, services can also become overvalued when PEs decline. This can happen when the cost of equipment and supplies fall, or when equipment is used more frequently, reducing its cost per use. Likewise, services can become undervalued when physician work increases or PEs rise. Thus, CMS and AMA RUC have taken increasingly significant steps to address potentially misvalued codes.
Expanding the multiple procedure payment reduction policy
When outpatient therapy or surgical services are furnished to the same patient on the same day, Medicare reduces payments for the second and subsequent procedures to account for efficiencies and PE, and pre- and post-surgical physician work. Since the Deficit Reduction Act, CMS reduces payments for the technical component of multiple imaging studies that are performed in the same session (the technical component includes the cost of the non-physician staff who perform the test, medical equipment, medical supplies and overhead expenses). CMS proposed to expand this policy, generally known as MPPR, to the professional component of certain imaging services which includes physicians' work involved in interpreting the studies' results and writing a report. When multiple CT, MRI or ultrasound services are performed in the same session, CMS would reduce payment for the professional component of the second and subsequent services by 50%. In the 2012 final rule, CMS retreated from this 50% cut but stated that it would implement the expansion of the MPPR with a 25% reduction to the professional component of second and subsequent advanced diagnostic imaging services administered to the same patient, by the same physician (or physician group), during the same session, on the same day. This proposal is based on the supposed efficiencies in physician work that occur primarily in the pre- and post-service periods when multiple services are performed in the same session. This policy is meant to be consistent with the current MPPR that applies to the technical components of multiple imaging services. The majority if not all imaging based organizations have taken great exception to this characterization, arguing that the relative efficiency on the professional side is nominal. Indeed, the ASNR comment on the final rule stated that “the proposed MPPR expansion is a manifestation of CMS attempting to circumnavigate the functions of the AMA RUC” where care has been taken to individually determine the value of these codes over a multi-year period. Consequently, CMS also proposes to extend its current MPPR policy to the physician interpretation of 119 imaging codes that are already subject to an MPPR for the procedure (technical component itself). In addition, the agency is considering additional policies that would make up to 700 diagnostic services subject to MPPR cuts and that would include common, low cost tests such as x-rays. Government Accountability Office, MedPAC and the AMA Specialty Society RVC (Relative Review Committee) Update Committees have worked on this issue and CMS is utilizing their work to justify these changes. ASNR believes that these recommendations are based on flawed assumptions. AMA calls that this analysis oversimplifies related to Government Accountability Office and MedPAC recommendations, misconstrues the findings of the RUC, overlooks relevant CMS data and results in a proposal that is likely to increase costs to Medicare and its beneficiaries while also further fragmenting medical care.
CMS projected savings of $100 million a year from its proposal. AMA also commented that imaging services performed in physician offices have been subjected to substantial cuts over the past several years, and between 2006 and 2013, some will experience payment cuts of more than 60%. AMA's analysis of 2010 Medicare claims data suggests that advanced imaging services are already shifting from physician offices to hospital outpatient department settings, and a new round of payment cuts seems likely to intensify the trend.
In response to comments from the RUC and many specialties, CMS scaled back its proposal to apply a reduction to the professional component of all but the highest valued codes when more than one procedure on a list of 119 imaging services is performed on the same patient on the same day. However, CMS did not agree with the comments that across the board multiple procedure cuts are inappropriate because the degree of overlapping work associated with these cases varies from service to service. Finally, per above, instead of a 50% reduction, the final rule limits the MPPR on 119, CT, MRI, MR angiogram and ultrasound codes to 25%.
Physician quality reporting system
PQRS is becoming a focal point in medical care. CMS proposed to provide interim feedback reports to physicians and other eligible professionals participating through the claims based reporting mechanisms under the PQRS for 2012 and beyond. These reports will be based on claims for dates of service occurring on or after January 1 and processed by March 31 of the respective program year. Reports will be available in the summer of the respective program year. CMS is also proposing for 2012 and beyond, to allow physicians and other eligible professionals who participate in the PQRS via the Electronic Health Record (EHR) based reporting mechanism to have the option of submitting quality measure data obtained from the PQRS qualified EHR to CMS either directly from the eligible professionals qualified EHR or indirectly from a qualified EHR data submission vendor on the EPS behalf. Physicians and other eligible professionals would be Eligible Professionals (EPs) required to have a separate PQRS qualified EHR product, despite the fact that physicians and other eligible professionals may have already purchased Certified EHR Technology for purposes of reporting under the Medicare and Medicaid EHR Incentive Programs (ie, meaningful use program).
CMS finalized its proposal to provide interim feedback reports to physicians reporting individual measures and measure groups through claims based reporting for 2012 and beyond. These reports will be a simplified version of the annual feedback report that CMS currently provides and will be based on claims for the first 3 months of each program year. The interim feedback reports will be provided to physicians during the summer of each program year. Despite strong opposition from the physician community, CMS finalized its proposal to use 2013 as the reporting period for the 2015 PQRS penalty. If CMS determines that a physician or group practice has not satisfactory reported quality data for the 2013 reporting period, then its 2015 payments will be reduced by 1.5%.
Conclusion
We believe 2012 represents a time of prescient change in American medicine. Rosy scenarios portray US economic growth as limited with real potential for setbacks to our fledgling recovery. What seems certain is that there will be continuing pressures to lower the cost of providing medical services. Physician reimbursement represents a compelling target for policy makers. Neurointerventionalists should be familiar with ongoing discussions regarding physician reimbursement.
Acknowledgments
The authors thank Sekar Edem for assistance in the search of the literature, Tom Prigge, MA, for manuscript review and Tonie M Hatton and Diane E Neihoff, transcriptionists, for their assistance in the preparation of this manuscript.
Footnotes
The manuscript is a brief version of Manchikanti L, et al. Physician payment outlook for 2012: Déjà Vu. Pain Physician 2012;15:E27–E52. This version is published with the consent of all the authors and the permission of the journal Pain Physician.
-
Correction notice This article has been corrected since it was published Online First. The disclosure information on the first page has been updated.
-
Competing interests JAH is a consultant for CareFusion and serves on the Steering Committee for the KAVIAR trial (volunteer position) and the Data and Safety Monitoring Board (DSMB): CEEP trial (volunteer position).
-
Provenance and peer review Not commissioned; not externally peer reviewed.