Article Text

Abstract
Background The Penumbra system is effective for recanalization of the primary arterial occlusion (PAO) in acute stroke. However, clinical outcomes are not as promising. The authors hypothesized that the formation of procedural distal emboli (PDE) during mechanical thrombectomy may lead to poorer patient outcomes.
Design/methods A retrospective review of patients with acute ischemic stroke treated with the Penumbra system was undertaken. Patients' outcome was evaluated by comparing discharge National Institute of Health stroke scale and modified Rankin score (mRS) of patients with and without PDE.
Results Out of 20 patients reviewed, recanalization of PAO was 100%. Six patients (30%) were confirmed to have PDE, of which two died (33.3%) and one (16.7%) had mRS of 2 or less. Of the 14 patients without PDE, three died (21.4%) and six (42.9%) had mRS of 2 or less. In the patient group who survived, mean National Institute of Health stroke scale decrease was only 2.3 in patients with PDE versus a decrease of 10.6 in patients without PDE.
Conclusions In spite of PAO recanalization, distal emboli formed subsequent to Penumbra thrombectomy may contribute to poorer clinical outcome in acute stroke patients.
- Arteriovenous malformation
- blood flow
- complication
- cranial nerve
- embolic
- intervention
- liquid embolic material
- stroke
- thrombectomy
- thrombolysis
Statistics from Altmetric.com
- Arteriovenous malformation
- blood flow
- complication
- cranial nerve
- embolic
- intervention
- liquid embolic material
- stroke
- thrombectomy
- thrombolysis
Treatment of stroke using the Penumbra mechanical thrombectomy system has been effective in the recanalization of primary arterial occlusion (PAO) in acute stroke.1 ,2 Several studies have shown recanalization rates ranging between 72% and 93%.2–4 However, clinical outcomes are not as promising even with recanalization possibly from clot fragmentation and procedural distal emboli (PDE). PDE resulting from the Penumbra system were noted in 11–48% of patients in previous studies but the clinical significance of these emboli are unknown.2 ,5
We report our personal experience using the Penumbra mechanical thrombectomy system in acute stroke. We evaluated PDE and subsequent clinical outcome during hospitalization.
Methods
After obtaining institutional internal review board approval, we reviewed our acute ischemic stroke patients who underwent Penumbra mechanical thrombolysis between 1 February 2009 and 31 March 2010. In each patient, medical records were reviewed and the following measures recorded: (1) time of stroke onset and subsequent procedure start time (femoral artery puncture); (2) time to recanalize PAO; (3) the presence of PDE; (4) recanalization of PDE and end of procedure time; and (5) functional outcome measured by the National Institutes of Health stroke scale (NIHSS) and modified Rankin score (mRS).
All interventional procedures were performed under general anesthesia. The Penumbra mechanical thrombectomy system (Penumbra, California, USA) was performed using a six French shuttle sheath. Penumbra aspiration catheters were selected for the largest size suitable for the treating artery. The largest possible Penumbra aspiration catheter (041, 032, 026) and separators at the time were utilized for more effective aspiration thrombectomy. Echelon 14 microcatheters (EV3, MN) were used co-axially with the Penumbra 041 aspiration catheters. Microcatheter contrast injections were performed distal to the primary occlusion before the intra-arterial administration of alteplase (Genentech, California, USA) alternating with thrombectomy. Penumbra aspiration thrombectomy was performed proximal to the clot and advanced distally.
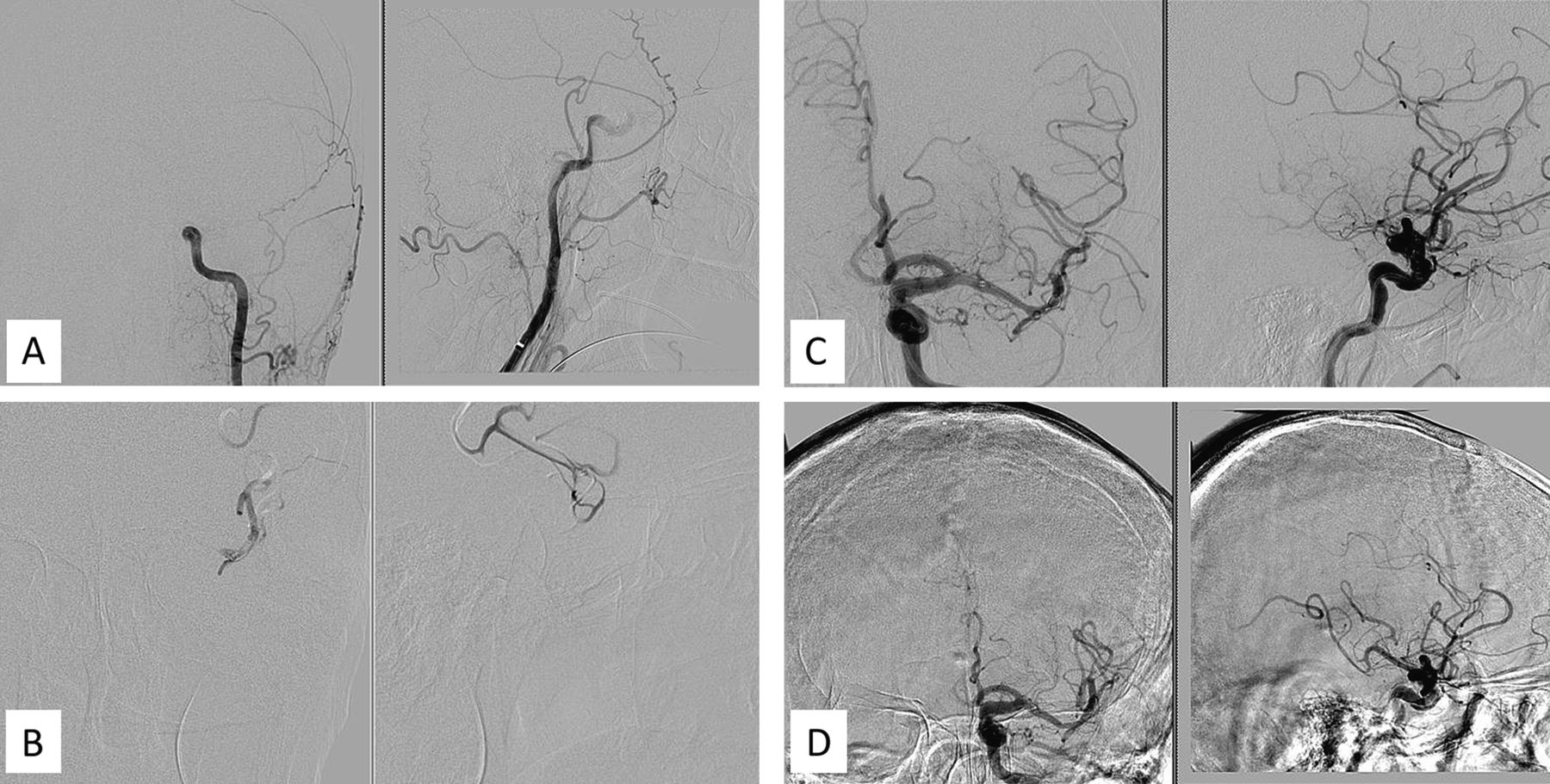
PDE was defined as emboli in an artery distal to the PAO, which was noted to be patent through an initial microcatheter contrast injection (figure 1). Initial NIHSS as well as subsequent daily NIHSS including discharge NIHSS were documented by the stroke team. Patients' degree of disability or dependence in the daily activities at discharge were assessed with mRS.
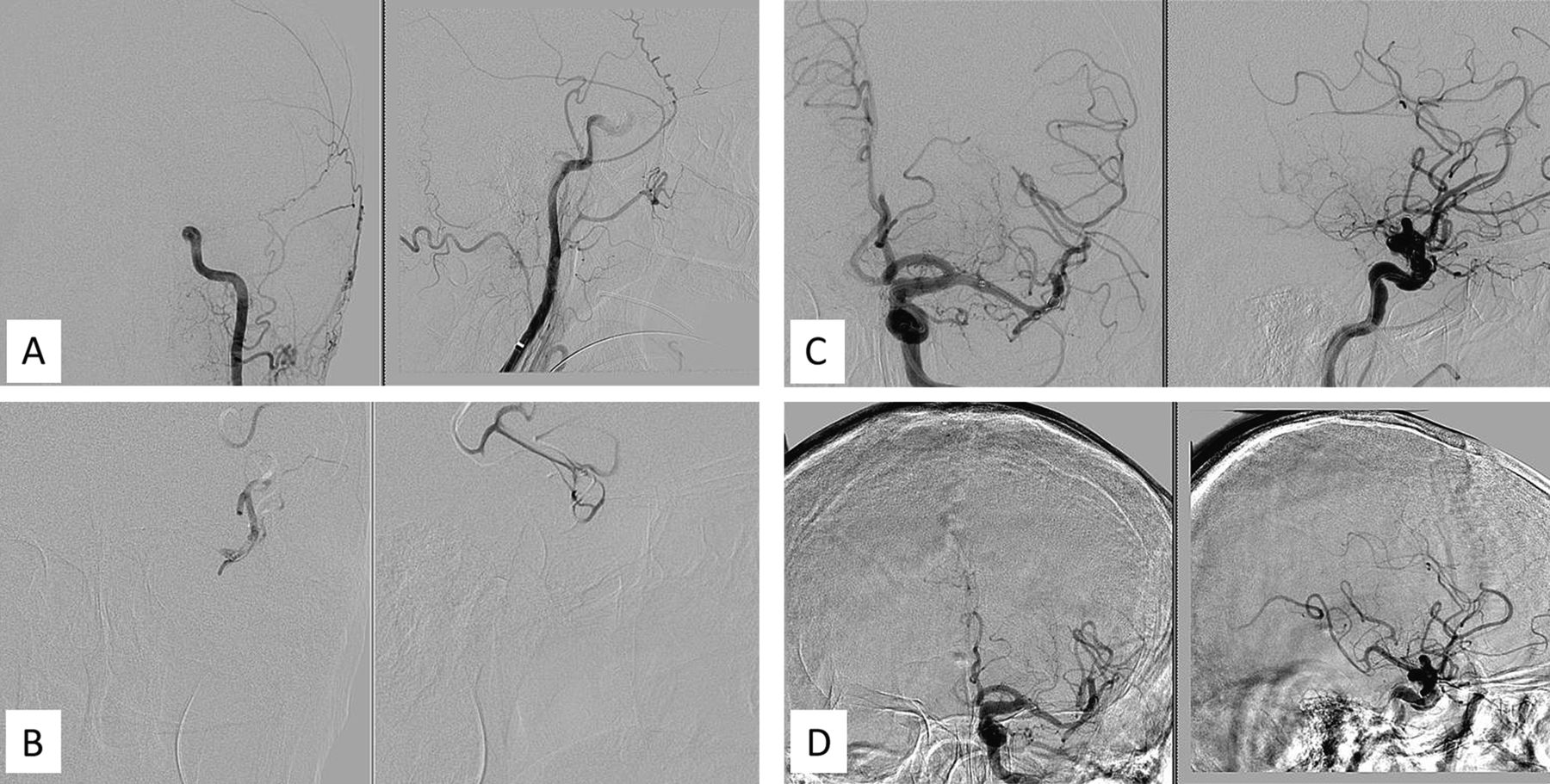
Cerebral angiography illustrating procedural distal emboli. (A) Initial angiogram demonstrates left supraophthalmic internal carotid artery occlusion. (B) Microcatheter digital subtraction angiogram demonstrates patent left posterior M2 segment branches. (C) After thrombectomy with Penumbra 041 catheter, the left posterior M2 segment is occluded with procedural distal embolus. (D) After thrombectomy with Penumbra 032 catheter, the left posterior M2 segment has recanalized with thrombolysis in myocardia infarction 3 flow.
Post-procedure CT scans were reviewed to identify patients with post-procedure intracerebral hemorrhage. Symptomatic intracranial hemorrhage (ICH) was defined as CT evidence of a bleed associated with a four-point deterioration on the NIHSS or death subsequent to the procedure.
Results
During this 14-month period, 20 patients were treated for acute ischemic stroke at our institution with the Penumbra mechanical thrombectomy device by a single neurointerventional radiologist. The mean age of patients was 67 years, with 11 men and nine women. The mean overall NIHSS at onset was 17.8. The site of PAO was M1 in 12 cases, internal carotid artery (ICA) in six cases, basilar artery in one case and M2 in one case (table 1).
Patient demographics, baseline stroke score, and site of PAO
Intravenous tissue plasminogen activator (tPA) was administered in five cases, with one patient (25%) associated with PDE, while of the 15 patients who did not receive intravenous tPA, five (33%) were associated with PDE (table 2). Intra-arterial tPA doses ranged from 2 mg to 20 mg, except for one case of 50 mg given to a patient evaluated within 3 h from acute stroke onset who had not received intravenous tPA (a decision was made to attempt mechanical thrombectomy directly because the patient was reaching the end of the 3-h window).
Comparison of patients with and without PDE
Recanalization of the PAO with a thrombolysis in myocardial infarction score6 of 3 was achieved in all cases. The overall mean time to recanalization from onset of symptoms was 351.2 min, with an average of 348.1 min among patients without PDE and 358.5 min among patients with PDE. The average procedural time to recanalize PAO was 52.9 min and was similar in patients with and without PDE. PDE were noted in 30.0% (6/20) of patients (table 2). The mean additional procedure time required to recanalize PDE was 45.8 min.
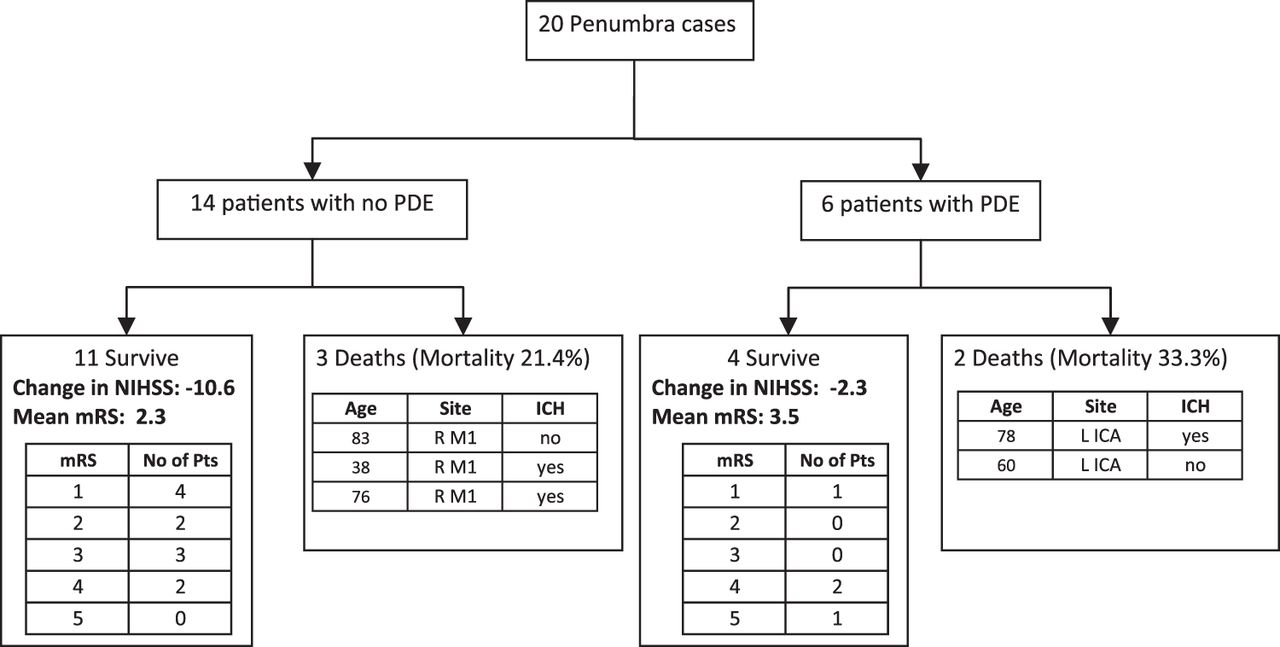
Clinically, a mean NIHSS decline of 10.6 points was noted in patients without PDE compared with only a 2.3 point decline in patients with PDE. Overall, 35% (7/20 patients) had mRS of 2 or less before discharge, with 42.9% (6/14) in patients without PDE and 16.7% (1/6) in patients with PDE. Patient outcome in relation to PDE is summarized in figure 2. Intravenous tPA did not appear to be positively associated with good outcome (mRS <2) at hospital discharge. Only one out five patients (25%) who received intravenous tPA had mRS less than 2 while six out of 15 patients (40%) who did not receive intravenous tPA had mRS less than 2. Stroke onset time to treatment was negatively associated with good outcome (mRS <2) at hospital discharge. Five out of 10 patients (50%) with thrombectomy initiated between 3–6 h from stroke onset had mRS less than 2, while only two out of 10 patients (20%) with thrombectomy initiated between 6–8 h from stroke onset had mRS less than 2. No patient had primary artery recanalization in the first 3 h of stroke onset (tables 3 and 4).

{kind=link}
{kind=link}
Overall summary of patient outcome. ICA, internal carotid artery; ICH, intracranial hemorrhage; L, left; mRS, modified Rankin score; NIHSS, National Institutes of Health stroke scale; PDE, procedural distal emboli; Pts, patients; R, right; tPA, tissue plasminogen activator.
Functional outcome according to time and PDE
Functional outcome comparing individual factors
The overall mortality rate was 25% (4/20 patients). The highest mortality was seen in patients with ICA occlusion. The mean mortality rate in patients with PDE was 33.3% (2/6) compared with 21.4% in patients (3/14) without PDE. Symptomatic ICH was seen in three patients, all of which were associated with mortality, including one patient with PDE and two patients without PDE.
Discussion
Previous studies have relied mainly on recanalization of PAO for acute stroke outcome.1–4 The multicenter Penumbra Pivotal Stroke trial documented recanalization in 81.6% of patients but only 25% of the patients have a favorable outcome (defined as a mRS of ≤2).
Our study suggests that PDE may play a significant role in clinical outcome. In this series, patients without PDE had greater NIHSS improvement and lower NIHSS and mRS at discharge from hospital. Distal emboli may affect clinical outcome by resulting in no improvement or deteriorating blood flow. Blood flow may be diminished from obstruction of collaterals either at a macroscopic or microscopic level leading to impaired reperfusion.7 Several studies suggest these collateral vessels are important in determining clinical outcome.8–10 Furthermore, the utilization of tPA, which has been shown to improve outcome with endovascular treatment, may do so by limiting PDE.9 Our results indeed showed a decreased incidence of PDE when intravenous tPA was administered (table 3).
The study has several limitations. First, this study is a retrospective chart review of a small series of acute stroke patients treated with Penumbra thrombectomy at a single center by a single operator. Because of the small number of cases involved, no statistically significant findings were noted. Second, the determination of PDE is an underestimation because we cannot conclude that all arteries distal to the PAO were visualized before thrombectomy. Therefore, the incidence of PDE with Penumbra may actually be higher than the 30% that we reported. Third, the reported rates of PDE or clot fragmentation may vary depending on the various technical procedural factors including device type, experience of the operator, and vigilance in detection. Finally, our data are limited to clinical outcome at discharge and longer term outcomes data may be more helpful in determining the effectiveness of treatment.
Further studies are needed better to measure PDE and its effects on poorer outcomes and the role of intravenous tPA. PDE are difficult to measure and generally prone to underestimation given arteries distally to primary occlusion are not well visualized. Other devices report lower PDE, with Solitaire stent retriever demonstrating a 3.4% angiographic PDE and no available statistic on PDE with MERCI retriever.11 Penumbra may result in greater clot fragmentation and therefore PDE. Standardized methods of measuring PDE are needed better to evaluate the risk of PDE.
Although intravenous tPA appears to lower the risk of PDE, it did not appear to improve clinical outcome. Our study is consistent with previous findings of poorer outcome of intravenous tPA on large artery occlusion.12 In addition, intravenous tPA was not associated with symptomatic ICH—none of the three symptomatic ICH received intravenous tPA.
Clinical outcome following endovascular treatment for acute stroke depends on multiple factors beyond recanalization of PAO within the shortest time possible. Improvements in detection, prevention, and management of PDE may narrow the observed discrepancy between the recanalization rate and patient outcome. Therefore, decreasing PDE may improve the potential clinical outcome for thrombectomy devices in acute stroke care.
References
Footnotes
-
Collaborators Marks SJ, Ahluwalia BS.
-
Competing interests None.
-
Patient consent This study was retrospective study. Deferment of patient consent was approved by the institutional review board.
-
Ethics approval Ethics approval was provided by New York Medical College Committees for Protection of Human Subjects.
-
Provenance and peer review Not commissioned; externally peer reviewed.