Article Text

Abstract
Background Advancements in technology have created a current generation of guide catheters that not only provide stable access but also allow navigation of tortuous portions of the carotid siphon facilitating more distal access. Clinical experience since the release of the current generation of guide catheters was reviewed to determine their safety and efficacy.
Methods Between October 2007 and November 2011, all neurointerventional procedures requiring access to the intracranial arterial circulation performed at our institution were reviewed. Clinical performance and complication rates of current generation guide catheters were compared with conventional guide catheters.
Results 1188 neurointerventional procedures were performed, of which 659 were eligible for this study. When navigating the anterior circulation, intracranial purchase was achieved significantly more often with current generation 0.070 inch and 0.053 inch guide catheters compared with conventional guide catheters. Similarly, current generation 0.070 inch and 0.053 inch catheters navigated at least one sharp 90° turn significantly more often than conventional guide catheters. Guide catheter related complications were encountered in 1.4% of cases with both catheter generations and differences were not significant although more complications were found when guide catheter tip position was cervical rather than intracranial.
Conclusion Current generation guide catheters allow distal access with a high rate of success while maintaining a low rate of complications. When intracranial location of the guide catheter was obtained, fewer complications occurred.
Statistics from Altmetric.com
Background
The treatment of cerebrovascular diseases continues to proliferate with improvements in technology that allow for safer and more efficacious surgeries.1 The presence of a stable guide catheter platform as close as possible to the target lesion is crucial to the success of endovascular procedures. Historically, this has been accomplished through large rigid guide catheters in the cervical cerebral arteries. Various strategies have been used traditionally to increase the stability of proximal guide, including the use of a ‘buddy wire’ maintained within the guide/sheath,2–4 coaxial double guiding catheter technique4 and alternative access from the upper limb (brachial or radial arteries2) or direct carotid puncture.5 Recent advancements in technology have created a current generation of guide catheters that not only continue to provide stable access but also facilitate navigation of tortuous portions of the carotid siphon to allow more distal access.6–11
Several case series have identified early experience with these guide catheters in an attempt to define their role in current endovascular surgeries. These catheters have been reported in the treatment of aneurysms, arteriovenous malformations, intracranial angioplasty and stenting, stroke and vasospasm treatment.6–11 We detail our clinical experience since the release of these new guide catheters to exhibit the safety and efficacy of their use in everyday clinical practice.
Methods
Institutional review board approval for this study was obtained from the Medical University of South Carolina. From October 2007 to November 2011, 1188 consecutive patients underwent therapeutic neurointerventional procedures. We excluded any patient where guide catheter support was not critical to the success of the surgery, including external carotid artery embolizations, cervical carotid or extracranial vertebral artery stenting, etc. Patients were also excluded if the images did not adequately define the final location of the guide catheter or the anatomy. We detailed the manufacturer and model of the guide catheters used in the study for intracranial access. We retrospectively reviewed the archived angiographic runs and still images as well as procedure reports.
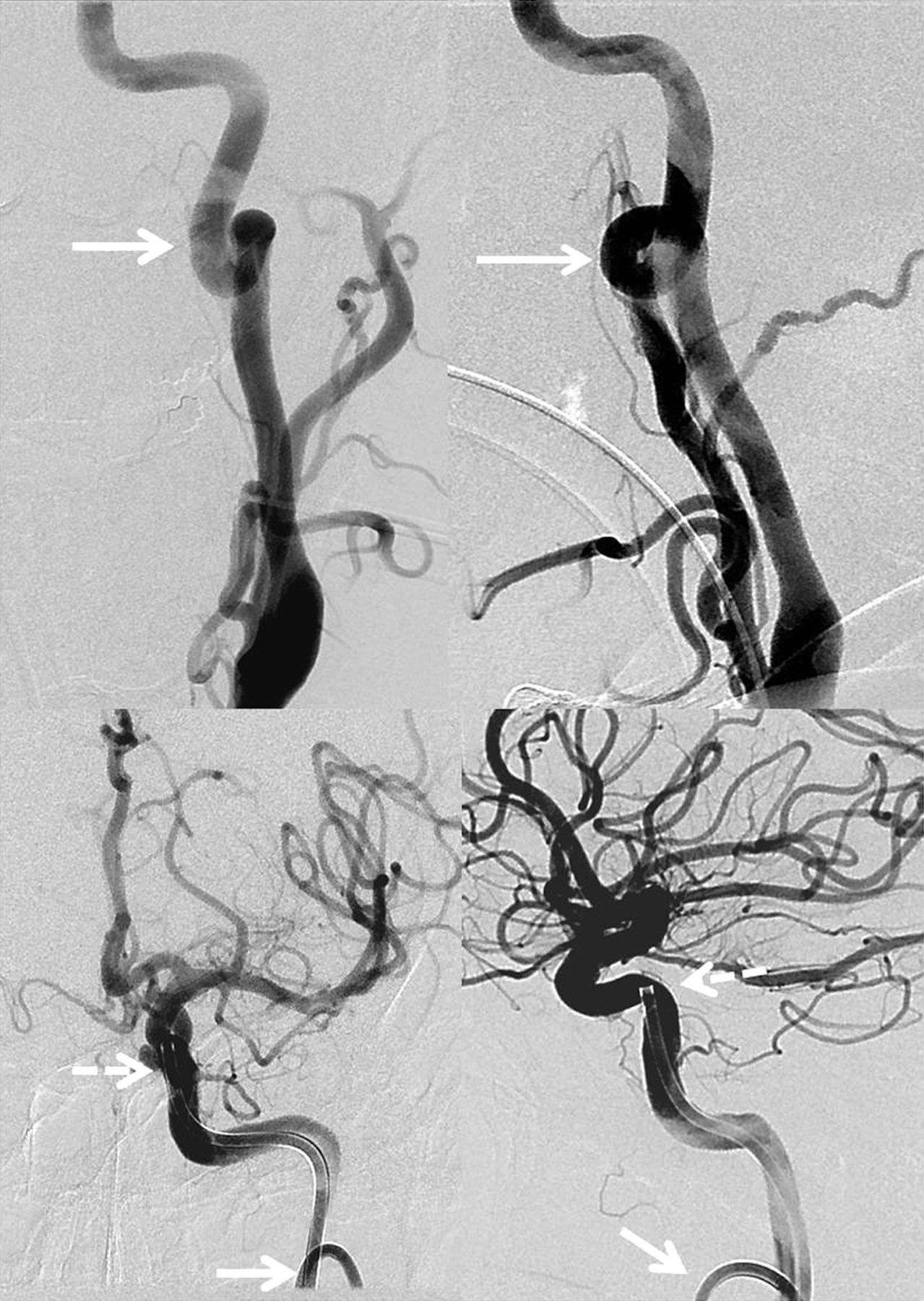
Clinical success was defined by the ability to achieve distal vascular access in the carotid siphon, as denoted by location of the guide catheter tip (figure 1), and practical performance graded by the number of sharp turns the catheter was able to navigate in either the anterior or posterior circulation (figure 2). A 360° loop in the cervical carotid artery was counted as two 90° loops. Gentle 90° curves in the cervical segments were not counted. The posterior circulation intracranial purchase was not separately evaluated or included as a marker for clinical success, as there is significantly more variability in anatomy, and distal vertebral extracranial guide catheter placement (V3 segment) is usually acceptable; these data are captured in the aggregate data regarding numbers of turns negotiated. The final location of the guide catheter tip and any guide catheter related complications were also documented. Complications were considered guide catheter related if they occurred during guide catheter placement or were clearly related to the guide catheter. This was documented on control angiogram after guide catheter placement or at the end of the procedure, such as a dissection or embolism.
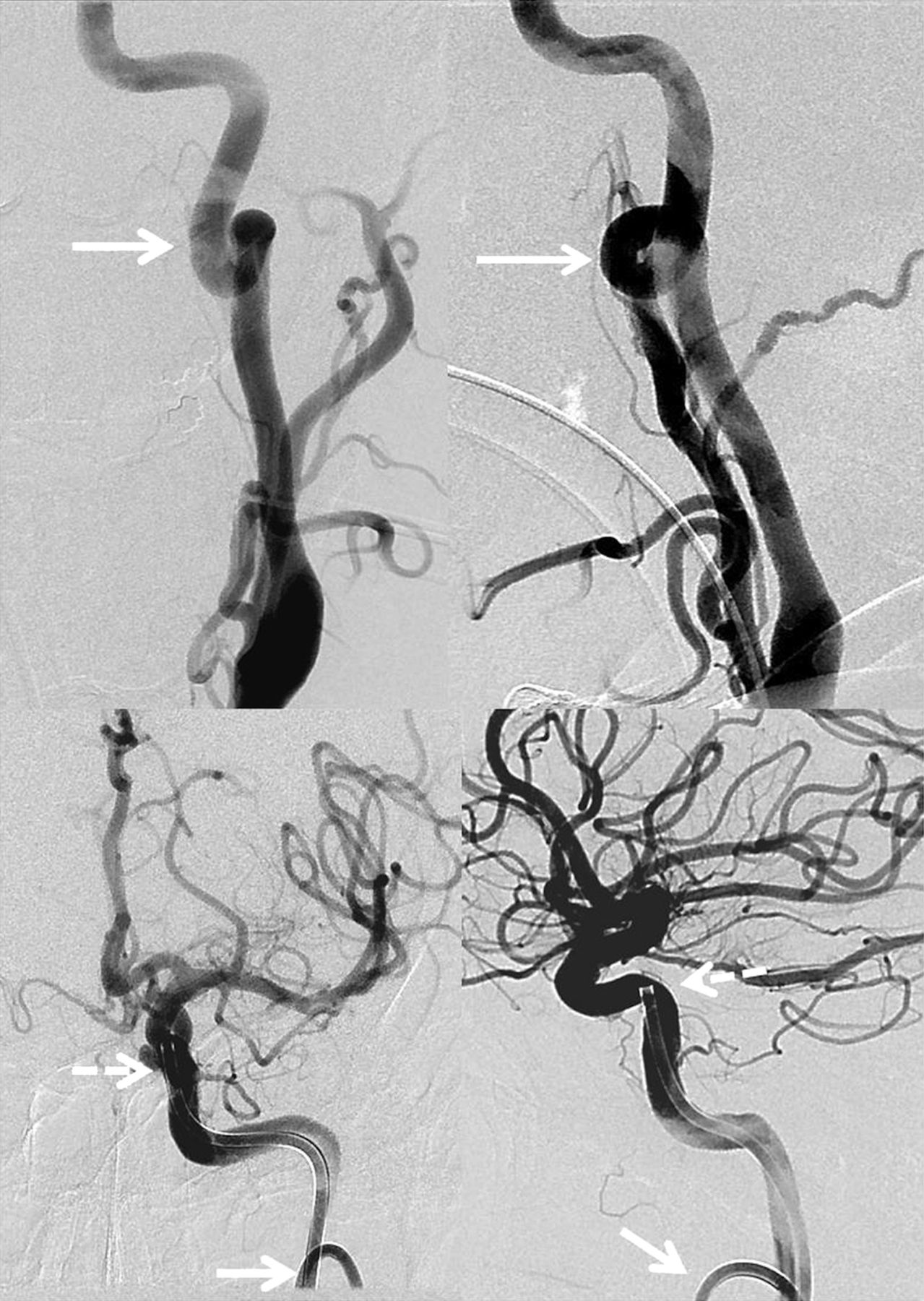
Frontal and lateral angiographic images of the left cervical carotid artery (top row, respectively) and intracranial internal carotid artery (bottom row, respectively) after placement of a 0.070 inch Neuron guide catheter into the vertical petrous segment of the carotid artery. Arrows denote loop in the cervical internal carotid artery which accounts for the two sharp turns the catheter navigated. Broken arrows denote final location of the catheter tip in the vertical petrous internal carotid artery after traversing two additional sharp turns for a total of four sharp turns negotiated.

Frontal and lateral image of the carotid siphon delineating the specified location the authors used in assigning final placement of the guide catheter tip, inferring number of sharp turns navigated assuming no cervical internal carotid artery (ICA) tortuousity. A=distal cervical ICA (0 turns); B=horizontal petrous ICA (one turn); C=vertical petrous ICA (two turns); and D=cavernous carotid artery (three turns).
We segregated the catheters into two technological paradigms. These included the current generation guide catheters (Neuron (Penumbra Inc, Oakland, California, USA) and Chaperone (Microvention-Terumo, Irvine, California, USA)) that represent newer and more flexible design allowing navigation around one or more sharp turns, and conventional guide catheters (Shuttle sheath (Cook, Bloomington, Indiana, USA) and Envoy XB (Codman, Raynham, Massachusetts, USA)) that are very rigid to provide linear support. The current generation guide catheters were further subdivided into two groups based on inner diameter dimensions of either 0.053 inch or 5 French and 0.070 inch or 6 French, based on standard clinical use. To assess performance, the larger 0.070 inch caliber guide catheters were judged to be successful by navigating one or more turns and 0.053 inch and smaller catheters had to navigate two or more turns. Success at navigating into the intracranial anterior circulation was also documented.
Results
A total of 1188 therapeutic neurointerventional procedures were performed over a 4 year period, of which 659 were eligible for this study. Four hundred and fifty-eight cases were excluded due to target lesions in locations other than the intracranial arterial circulation (eg, external carotid artery, venous, spinal, etc), 23 cases were excluded due to inability to assess the anatomy navigated and the remaining cases were excluded as ease of vascular access was deemed as not being critical to the success of the procedure. During this period, 245 cases were performed utilizing the Neuron 0.070 inch, 152 with the 6 F Chaperone, 99 with the 0.053 inch Neuron, 75 with the 6 F Shuttle sheath, 55 with the Envoy XB and 33 with the 5 F Chaperone. The procedures included treatment of 422 aneurysms, 132 acute ischemic strokes, 58 arteriovenous malformations/arteriovenous fistulas, 23 subarachnoid hemorrhage related vasospasms, 17 intracranial stenoses and seven tumors.
When target lesions were in the anterior circulation, the current generation 0.070 inch guide catheters were able to achieve carotid intracranial purchase in 69.5% of cases and navigated at least one sharp turn in 78.6% of cases (tables 1 and 2).
Number of sharp turns navigated
Final guide catheter placement in the anterior circulation
The Neuron 070 catheter achieved intracranial purchase in 165 out of 205 anterior circulation cases (80.5%), including 53 cases in the horizontal petrous segment, 87 cases in the vertical petrous segment and 25 cases in the cavernous segment. The Neuron 0.070 inch was able to navigate at least one sharp turn 88.2% of the time, two sharp turns 64.9% of the time, three sharp turns 23.7% of the time and four or more sharp turns 8.2% of the time. The 6 F Chaperone catheter achieved intracranial purchase in 67 out of 116 cases (57.3%), including 29 cases in the horizontal petrous segment, 29 cases in the vertical petrous segment and nine cases in the cavernous segment. The Chaperone was able to navigate at least one sharp turn 63.2% of the time, two sharp turns 40.8% of the time, three sharp turns 11.8% of the time and at least four sharp turns 0% of the time. Of the 397 cases utilizing 0.070 inch current generation guide catheters, there were four arterial dissections and one thromboembolic event (1.3%) associated with these guide catheters. All guide catheter related complications were successfully managed without permanent morbidity.
The current generation 0.053 inch catheters were able to obtain anterior circulation intracranial purchase in 73.8% of cases and navigate at least two sharp turns in 60.6% of cases (tables 1 and 2). The Neuron 0.053 inch catheter achieved anterior circulation intracranial purchase in 48 of 63 cases (76.2%). This included 15 cases in the horizontal petrous segment, 22 cases in the vertical petrous segment and 11 cases in the cavernous segment. The Neuron was able to navigate at least one sharp turn 83.8% of the time, two sharp turns 67.7% of the time, three sharp turns 43.4% of the time and at least four sharp turns 20.2% of the time. The 5 F Chaperone achieved intracranial purchase in 11 of 17 cases (64.7%). This included three cases in the horizontal petrous segment, four cases in the vertical petrous segment and three cases in the cavernous segment. The Chaperone was able to navigate one sharp turn 54.5% of the time, two sharp turns 39.4% of the time, three sharp turns 21.2% of the time and four sharp turns 0% of the time. There was one carotid–cavernous fistula (CCF) related to these guide catheters (0.8%).
By comparison, the 6 F Envoy XB and 6 F Shuttle Sheath were successful in obtaining intracranial carotid access in four of 116 anterior circulation cases. There were three vessel dissections encountered during the 130 cases (2.3%) with the use of these guide catheters.
Discussion
In this report, we have documented our clinical experience with the current generation guide catheters that allow for distal vascular access, even in the setting of tortuous anatomy. Utilizing current generation 0.070 inch guide catheters, we found that we were able to successfully achieve intracranial carotid purchase in 70% of cases and navigate at least one sharp turn in 79% of cases. When utilizing 0.053 inch guide catheters, intracranial carotid purchase was achieved in 74% of cases and at least two sharp turns were negotiated in 61% of cases. By comparison, intracranial carotid purchase utilizing conventional guide catheters was possible in only 3.4% of cases, and no sharp turns were made in 87.7% of cases (p<0.05). This was achieved while maintaining a similar safety profile with conventional guide catheters of an approximately 1.1% guide catheter related complication rate.
Current generation guide catheters were created to address the deficiency of often insufficient support provided by conventional guide catheters.9 These current generation guide catheters capitalize on the increased support afforded by geometrical anchoring of the catheter around sharp vascular bends. This allows the guide catheters to become softer and more trackable while providing similar support. This then permits improved and deeper distal access, often into the carotid siphon and closer to the target lesion. Access to the carotid siphon allows for improved stability, more predictable microcatheter movement during engagement with the target lesion and better control of device deployment, which likely translates into a safer surgery.9 Previous reports have discussed initial experience, theoretical benefits and potential uses.11 Several reports have detailed small clinical experiences with these current generation guide catheters and reported low complication rates. However, these series mostly reported cases where traditional guide catheters failed and these current generation guide catheters allowed technical procedural success.6–11 The current study is the largest and most comprehensive assessment of current generation guide catheter performance in everyday clinical practice.
We found that the Neuron 0.070 inch was successful in navigating into the intracranial carotid artery 80.5% and traversing at least one sharp turn 88.2% of the time and Chaperone 6 F was successful 57.3% and 62.7% of the time, respectively. These results, however, may underestimate success in current practice, as our philosophy has evolved over the past 3 years from traditional proximal placement to our current practice of more routine distal intracranial placement. There is a clear learning curve involved in appropriately using these catheters as operators learn the mechanics and features unique to each of these different guide catheters. There are several factors that impact the location of final guide catheter tip placement, and choice of placement can vary by operator. Final guide catheter placement into the distal cavernous segment is sometimes the goal, while advancement to the horizontal petrous segment is the goal in others, depending on anatomy of the siphon and location of the target lesion. Administration of intra-arterial verapamil prior to distal selective catheterization may decrease vasospasm related limitations. The use of a shaped diagnostic insert that precedes the guide catheter allows for much improved tracking of the guide catheter around sharp curves.
Understanding the interaction and characteristics of the catheter relative to the diagnostic insert is also important. The 0.070 inch Neuron catheter is relatively supple whereas the insert of the 0.070 inch Neuron is relatively stiff. This combination allows stable selective catheterization of the great vessels off the arch and navigation around the petrous curve at the skull base but is too rigid for further distal use. The Chaperone guide catheter is relatively stiff while the insert is relatively supple. This makes selection of the great vessels off the arch challenging and the use of a long taper Terumo glidewire is recommended. The supple insert, however, allows more distal catheterization, often into the cavernous segment of the internal carotid artery which then supports advancement of the guide catheter. We experienced a cavernous carotid fistula due to 0.038 inch guide wire perforation early in our experience. Paying close attention to wire and catheter movement can remedy this particular complication during initial advancement. Improvements in establishing a balance between the flexibility of the guide catheter and diagnostic insert as well as increased experience with this advance in catheter technology will likely result in significantly increased success rates. We found no significant difference in catheter related complications between the catheter types or the presence of an insert inside the catheter, suggesting that operator preference and understanding of catheter behavior is likely more important than catheter type.
While the distal placement of guide catheters into the intracranial carotid siphon intuitively seems more dangerous, we encountered fewer catheter related adverse events. When intracranial purchase was achieved, we had no intracranial vessel dissections. In addition to the above-mentioned CCF, there was one elective case with a thromboembolic event. By comparison, when only cervical guide catheter access was obtained, there were seven vessel injuries. This is likely related to improved guide catheter stability when the catheter is anchored around the curves of the siphon, which are further reinforced by the bony skull base. In contrast, the cervical vessels often have gentle curves surrounded by pliable soft tissue. The conventional guide catheters are supported by mechanical rigidity designed to resist linear translation. This creates a situation such that when devices are being forcefully advanced the distal guide catheters are supported around multiple bends whereas cervical guide catheters tend to back out. Further, as the force to advance the device is removed, the distal catheter will usually remain stable while the cervical catheters will usually ride back up the carotid. This ‘to and fro’ motion in the cervical carotid artery likely gives rise to the mechanism of the encountered vessel dissections. One other factor may be that eight of the nine cases where complications were encountered were emergency cases treating five acute ischemic strokes and three intracranial aneurysms. This suggests that final location of the guide catheter tip is likely more important than catheter type and guide catheter related complications, while infrequent, are more common in the emergency setting.
The 0.053 inch Neuron guide catheter was successful in intracranial carotid vascular access in 74% of cases and at least two sharp turns were navigated in 68% of cases. We do not use this guide catheter with a diagnostic insert and therefore required an exchange with a diagnostic catheter. The Chaperone 5 F guide catheter has a diagnostic insert that has similar characteristics as its larger 6 F version and was successful in reaching the intracranial carotid artery in 65% of cases and navigating at least two sharp turns in 40% of cases. This allows distal catheterization, often into the cavernous segment of the internal carotid artery which then supports advancement of the guide catheter. There was one guide wire related CCF related to these smaller, more supple guide catheters.
One advantage of using distal guide catheter placement over distal access catheters is avoiding tri-axial systems that are known to create the potential for embolic complications. There is also a likely significant decrease in procedural device cost as the distal access catheter technique relies on tracking over a large microwire or microcatheter or telescoping sequentially smaller distal access catheters to track into the carotid siphon. Although the use of a microwire rather than a 0.038 inch glidewire is likely safer, we experienced only one guidewire related complication early in our experience. The proximity of the guide catheter tip placement to the target lesion is likely not significantly different between the two techniques.
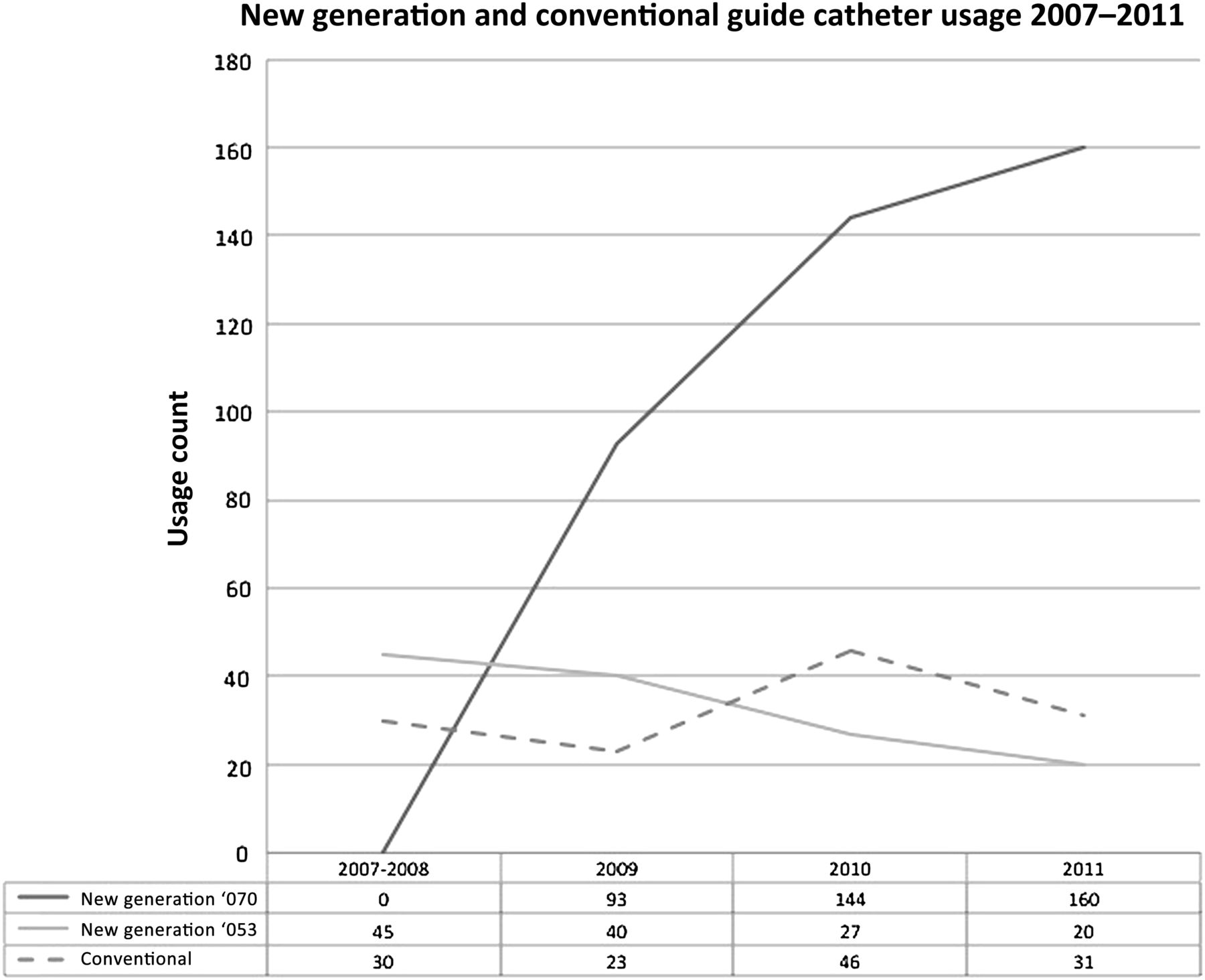
A limitation of this paper is the retrospective design. The inclusion of our experience with these devices since their commercial release likely affects the success rates and the complication rates due to evolution of operator experience and familiarity. Improvements to the catheter design during this period could also influence individual catheter success rates. One measure of clinical success was achievement of intracranial carotid purchase while not including posterior circulation. This metric was chosen due to the relative anatomical uniformity of the carotid siphon relative to the vertebral arteries and the safety of navigating the extradural carotid siphon. Direct comparison of current clinical guide catheter performance to conventional guide catheters is likely not possible but this does highlight the differences in philosophy of use, as depicted in figure 3. While it is often challenging to understand philosophical influences on decisions, figure 3 highlights the robust growth of this type of guide catheter usage as the case volume increased. It is likely that use of current generation guide catheters allows faster and safer procedures although measuring this in an accurate manner is not possible retrospectively. Finally, a major limitation of this study is that this type of review does not allow for a systematic review of the methodology.
{kind=link}
{kind=link}
{kind=link}
Guide catheter usage over time. Usage was also influenced by growth in procedure volume as the practice started in October 2007.
These data represent our clinical experience using current generation guide catheters as firstline access devices. While there are some limitations, these data should establish parameters for operators utilizing these guide catheters in everyday practice.
Conclusion
Current generation guide catheters allow distal access through tortuous pathways with a high rate of success and a low rate of complications. When intracranial location of the guide catheter can be obtained, this was associated with fewer complications.
Footnotes
-
Competing interests None.
-
Ethics approval Institutional review board approval for this study was obtained from the Medical University of South Carolina.
-
Provenance and peer review Not commissioned; externally peer reviewed.