Article Text

Abstract
Background and purpose Diffusion weighted imaging (DWI) may be used to evaluate post-coiling ischemia. Heparinization protocols for cerebral aneurysm coiling procedures differ among operators and centers, with little literature surrounding its effect on DWI lesions. The goal of this study was to determine which factors, including heparinization protocols, may affect DWI lesion load post-coiling.
Materials and methods A review of 135 coiling procedures over 5 years at our centre was performed. Procedural data including length of procedure, number of coils used, stent or balloon assistance and operators were collected. Procedures were either assigned as using a bolus dose (>2000 U at any one time) or small aliquots of heparin (≤2000 U). Postprocedure DWI was reviewed and lesions were classified as small (< 5mm), medium (5–10 mm) or large (>10 mm). The cases were then classified into group 1 (≤5 small lesions) or group 2 (>5 small lesions or ≥1 medium or large lesion). Multivariate regression of the procedural variables for the two groups was calculated. A p value of <0.05 was considered significant.
Results There were 78 procedures in group 1 and 57 procedures in group 2. Patients who received small aliquots (n=37) versus boluses of heparin (n=98) intraprocedurally had significantly greater frequency and size of DWI lesions (p=0.03). None of the other procedural variables was found to impact on lesion load.
Conclusions More substantial DWI lesions were associated with small aliquots of heparin dosage compared with bolus doses. Heparin boluses should be preferentially administered during aneurysm coiling.
Statistics from Altmetric.com
Introduction
The advent of the Guglielmi detachable coils (Boston Scientific Neurovascular, Natick, Massachusetts, USA) in the 1990s has allowed cerebral aneurysms to be treated by endovascular coiling with favorable short term outcomes.1 Over the past 20 years, the advantages of endovascular procedures over surgery as treatment for aneurysms have been reported for ruptured aneurysms.2 ,3 While these studies demonstrate that endovascular coiling fare more favorably in terms of postprocedure morbidity and mortality over surgical clipping,4 aneurysm recurrence from neck remnants, recanalization, vasospasm, incomplete obliteration and bleeding remain major concerns in endovascular coiling. Even more common is the risk of thromboembolism which can be due to either thrombus formation within the parent artery, microembolization of an atherosclerotic plaque or embolization from a partially thrombosed aneurysm itself.5–7
In our center, imaging follow-up with contrast enhanced MRI is performed after every coiling procedure prior to patient discharge to provide a baseline evaluation of aneurysm obliteration after the intervention. A diffusion weighted sequence is part of our routine imaging following aneurysm coiling and is better at detecting ischemic lesions compared with CT.8 While these lesions are usually clinically silent, they may cause symptoms depending on the eloquence of brain involved.
Patient, anatomical and procedural factors which may be associated with the risk of postprocedure ischemic lesions include morphology, size, anatomical location of the aneurysm, rupture status, as well as patient age, comorbidities and concurrent treatments. Factors which can impact on the number of diffusion weighted lesions post-coiling include: (i) length of the procedure; (ii) number of assistive devices used to perform coiling, such as a balloon or stent; and (iii) heparinization routines.9–12 There is little literature assessing the relationship between heparinization and diffusion weighted imaging (DWI) lesions post-coiling. In our center, a baseline contrast enhanced MR angiography study with DWI is performed prior to the patient being discharged. These studies are interpreted by one of two neurointerventionists. We had noticed a variable degree of DWI lesions on the immediate post-coiling MRI. Many of the MRIs demonstrated no or minimal DWI lesions, while some patients had more DWI lesions. These lesions seemingly appeared unrelated to the length of the procedure or technical difficulty. This raised the question if there were other factors that could explain the variability in DWI lesions.
Heparin boluses ranging from 2500 to 7500 U have routinely been used in neuroangiography.13 In our own experience, neurointerventionists from different training backgrounds have variable heparin regimens. Some operators have preferred using small aliquots while others prefer bolus heparin doses. However, no study has yet statistically compared the effect of using bolus doses versus aliquots of heparin on frequency of DWI lesions.
The main goal of this study was to determine which procedural variables were associated with a greater number of diffusion weighted lesions post-endovascular coiling of aneurysms.
Materials and methods
Selection of patient population
A retrospective review of all aneurysms coiled between March 2006 and June 2010 at our institution was performed, with the approval of our institutional ethics board. This consisted of 277 coiling procedures of which 113 were excluded due to absent postprocedure MR image, MR images obtained more than 10 days after surgery or insufficient documentation of the periprocedural heparinization protocol, leaving 135 procedures in 126 patients. We started using contrast enhanced magnetic resonance angiography (CEMRA) in the latter half of 2006, however, introduction of this new technique was initially slow.14 At first, a DWI image was not included as part of the routine post-coiling protocol. It then later became part of the routine post-coiling protocol in 2007. Routine CEMRA including DWI at our institution fully replaced catheter angiography by March 2007.
Patient records were reviewed and the following baseline characteristics were recorded for each patient: age, sex, aneurysm size, neck to dome ratio and presentation of the aneurysm (ruptured or unruptured). We only routinely administer antiplatelet agents for aneurysm coiling in stent assisted cases. Therefore, the use of antiplatelet medication was not recorded in our study.
Aneurysm embolization procedure
Coiling procedures were performed through the transfemoral route under general anesthesia. Neurological status could therefore not be assessed during the procedure. All flushed saline and contrast medium were heparinized (1000 U/100 ml) and the guiding catheter and microcatheter were both placed with a continuous heparinized saline drip. Balloon assisted techniques were performed in more challenging cases, including wider neck aneurysms. All treated aneurysms were evaluated angiographically by the interventional team after embolization and the results were classified into complete occlusion (no filling of aneurysm rests without sac or neck remnant) or incomplete occlusion (small neck remnant or partial occlusion) according to the Raymond and Roy scale.15 ,16 Procedural variables such as length of procedure, number of coils used, balloon or stent assistance, and identity of the operator were collected.
Heparinization
Heparin was administered during the procedure in conjunction with activated clotting time (ACT) readings, whenever ACT was inferior to the targeted value of 250 s. The heparinization pattern (dosage and frequency) for each procedure was noted. The heparin protocols tended to be quite varied depending on the operator. Some patients were given multiple 1000 unit aliquots, others were given 2000 units initially (quite a frequent occurrence) while others were given a bolus of 100 IU/kg after placement of the first coil. For the purposes of the study, a bolus dose of heparin was a priori defined as >2000 U heparin given at any one time during the procedure, not necessarily as the first heparin administration. The procedures were then assigned as having received either a bolus dose of heparin or aliquots of heparin (≤2000 U at any one time). For example, a patient who received 1000 U of heparin after sheath placement, followed by a bolus of 6000 U after placement of the first coil, was placed in the ‘bolus’ group. In contrast, a patient who received 2000 U of heparin after groin sheath placement and subsequently 1000 U of intermittent heparin was placed in the ‘aliquot’ group.
ACT readings were measured using a kaolin based system (Medtronic ACT-II; Medtronics Inc, Minneapolis, Minnesota, USA) and were monitored throughout the embolization procedure. The time to achieve ACT was only reliably recorded in 88 procedures and therefore was not used as a perioperative variable in this study.
Characterization of postprocedural thromboembolic events with DWI
All patients treated for aneurysms underwent MR imaging within 10 days of treatment for a baseline comparison, as per the institutional protocol. Imaging was performed with 1.5 T and 3 T systems (Magnetom Vision; Siemens, Erlangen, Germany) using a multisection, single shot, spin echo, echo planer imaging sequence. Diffusion gradients were applied in each of the x, y and z directions with three b values (0, 500 and 1000 s/mm2). Imaging parameters included a TE of 94 ms, field of view of 23 cm, matrix of 128 and section thickness of 5.5 mm for the 1.5 T system and a TE of 83 ms, field of view of 23 cm, matrix of 128 and section thickness of 3 mm for the 3 T system. Conventional spin echo imaging also was performed at each examination under T1 and T2 weighted conditions and with a fluid attenuated inversion recovery sequence.
Postprocedure MRIs were reviewed by one investigator (MJLF) for evidence of acute ischemia, which were seen as new areas of restricted diffusion on DWI. We included punctate hyperintense lesions on the DWI image which did not have correspondingly low ADC values as true restricted diffusion lesions. If abnormalities were noted, their number and size were recorded and the lesions were then prospectively classified as small (<5 mm) (as illustrated in figure 1), medium (5–10 mm) or large (>10 mm) as a variation of the scheme used by Rordorf et al 11 and Soeda et al. 12 ,17

Diffusion weighted imaging of a 54-year-old woman initially presenting with an asymptomatic intrasellar paraophthalmic artery aneurysm. Imaging done 24 h after aneurysm coiling shows >5 small punctate lesions. Each arrow represents a single DWI lesion.
Statistical analysis
Our experience with post-coiling CEMRA DWI has been that the majority of cases have either no or a few (<5) small DWI lesions and represent minimal DWI lesion load. Patients with more than five DWI lesions or with medium to large lesions were then grouped together to represent more significant DWI ischemic loads. This resulted in two groups: group 1—cases with minor or no ischemic lesions postprocedure; and group 2—cases with more than five small lesions or at least one medium or large lesion on DWI. We then performed a univariate analysis to determine which variables were associated with minor/no versus more significant lesion loads. Variables that were significant with p<0.25 in univariate linear regression were analyzed using a multivariate logistic regression model to determine the variables which were significantly associated with DWI lesions. For each comparison, ORs with p values were computed. A p value of <0.05 was considered significant.
SPSS software package (V.18.0 for Mac, SPSS Inc) was used for the statistical analysis.
Results
A total of 135 coiling procedures were analyzed in 126 patients. There were 97 female patients and 29 male patients. Six women and three men had two separate aneurysm coiling procedures. The mean age of the patients was 55.1 years (range 28–91). Sixty-four aneurysms were ruptured while 71 were unruptured. There were 53 small, 64 medium and 18 large aneurysms. The mean neck:dome ratio for all aneurysms coiled was 0.57 (SD 0.27). Thirteen cases were stent assisted cases and there were 51 balloon assisted cases (table 1).
Baseline characteristics and procedural variables according to the dichotomous variables of none/<5 small (group 1) versus >5/medium or large diffusion weighted imaging lesions (group 2)
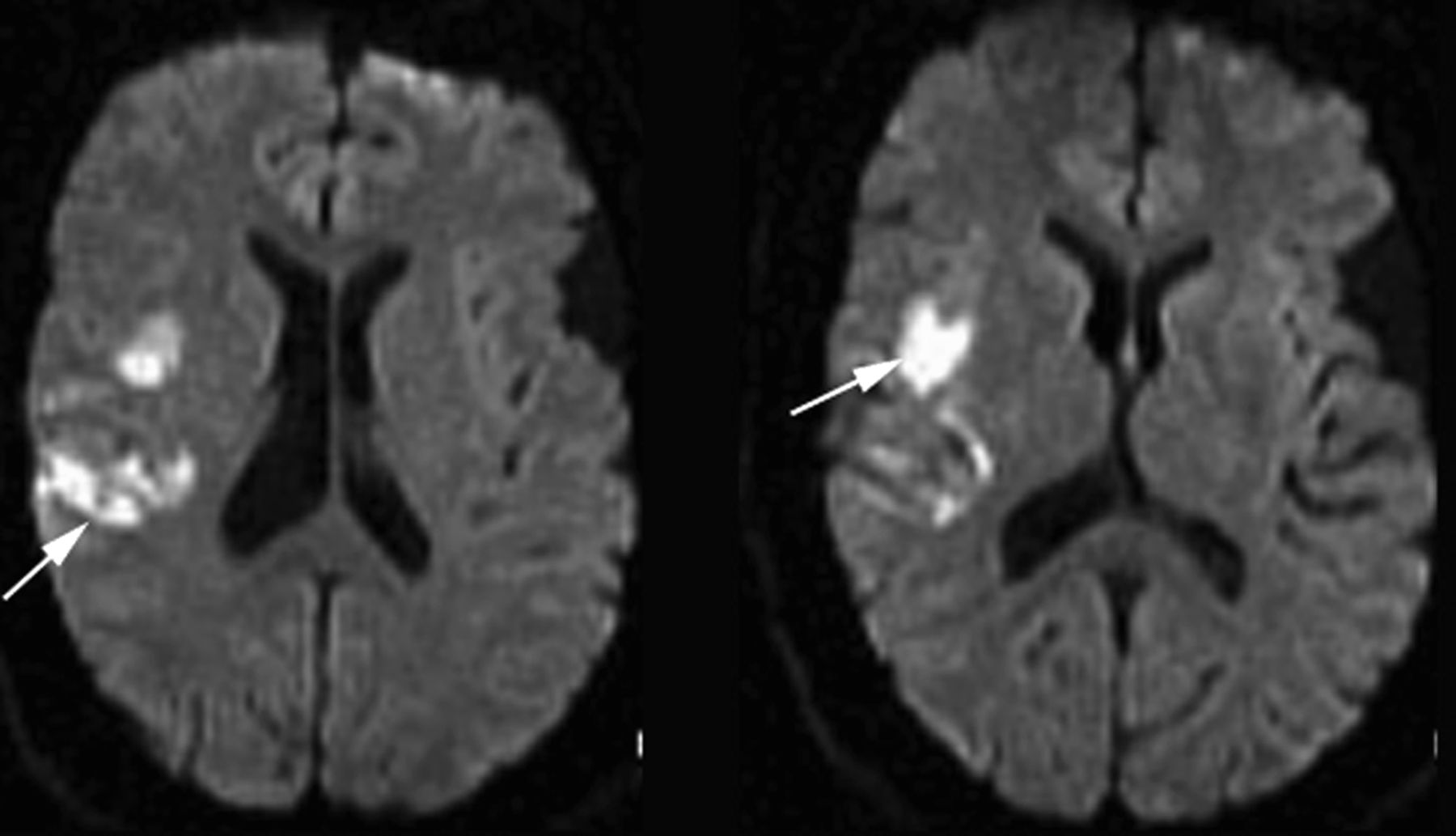
In the analysis comparing the variables associated with minor/no versus more DWI lesions load, there were 78 procedures in group 1 (cases with <5 small acute infarcts or no infarct on DWI) and 57 procedures in group 2 (procedures with >5 small lesions or at least one medium or large lesion on DWI. An example of a case in which a large lesion is showed in figure 2). The total number of cases with ischemic lesions was 96 (71% of total cases) but 59 (44%) had 0–2 small lesions.
{kind=link}
{kind=link}
Diffusion weighted imaging of a 48-year-old man, initially presenting with a ruptured internal carotid aneurysm, shows a large infarct in the right parietal lobe 72 h post-coiling.
A univariate logistic regression analysis was performed with the dichotomous dependent variable being cases with <5 small acute infarcts or no infarct on DWI compared with >5 small lesions or at least one medium or large lesion on DWI. In the univariate analysis, heparin bolus was associated with less DWI load (group 1) (table 1). All variables with p values <0.25 were considered covariates in the final multivariate analysis (table 2). The association between heparin bolus and fewer DWI ischemic lesions continued to be significant (OR=0.44, 95% CI 0.2 to 0.97, p=0.04).
Multivariate logistic regression model for outcome groups
A subanalysis of rupture status in relation to outcome, as measured by DWI versus no DWI lesion and group 1 versus group 2, was also performed. There was no significant difference demonstrated in either outcome measure when rupture status was the independent variable (table 3).
Subanalysis with rupture status (ruptured vs unruptured) as an independent variable
Discussion
Animal studies have shown that DWI can reveal an ischemic zone within 5 min18 to 1–3 h after onset of symptoms.19 ,20 In humans, DWI abnormalities are seen as early as 2–6 h after the onset of symptoms.21 ,22 Diffusion weighted MRI performed soon after endovascular coiling allows visualization of acute ischemic lesions that develop periprocedurally.
Previous studies have commented on a higher number of ischemic lesions detected on DWI than initially predicted, with a frequency ranging from 10% to 71% of cases, as illustrated in table 4. We found evidence of DWI lesions in 96 of the 135 cases (71%) with most cases (44%) having 0–2 small lesions, representing a minimal ischemic lesion load.
Published studies on frequency of diffusion weighted imaging lesions post-coiling of cerebral aneurysms
Procedural determinants of ischemic lesions
Our results indicate that neither the length of the embolization procedure nor the number of coils utilized were associated with an increased risk of ischemic lesions. These findings are consistent with the observations of Grunwald et al who did not find any association between these two variables and frequency of ischemic lesions.9 In addition, another study noted that the number of coils did not increase the risk of thromboembolic complications, as measured by DWI.11
Use of balloon assisted techniques was not significantly associated with a higher frequency of DWI lesions. Balloon assisted techniques have been associated with an increase in frequency of ischemic lesions10 ,12 and with no additional risk compared with conventional embolization techniques.25 ,26 Other studies described the complications and safety issues relating to balloon assisted techniques but did not use DWI imaging to view postprocedural lesions.26 Additional studies using DWI and limiting potential confounding variables are required to determine whether balloons pose an additional risk for thromboembolic events.
Four different experienced staff interventional neuroradiologists were the primary operators in the cases reviewed. Due to their different training backgrounds and number of years practicing at the institution, it was possible that their respective strategies for treatment, endovascular technique and choice of instrumentation could affect the outcome of the procedures. However, the occurrence of ischemic lesions was not found to differ significantly among them in this study.
Heparinization in endovascular coiling procedures
Heparin bolus doses of 2500–7500 U have routinely been used in neuroangiography.13 There are few data on heparinization protocols in aneurysm coiling. In our own center, with neurointerventionists having been trained at different centers, there was heterogeneity in the heparinization protocols; some preferred boluses of heparin while some operators preferred aliquots. One of the motivating reasons for undertaking this study was to determine if there was any difference in DWI lesions load in patients receiving the different heparin protocols.
We found that administration of small aliquots of heparin (<2000 U) was significantly associated with a higher risk of ischemic events compared with administration of a bolus dose of heparin (>2000 U) (OR=0.41, p =0.04). This was the case regardless of the total dose of heparin administered and whether the target ACT was achieved. Higher doses of heparin increase the half-life of the drug significantly compared with smaller doses. Clearance of heparin occurs through a combination of a rapid saturable mechanism which is mostly due to endothelial cell receptor binding and much slower first order mechanisms which is renal.27 As described in the American Heart Association's guide to anticoagulant therapy, the apparent biological half-life of heparin increases from 30 min after an intravenous bolus of 25 U/kg (1750 U for the average 70 kg man) to 60 min with an intravenous bolus of 100 U/kg (7000 U for the average 70 kg man).28 The World Federation of Interventional and Therapeutic Neuroradiology has issued recommendations for heparin boluses of 5000 U for aneurysm coiling with subsequent aliquots of 1000 U. Our findings support the routine use of heparin boluses over small aliquots in aneurysm coiling.
Previous research on complications post-coiling has separated ruptured from unruptured aneurysms when studying the effects of procedural variables.2 ,10 ,29 In our case, it was felt that the protocol for coiling at our institution was similar for both groups, including target ACT and heparinization protocol. There was no significant difference in the presence of fewer versus more significant DWI lesion loads for either the ruptured or unruptured aneurysm groups.
Other alternatives to standard heparinization protocols include continuous intravenous heparin. A recent study described low occurrence of microembolic signals (MESs) on transcranial Doppler sonography with the use of a continuous heparin drip following coiling.30 While the vast majority of patients in this study received a continuous heparin drip during the first MES scan (96.7%), the incidence of MESs observed was in this group was lower than in the cases where heparin was not continued (3.4 vs 18.8 MESs/h).
Limitations
One of the major limitations was that this was a retrospective analysis. Ideally, a randomized controlled study would be needed to adequately measure the effect of bolus versus aliquots of heparin on ischemic load. A significant number of patients were not included in the study time period. We wanted to capture as many patients as possible who had post-coiling DWI studies, which is why this study time period was chosen. However, we acknowledge that because of the gradual introduction of CEMRA to replace catheter angiography in our institution, this led to exclusion of a proportion of cases during the study period. We chose DWI as a surrogate for ischemia rather than clinical outcome. DWI lesion load has been used as a surrogate measure of outcome in some recent clinical trials (Evaluating Neuroprotection in Aneurysm Coiling Therapy, ClinicalTrials.gov identifier: NCT00728182). Ideally, detailed neuropsychological testing would have to have been performed but this was beyond the scope of our study. We did not attempt to relate the location of the DWI lesions to the parent artery of the coiled aneurysms. Therefore, it is not possible to determine if lesions resulted from the coiling or as a complication of diagnostic angiography. However, as all patients underwent the same process of diagnostic imaging preprocedure (diagnostic CT angiography followed by coiling procedure) and operators were consistent with their own heparinization protocol for angiography, we did not feel this was a significant issue. Only cases in which DWI was obtained less than 10 days post-coiling were reviewed and we did not perform a subanalysis based on the amount of time post-coiling at which DWI was performed. We did not account for peri- or postprocedural antiplatelet regimens or the use of other anticoagulants which could play a role in ischemic load post-coiling.
Conclusion
Our study indicates that ischemic lesions seen on DWI post-coiling are a frequent occurrence. More substantial lesions were associated with aliquots of heparin compared with bolus doses. In the future, preferential loading with bolus heparin doses above 2000 U when coiling cerebral aneurysms may help reduce DWI lesions post-coiling.
References
Footnotes
-
Competing interests None.
-
Ethics approval Ethics approval was provided by the Ottawa Hospital Research Ethics Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Unpublished data from the study are only available to the authors of the paper.