Article Text

Abstract
Introduction A number of recent trials evaluating intra-arterial therapies for acute ischemic stroke have been completed. We present a review of prospective acute ischemic stroke trials reported in a peer-reviewed forum during the last 20 years to provide insight into the general direction of this rapidly evolving field.
Methods Prospective trials evaluating acute stroke intra-arterial therapies since 1999 were included, with the National Institute of Neurological Disorders and Stroke rtPA trial published in 1995 as a baseline comparator. Patient presenting factors and outcome data were analyzed based on year of publication and best-fit lines and linear regression analyses were generated.
Results Thirteen prospective trials were included. Regression analyses demonstrated no appreciable change in the median NIH Stroke Scale score of subjects at the time of enrollment since 1995 (p=0.44) and no appreciable improvements in good outcome based on a modified Rankin score of 0–2 at 90 days (p=0.66) or mortality at 90 days (p=0.55). A significant increase in time from onset of symptoms to treatment among enrolled patients was noted from 1995 to 2012 (p=0.03). In addition, a significant improvement in recanalization/reperfusion was noted over the last two decades (p=0.02).
Conclusions This review of prospective acute ischemic stroke trials since 1999 indicates a substantial improvement in revascularization in the setting of a significant increase in time to therapy onset, but no appreciable change in good functional outcome.
- Intervention
- Stroke
- Thrombectomy
- Thrombolysis
Statistics from Altmetric.com
Introduction
The treatment of acute ischemic stroke has evolved over the last two decades in concert with improvements in imaging techniques, preventive therapies and intravascular treatments. However, stroke remains the fourth leading cause of death in the USA (Centers for Disease Control, unpublished data, 2012) and, unfortunately, acute stroke intervention remains significantly underutilized.1 The modern treatment paradigm for acute ischemic stroke originates from several large randomized trials evaluating intravenous tissue plasminogen activator (tPA) on stroke outcome measures in the 1990s.2 ,3 While other treatment modalities have been evaluated in rigorous prospective studies since that time, intravenous tPA remains the only Food and Drug Administration (FDA)-approved therapy for acute ischemic stroke with class 1 evidence supporting its use.
In May 2012 the Interventional Management of Stroke (IMS) III trial,4 one of five worldwide randomized trials comparing intra-arterial plus intravenous therapies versus intravenous tPA alone, halted enrollment due to futility. There are four randomized trials evaluating combined intravenous/intra-arterial stroke intervention still underway across the world, including the THERAPY trial in the USA and three European trials (PISTE, MR CLEAN and THRACE), but these results will not be known for several years. The absence of benefit of intra-arterial intervention over intravenous rtPA seen in the IMS III trial is particularly disappointing to the stroke community, especially given recent improvements in imaging, thrombectomy devices and, presumably, outcomes after stroke treatment with cutting edge intra-arterial therapies. We present a review of prospective acute ischemic stroke trials performed during the last 20 years and reported in a peer-reviewed forum (publication or formal presentation at national meeting with peer review screening) to provide insight into the general direction of this rapidly evolving field. This analysis is intended to serve as a review of general trends in commonly reported stroke outcome measures over the last two decades and is not intended to represent a rigorous comparison of different trials to generate robust observations regarding treatment and outcome.
Methods
Prospective trials evaluating acute stroke intra-arterial therapies since 1999 were included, with the National Institute of Neurological Disorders and Stroke (NINDS) rtPA trial2 used as a baseline comparator. Median National Institute of Health Stroke Scale (NIHSS) at time of presentation was recorded for each trial. If a median NIHSS was not reported, mean NIHSS was used as a surrogate. Time to treatment was defined as the time from the onset of stroke symptoms until the administration of intravenous tPA for the NINDS trial and until time of groin puncture for all other trials. Outcome data, including revascularization status at the end of the procedure, modified Rankin score (mRS) at 90 days, mortality at 90 days and incidence of symptomatic and total hemorrhagic complications were evaluated. Good outcome was defined as a mRS of 0–2 at 90 days. Revascularization is reported based upon the Thrombolysis in Cerebral Ischemia (TICI) reperfusion scale; if TICI is not reported, Thrombolysis in Myocardial Ischemia (TIMI) is used as a surrogate.5 Core laboratory adjudication was used in eight of the 13 trials. The rate of intracranial hemorrhage (ICH) and symptomatic ICH were recorded as defined and reported by each individual study. The SARIS trial reported its short-term6 and mid-term7 results in different publications 2 years apart; for analysis purposes, the SARIS results are presented as a single trial completed in 2011. The START8 and TREVO9 trials have yet to be published at the time of writing, but peer-reviewed preliminary results have been presented at national stroke meetings.
Best-fit lines and linear regression analyses were performed using SPSS statistical software. Furthermore, studies were divided into three temporal strata (NINDS, 1999–2008 and 2009–2012) for analysis of presentation and outcome data by ANOVA.
Results
Thirteen prospective trials from 1995 to 2012, including 11 published studies6–7 10–18 and two recent unpublished prospective studies presented at national stroke conferences, were included. Table 1 shows enrollment criteria, treatment arms, median NIHSS and mean time from onset of symptoms to treatment. Outcome data are reported in table 2. Figures 1⇓⇓⇓⇓⇓⇓⇓⇓–10 depict the change in patient presenting factors and outcomes over the last two decades with their associated best-fit lines and p values, as well as these same variables in bar graph format, based upon temporal strata, with 95% confidence interval error bars and ANOVA p value results.
Prospective stroke trials and their criteria for enrollment and patient characteristics
Outcome data from the prospective stroke trials
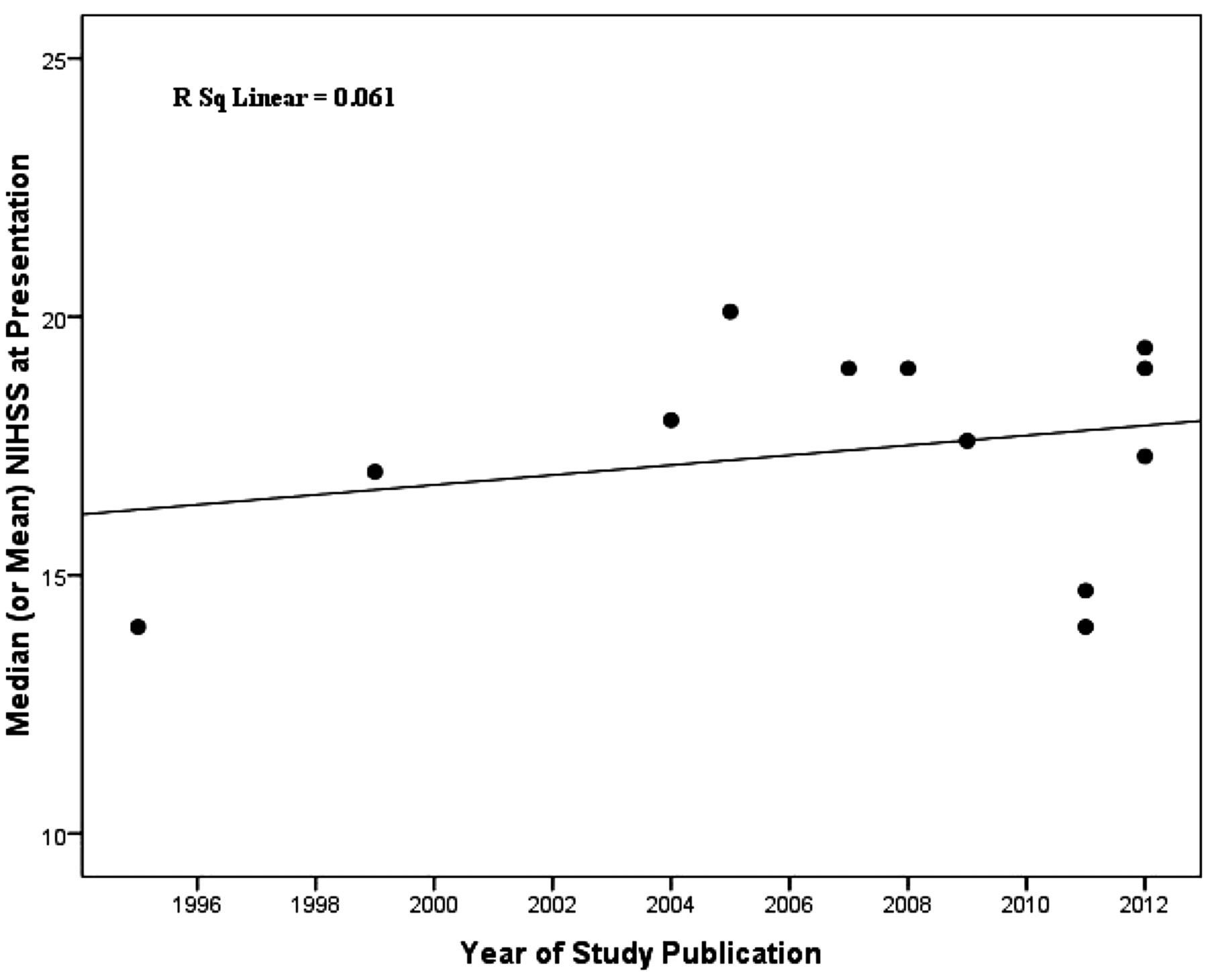
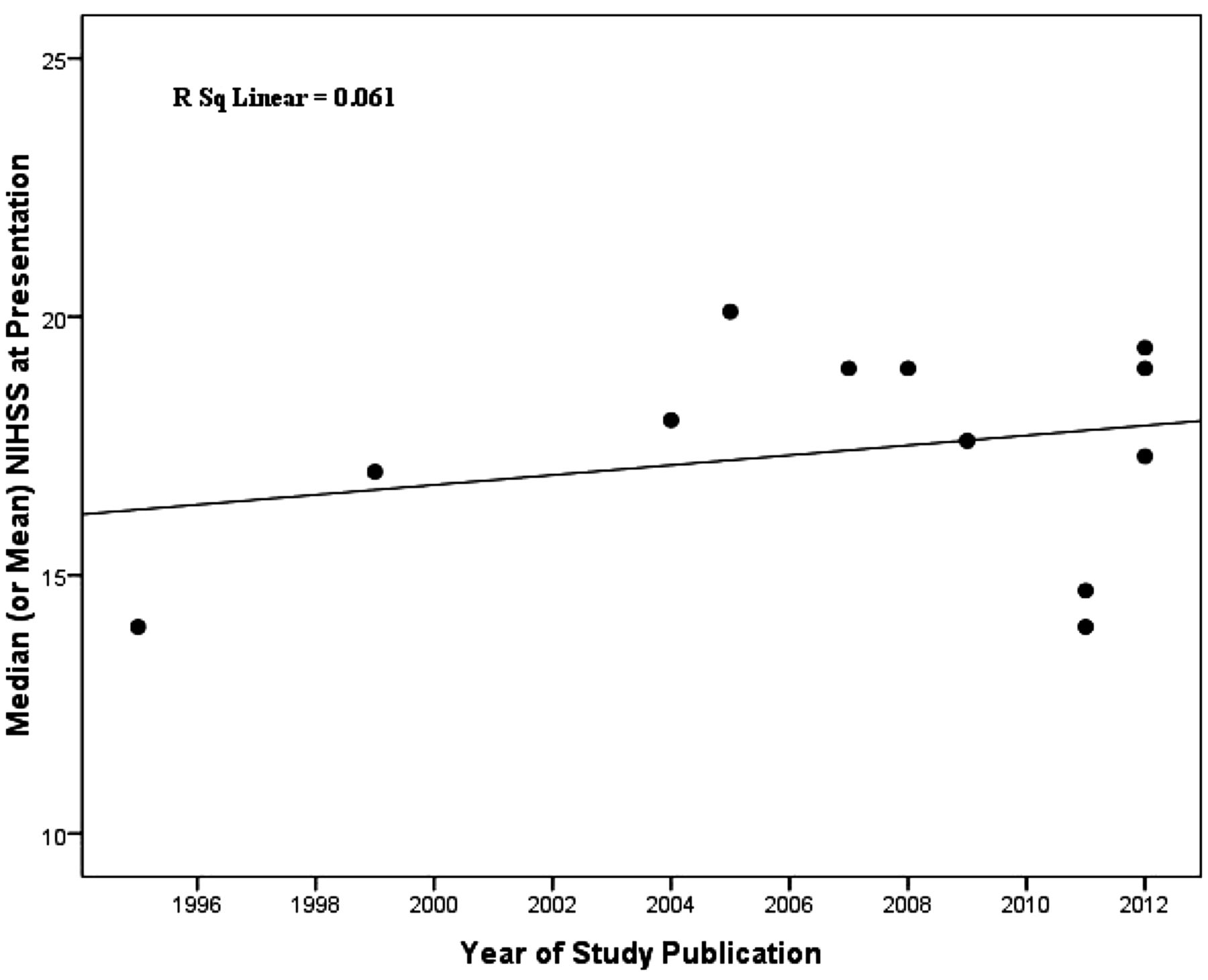
Scatterplot and best-fit line demonstrating no appreciable change in the mean or median NIH Stroke Scale (NIHSS) of subjects at time of enrollment since 1995 (p=0.44).

Bar graph demonstrating a lower median NIH Stroke Scale (NIHSS) of subjects at time of enrollment in the NINDS trial than more recent studies, but no change from 1999–2008 to 2009–2012 (p=0.17).
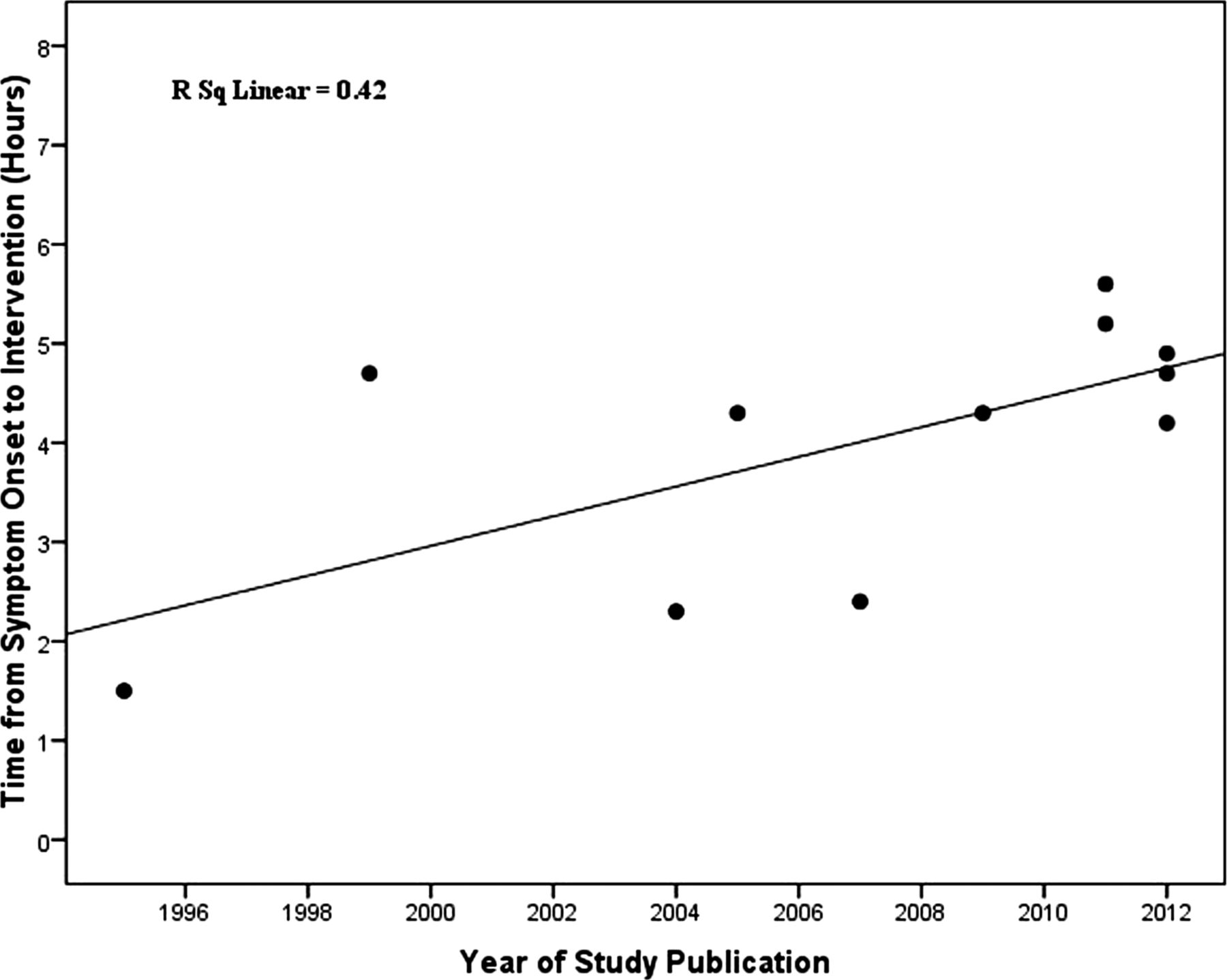
Scatterplot and best-fit line demonstrating an increase in time from onset of symptoms to treatment among enrolled patients. The slope of the line is statistically different from zero (p=0.03).

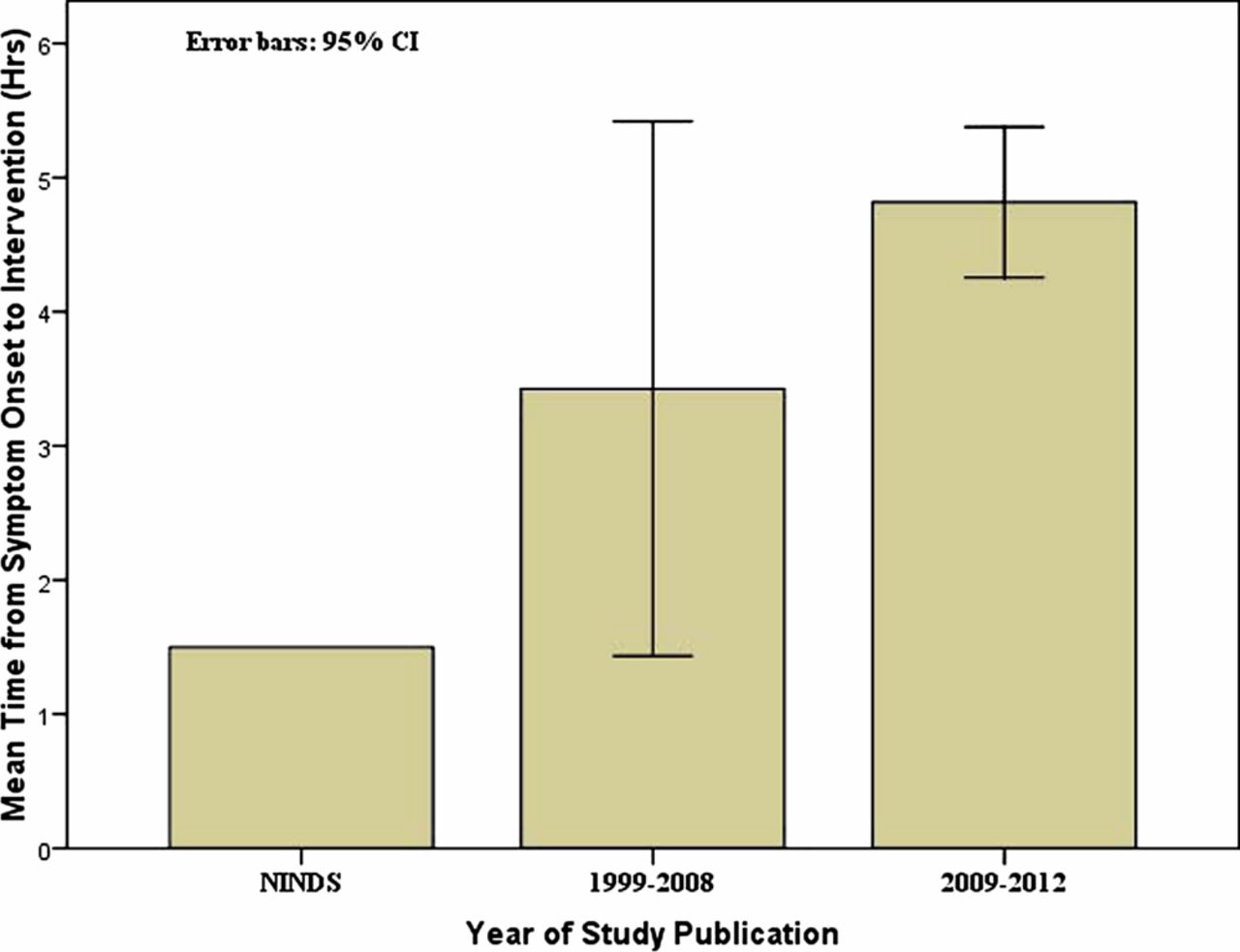
Bar graph demonstrating an increase in mean time from onset of symptoms to treatment among enrolled patients over the last two decades (p=0.01).

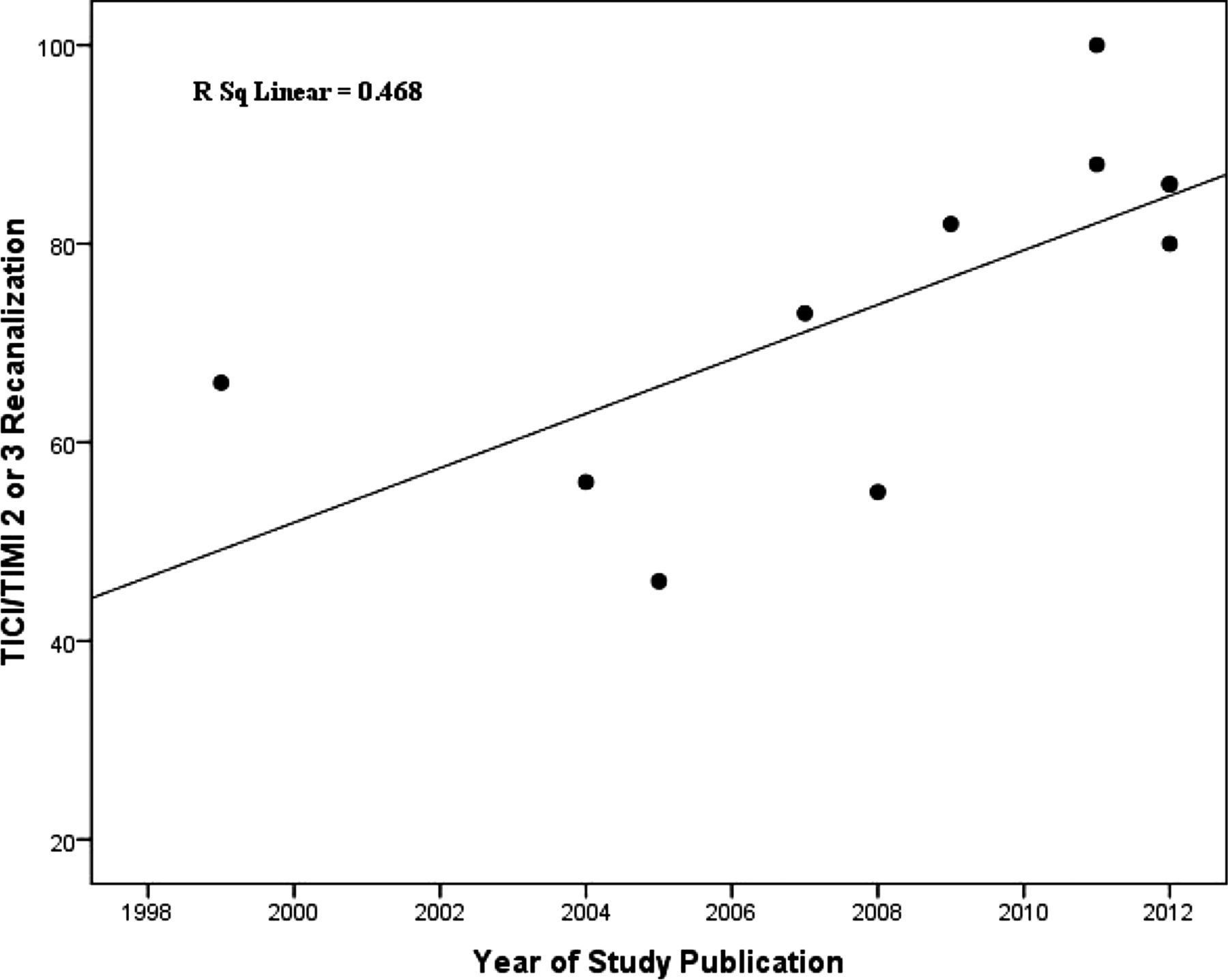
Scatterplot and best-fit line depicting improvement in recanalization/reperfusion over the last two decades. The line slope is significantly different from zero (p=0.02). TICI, Thrombolysis in Cerebral Ischemia; TIMI, Thrombolysis in Myocardial Ischemia.
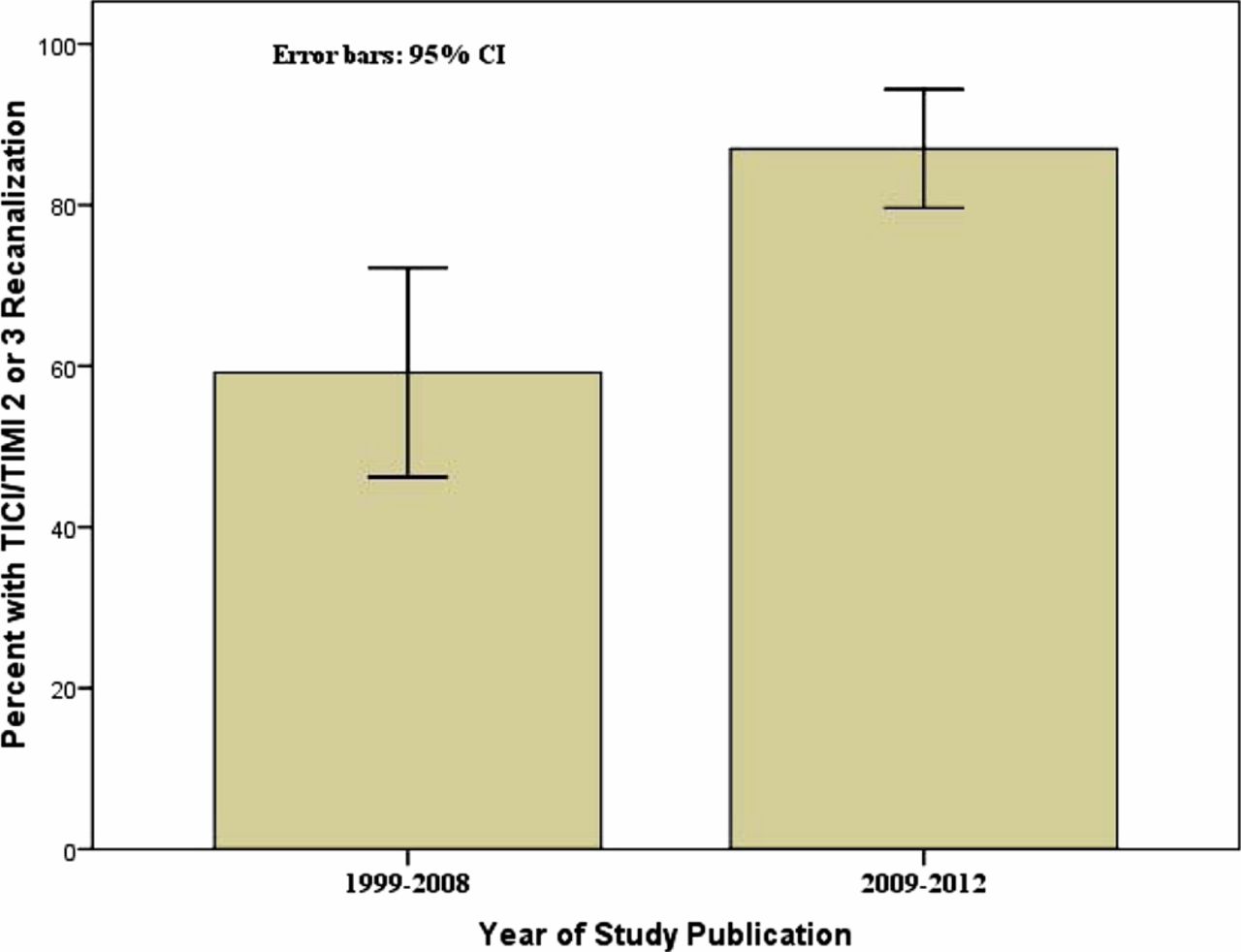
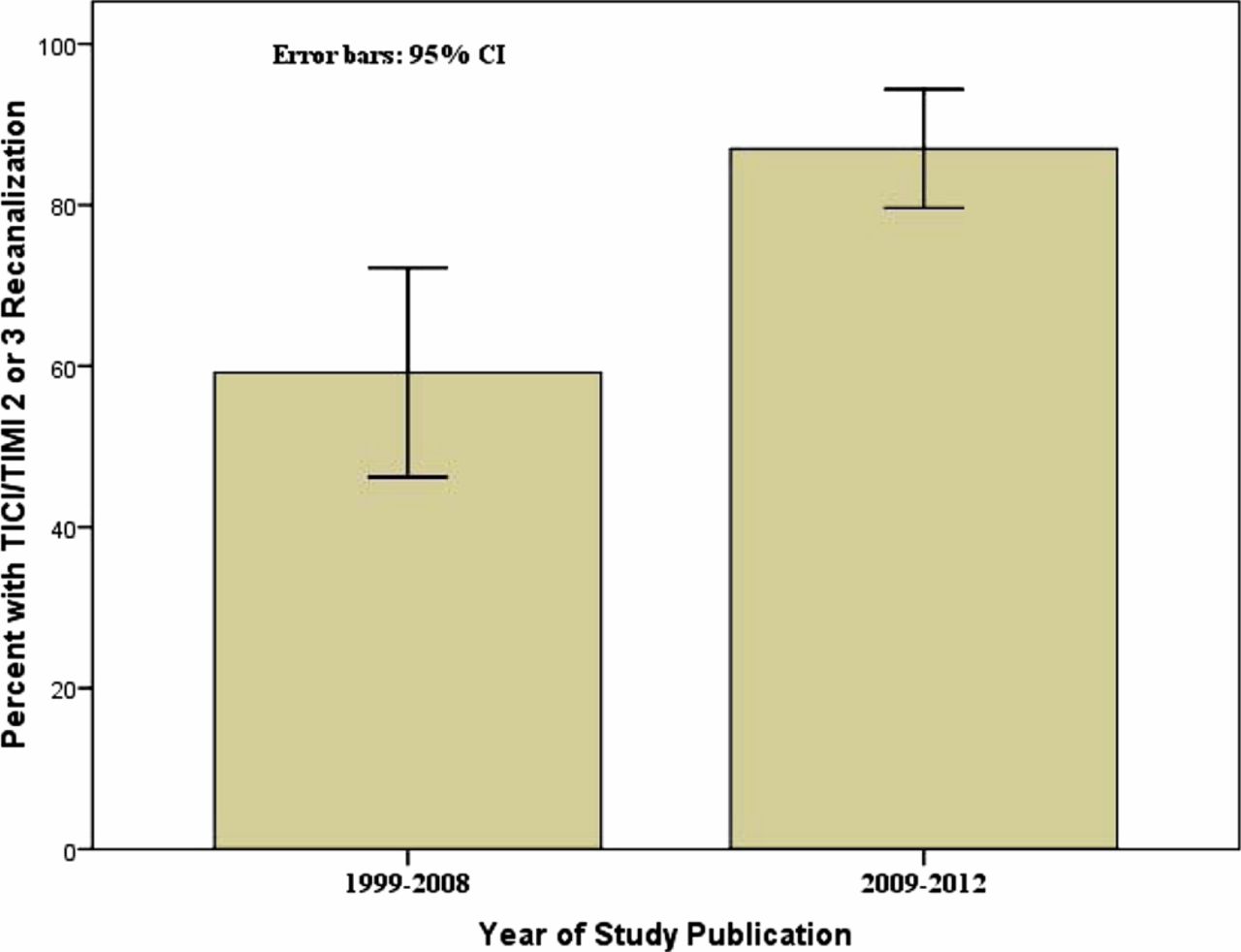
Bar graph demonstrating a significant improvement in mean recanalization/reperfusion from 1999–2008 to 2009–2012 (p=0.01). TICI, Thrombolysis in Cerebral Ischemia; TIMI, Thrombolysis in Myocardial Ischemia.

Scatterplot and best-fit line depicting no appreciable change in good outcomes at 90 days since 1995 (p=0.66). mRS, modified Rankin scale.

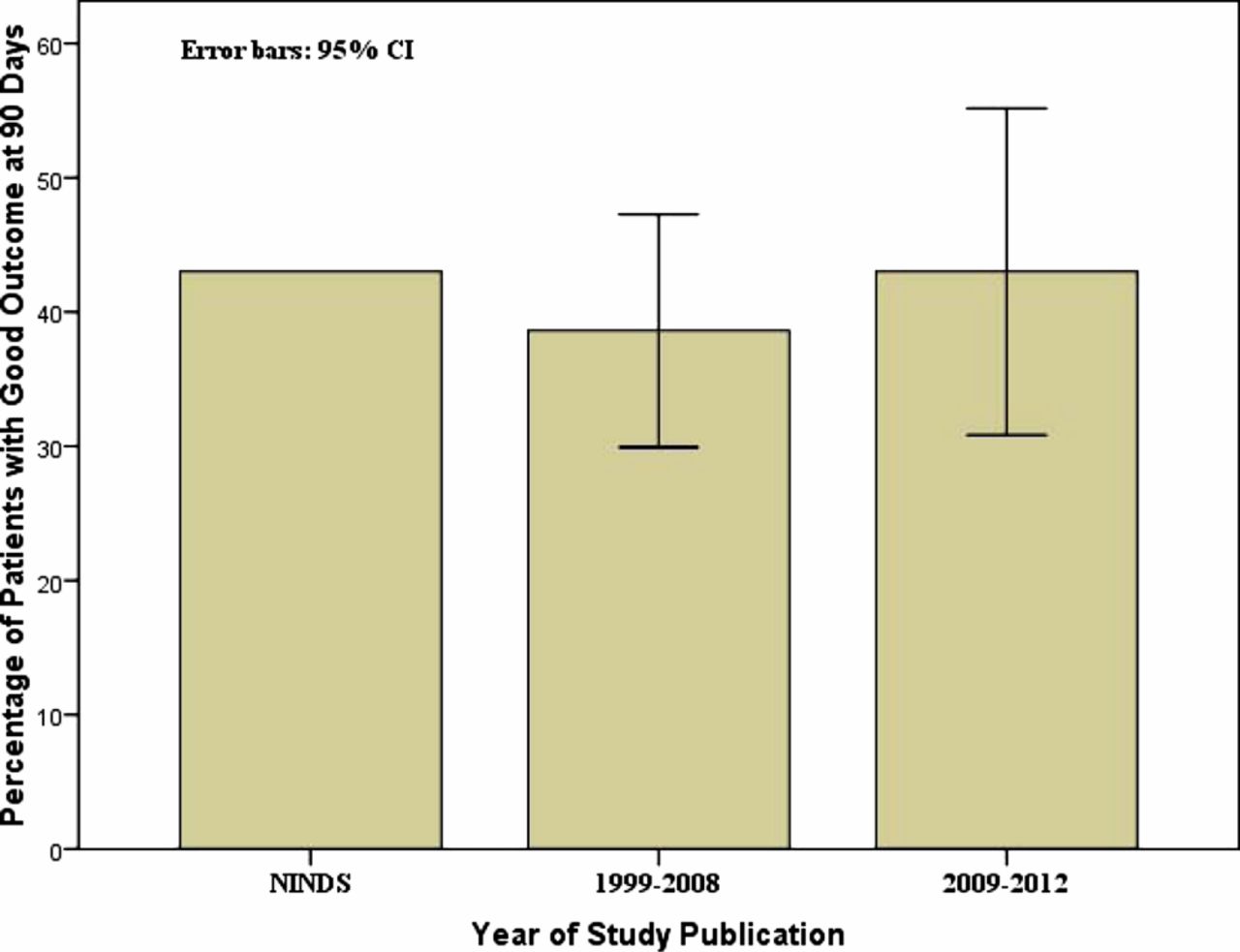
Bar graph depicting no appreciable change in good outcomes at 90 days since 1995 (p=0.75).

Scatterplot and best-fit line demonstrating no appreciable change in mortality over the last two decades (p=0.55).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
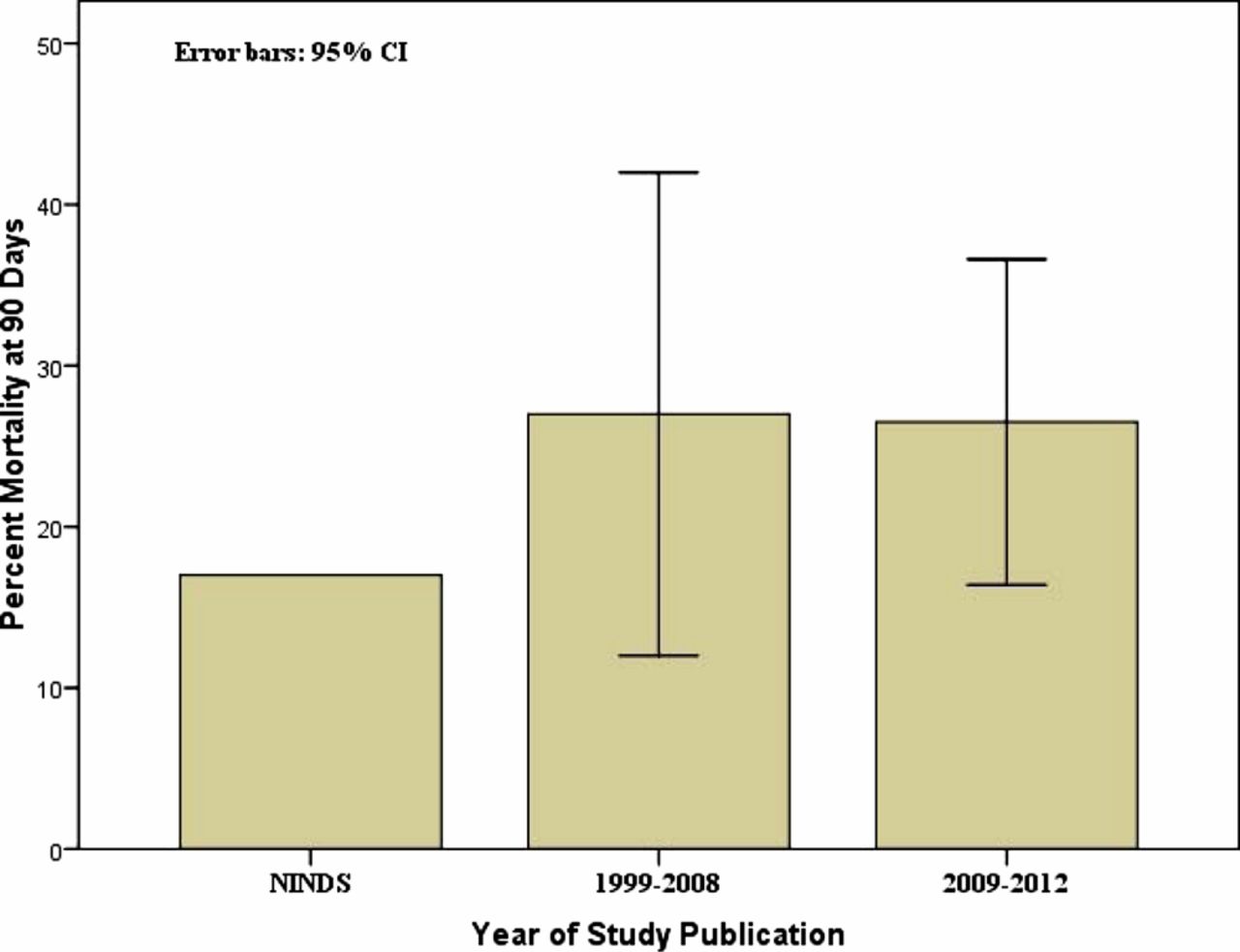
Bar graph demonstrating no appreciable change in mortality over the last two decades (p=0.70).
Discussion
Since 1995 the percentage of patients achieving TICI/TIMI 2 or 3 revascularization has increased substantially, with a strong statistically significant upward slope. The most recent prospective studies have demonstrated revascularization rates approximating 85%, while those a decade earlier demonstrated rates near 50%. This dramatic improvement appears to be secondary to improvements in intra-arterial techniques and devices designed to rapidly lyse or mechanically remove the offending thrombus. This success is despite an increase in the time from onset to treatment, and with stable stroke severity according to NIHSS, for patients undergoing intra-arterial intervention. Intravenous tPA, the only FDA-approved treatment with class 1 evidence, was approved based upon a mean time from symptom onset to treatment of 90 min, a time window substantially shorter than any of the intra-arterial trials that have followed. Later studies evaluating the benefit of intravenous tPA have demonstrated an inherent time limitation of 4.5 h after symptom onset.3 ,21 Furthermore, the limitations of systemic intravenous tPA in thrombolysis of long22 or dense23 thrombus have been reported and are probably present to some degree with intra-arterial administration of this medication.22 Newer generation thrombectomy devices, which can be navigated directly to the site of occlusion to physically disrupt, remove or aspirate the thrombus, are able to quickly recanalize occluded vessels and allow for restoration of perfusion. The Penumbra System (Penumbra; Alameda, California, USA) and Solitaire stent (ev3; Irvine, California, USA) represent two such devices that have shown excellent revascularization results (80–90%) in recent published studies15–17 and recent presentations.20 In addition, these devices have demonstrated encouraging safety results in single-arm studies when used beyond the 4.5 h time window10 ,12–13 ,15 and appear to harbor only slightly higher hemorrhage rates than intravenous tPA. The refinement of neurointerventional stroke devices and techniques is probably the major reason for the dramatic improvement in revascularization seen in acute stroke studies over the last 20 years.
Interestingly, however, improvements in clinical outcomes have not followed. Our analysis demonstrates a non-significant subtle upward slope of the best-fit line over the last 20 years with regard to good outcome. This lack of a corresponding clinical improvement is probably multifactorial, reflecting an increasing time from stroke onset to treatment and continued difficulties in identifying those patients who are likely to benefit from intervention. The observation that recanalization is not always a good surrogate marker for outcome has been indicated previously: several studies have demonstrated a strong relationship between time to revascularization and good outcome at 90 days, with delayed recanalization associated with poorer outcomes.10 ,12 ,15 ,24 ,25 It is interesting to note that the time to recanalization has also significantly, and dramatically, increased over the time course of this analysis, and therefore it may be that simply holding outcomes constant represents relative progress and success that can be achieved with faster treatments. These factors highlight the importance of randomized clinical trials. It may be that physiologic imaging, which has become a critical component of the patient selection process for many high volume stroke centers, will aid efforts to better identify appropriate patients. However, the data to support such a supposition are by no means conclusive; it remains possible that imaging selection primarily introduces treatment delays which lead to worse outcomes. Interestingly, only one of the reviewed studies (SARIS) used physiologic imaging (CT perfusion in this case) for all enrolled patients6 ,7 and, although a very small study, SARIS demonstrated the best clinical outcome rate of the studies evaluated.
The recent suspension of IMS III due to futility to show a clinical benefit comes at a time when there are significant challenges facing the investigators of large randomized trials. Concern has been generated regarding full reimbursement for use of stroke devices by the Center for Medicare and Medicaid Services (CMS) even though no class 1 data exist to support their use, as this may be limiting enrollment into randomized trials investigating these devices.26 ,27 The IMS III trial was halted after enrolling 656 of the designated 900 patients following 6 years of enrollment. The halting of IMS III appropriately raises serious concerns about the value of intra-arterial therapy as it was a well-designed prospective randomized trial. Unfortunately, the data from IMS have yet to be made available. Doubtless the information gleaned from this landmark trial will provide crucial information to the stroke community regarding the future of intra-arterial stroke therapy.
It should be emphasized that this analysis of recent prospective stroke trials has significant limitations inherent to its design. The trials that are compared have different criteria for enrollment, involve different treatment modalities, use different scales to assess revascularization success28 and, in one instance, measure good outcome at a different time. Specifically, only mRS 0–2 at 180 days7 instead of mRS of 0–2 at 90 days was available for one study. In addition, data from two trials (TREVO, START) are based on presentations at national meetings and have yet to be published as manuscripts. It is possible that the future publications of these trials will reveal different results from those indicated by the preliminary analyses. A statistical analysis of this manner on studies of different populations with different enrollment criteria is clearly inherently flawed. Furthermore, the calculations performed to generate the best-fit line and determine slope significance also lack validity given the nature of the data used to generate the fit line. In addition, we have assumed a linear best-fit in the analysis of each variable. Thus, it must be stated that this analysis is not intended to be a rigorous comparison of different trials to generate robust observations regarding treatment and outcome, but instead as a review to depict the general trends in commonly reported outcomes over the last two decades and to generate context as we consider detailed results and secondary analyses of the IMS III trial.
Conclusions
This review of prospective acute ischemic stroke trial results since 1999 indicates a substantial improvement in revascularization. However, in the setting of a significant increase in time to treatment onset, no appreciable change in good functional outcome was identified. While the results presented here indicate exciting progress in treatment of acute stroke over the last two decades, it is evident that there is much work to be done in translating improved recanalization to improved patient functional outcomes.
References
Footnotes
-
Contributors All authors contributed to the work presented through study design, manuscript composition and/or critical review.
-
Funding No funding was obtained for the completion of this manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; internally peer reviewed.