Article Text

Abstract
Background Hydration and anticoagulation are the standard of care for cerebral venous sinus thrombosis (CVST) but some patients remain refractory to medical management and warrant more aggressive therapy. Here we present the technique of endovascular transvenous manual aspiration thrombectomy (MAT) in six patients.
Objective Present an alternative technique for endovascular transvenous thrombectomy in a series of CVST patients.
Methods We reviewed the records of six patients with medically refractory CVST. Transvenous access via the femoral vein was used to advance an aspiration catheter of varying internal diameter (0.044, 0.054, 0.057, 0.070, 0.072) up to and through the thrombus. Tissue plasminogen activator was administered in select cases. Manual aspiration with a 20 ml syringe applied to the catheter hub was applied as the catheter was slowly retracted. Presentation, technique, and outcome were evaluated.
Results Clinical presentation included vomiting, dehydration, mental status changes, headaches, and acute motor deficits. On imaging, four of the six patients had hemorrhage, edema, and mass effect present before treatment, while two had edema only. All patients demonstrated continued deterioration despite early and aggressive medical anticoagulation therapy, warranting aggressive intervention. Aspiration of the superior sagittal sinus, transverse sinuses, straight sinus, sigmoid sinus, and internal jugular vein were performed in this series. There were no procedural complications. Revascularization was achieved in all instances. A modified Rankin Scale score of 1–3 was attained in 5/6 patients, while one patient died.
Conclusions In this series, transvenous MAT was a safe, simple, and effective revascularization technique to treat patients with CVST who remained refractory to medical management.
- Catheter
- Stroke
- Thrombectomy
- Technique
- Vein
Statistics from Altmetric.com
Introduction
Cerebral venous sinus thrombosis (CVST) is an uncommon form of stroke. Although large controlled studies have shown the benefit of anticoagulation, aggressive endovascular therapy may be necessary in select patients who fail medical management. Multiple endovascular methods have been described, including direct thrombolysis, angioplasty, and other methods of mechanical clot disruption or aspiration. It has been suggested that mechanical methods may have the lowest rate of procedure associated morbidity and mortality.1 Aspiration thrombectomy has been described to treat both arterial and venous thrombosis.2 A technique for manual aspiration thrombectomy (MAT) is described, as well as a series of six patients that underwent MAT with short term follow-up.
Patients and methods
In accordance with institutional review board approval and hospital protocol, we performed a retrospective review of CVST patients at our center. Our clinical database yielded 27 cases of CVST presenting to our institution between 2009 and 2012. Six of these 27 (22%) patients experienced medically refractory CVST, undergoing MAT. Table 1 outlines the demographics of the MAT patients. There was a female predominance, as has been reported previously.3 Presenting symptoms included headache, dysarthria, weakness, seizure, obtundation, vision changes, and mental status changes (table 2). Involved veins included the superior sagittal sinus (n=3), transverse sinus (n=3), internal jugular vein (n=1), sigmoid sinus (n=1), and straight sinus (n=1). Four of six patients had hemorrhage, edema, and mass effect or sulcal effacement on imaging while two of six patients had edema alone. Early and aggressive full anticoagulation remains the standard of care, and therefore the adult patients were treated with anticoagulation within 24 h of presentation in the form of intravenous heparin and hydration while the single pediatric patient was treated with subcutaneous lovenox, heparin, and hydration. Two patients, patient Nos 5 and 6, had endovascular therapy that was initiated before the partial thromboplastin time (PTT) was above 35 s due to early rapid neurological decompensation. All other patients demonstrated PTT values above 40 s, with three of six patients having preoperative PTT values above 60 s (table 3). Thus, for four of six patients, the PTT had achieved the goal of two times normal pretreatment values, as has been recommended in CVST studies.4 Despite medical management, all patients demonstrated marked clinical (progressive neurological deficit or lethargy) and radiographic (increased edema and hemorrhage) worsening, warranting more aggressive intervention.
Patient demographics and presentation
Presenting symptoms
Procedural information and outcome
Technique and patient outcome
Without stopping the intravenous heparin drip, a 5 F sheath was placed into the right common femoral artery to allow a diagnostic cerebral angiogram. After obtaining delayed runs to delineate the location of sinus occlusion, a 5 F diagnostic catheter was placed into the common carotid artery contralateral to the thrombus to allow repeat injections to gauge the effectiveness of therapy. In all cases, transvenous access was then obtained via the femoral vein and a 6 F shuttle sheath that was advanced to the most distal position technically possible in the internal jugular vein or, if possible, into the internal jugular vein–sigmoid sinus transition. This is the smallest diameter sheath which still allows the use of up to 0.072 inch inner diameter (ID) aspiration catheters. A triaxial system was then utilized to facilitate advancement of the aspiration catheter as far as possible into or even past the thrombus. Typically, the system consisted of a 0.054–0.072 inch ID aspiration catheter, a 0.021 inch ID microcatheter, and a 0.014 inch wire. In four of six patients, tissue plasminogen activator (tPA) was initially administered directly into the thrombus. The microcatheter was advanced through the thrombus, followed by administration of tPA as the catheter was slowly retracted through the entire clot over 10 min. tPA doses ranged from 10 to 40 mg and were based on the extent of clot and intracranial hemorrhage (ICH). Patient Nos 3 and 6 did not receive tPA due to the extent of ICH and initial success with MAT. After re-advancing the entire triaxial system into the thrombus, the microcatheter and wire were removed and a 20 ml syringe was attached to the hub of the aspiration catheter. Catheters included the 0.070, 0.057, and 0.044 distal access catheter (Concentric Medical, Inc, Mountain View, California, USA), 0.072 ReFlex catheter (Reverse Medical, Irvine, California, USA), and the 0.054 Penumbra reperfusion catheter (Penumbra, Inc, Alameda, California, USA) (see table 3). With the advent of larger catheters, preference was given to using the largest diameter aspiration catheter available. MAT was performed by retraction of the catheter through the thrombus with continuous manual aspiration using a 20 ml syringe that was immediately retracted maximally in each pass. If blood and clot immediately filled the syringe, it was repeatedly replaced and aspirated as the catheter was withdrawn. If thrombus occluded the catheter, the aspiration catheter was removed while maintaining continuous suction with the syringe. Three to ten passes were commonly needed to re-establish flow. If follow-up arterial control runs showed significant residual thrombus, the procedure was repeated. In all cases radiographic patency was achieved (figures 1 and 2). Large amounts of thrombus were aspirated into the syringe in all cases (figure 3). Procedural time varied from 1 to 2 h.
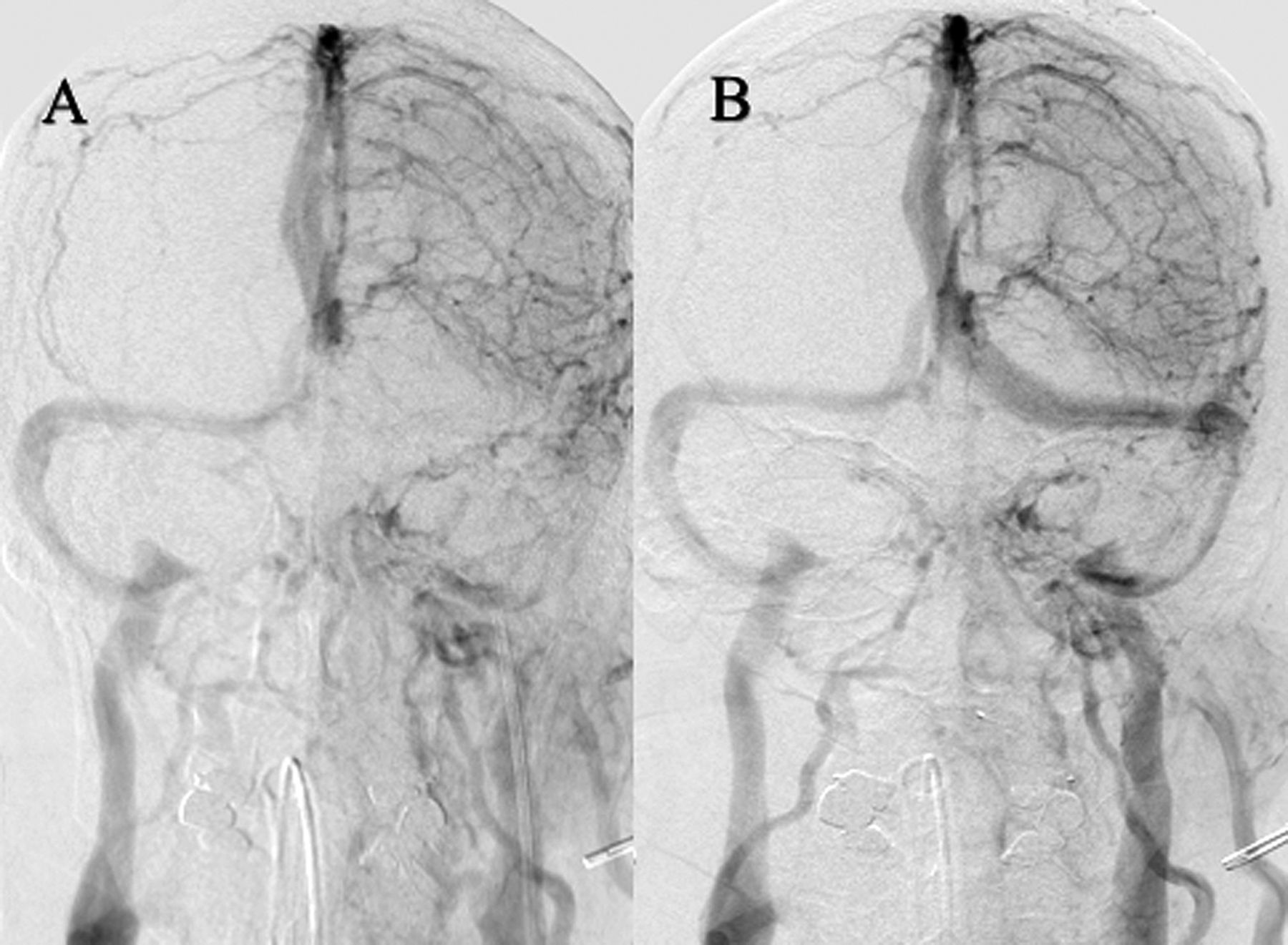
Venous angiography showing preoperative (A) and postoperative (B) runs in a patient undergoing manual aspiration thrombectomy of the left transverse sinus.
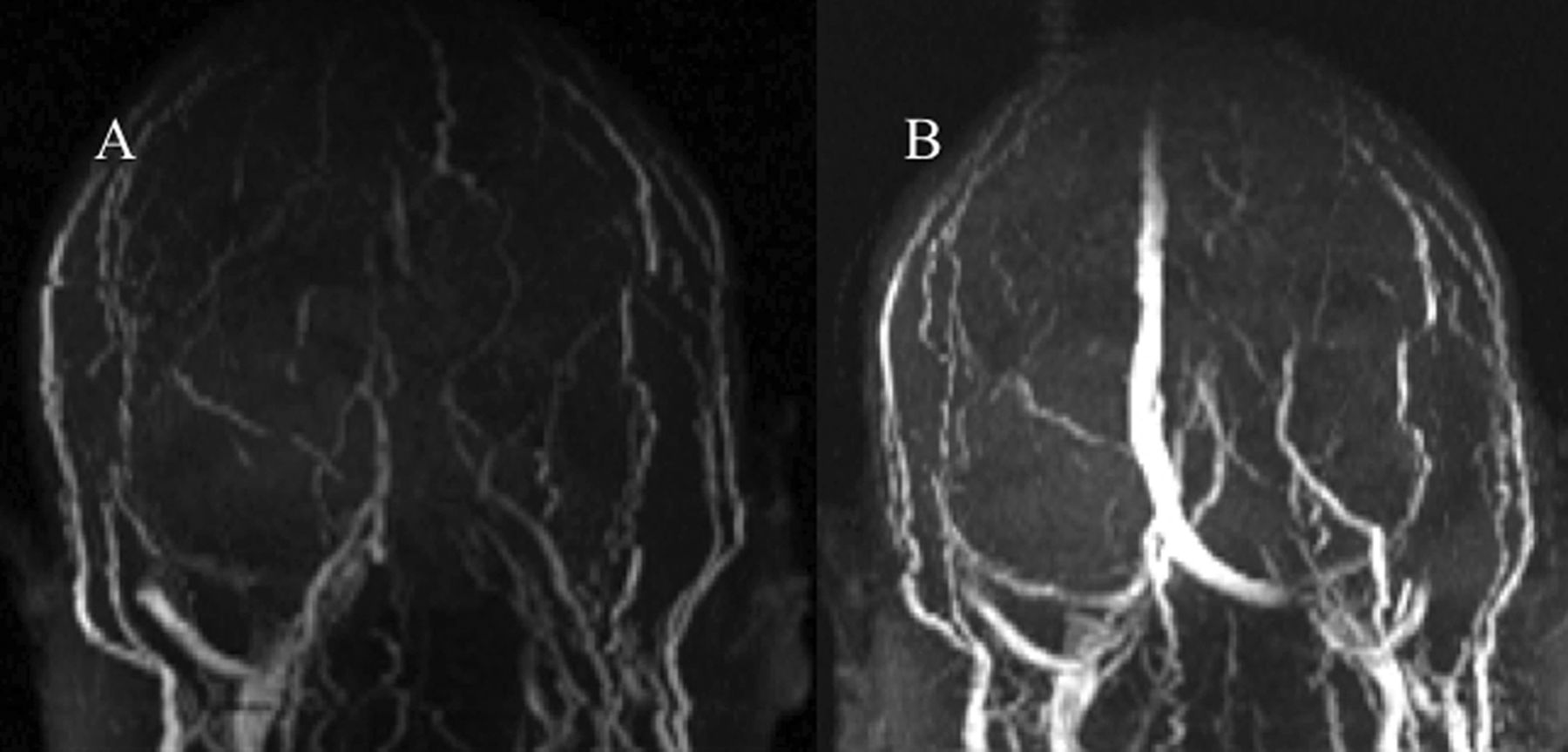
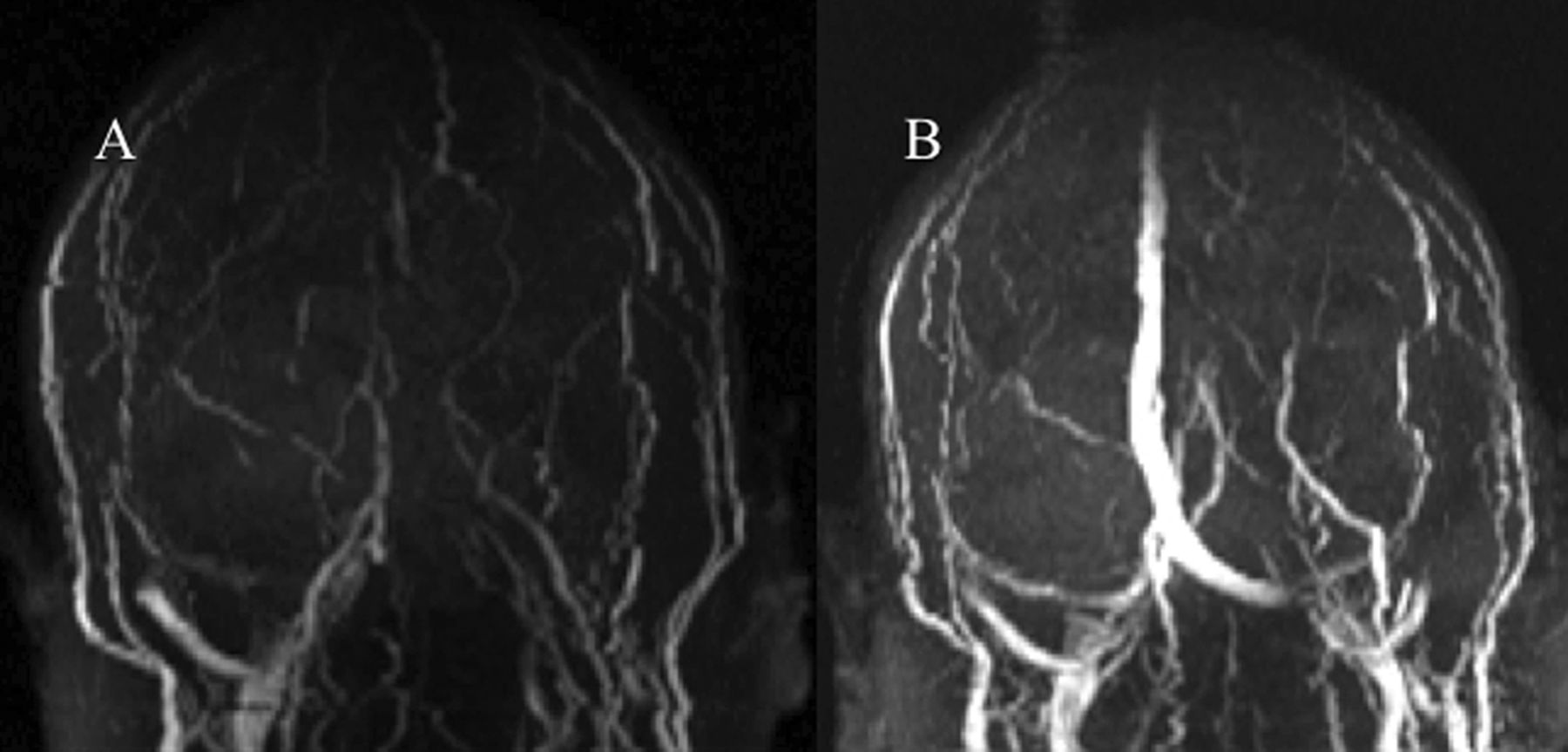
Preoperative (A) and postoperative (B) MR venography in a patient undergoing manual aspiration thrombectomy of the left transverse and superior sagittal sinuses.

{kind=link}
{kind=link}
{kind=link}
Thrombus removed from the cerebral sinus using the manual aspiration thrombectomy method.
Immediate clinical outcomes were as follows. Patient No 4 presented neurologically devastated and, despite successful venous sinus recanalization with MAT, showed no improvement in her examination and died 3 days later. Patient Nos 3 and 5 remained neurologically stable after treatment with no new hemorrhaging and mild to moderate improvement over the next several days, including improved mental status. Despite an interval increase in patient No 2's ICH the day after surgery, her neurological examination improved over subsequent days. The hemorrhagic progression appeared to be the evolution of her initial bleed, with no new sites of edema or hemorrhage noted. The continued hemorrhage postoperatively could have been related to the 40 mg tPA infusion. Patient No 1 initially exhibited a stable examination, however, several days later developed a middle cerebral artery occlusion that warranted a right frontotemporal decompressive craniotomy. This was felt to be due to her prothrombotic state and unrelated to the procedure. She experienced a gradual recovery over several weeks before discharge. Patient No 6 experienced an immediate improvement in her neurological examination postoperatively, despite some progression of her ICH over the following 48 hours. Long term patient outcome was assessed at 3 months (table 3) using a 0–6 modified Rankin Scale score.
Discussion
While CVST has existed as a documented entity in the medical literature since the 19th century,5 ,6 there is still much to be learned about the pathophysiology and treatment of this condition.6 ,7 This is largely attributable to the rare nature of CVST, which constitutes only 0.5% of stroke cases.3 ,6 As with other thrombotic processes, causes are related to blood stasis, vascular wall damage, and hematologically hypercoaguable states, with most cases involving multiple thrombotic risk factors.3 ,6 ,8 Commonly implicated causes include genetic causes of hypercoaguability, acquired states of hypercoaguability, severe infections, complications related to pregnancy or peripatrum complications, and oral contraceptive use.3 ,6 ,8 The resulting cerebral injury has been proposed to occur via both venous stasis causing vasogenic edema and hemorrhage, as well as impaired CSF flow with resulting hydrocephalus.6
The standard of care for treatment of patients with CVST involves initial medical therapy with aggressive hydration and systemic anticoagulation with heparin, with a target of attaining a PTT of twice the normal pretreatment levels.1 ,4 ,6 ,8 ,9 Retrospective review has suggested that systemic anticoagulation is relatively safe in CVST patients, even in the presence of hemorrhage,1 although fatalities have been reported.10 It has been suggested that the most common reason for CVST patient deterioration is insufficient anticoagulation therapy.7 While meta-analysis of two randomized prospective studies showed the expected trend of reduced death and death or dependent disability in patients treated with anticoagulation compared with placebo, it failed to reach statistical significance.9 The largest randomized, prospective study included in this analysis still showed a 13% incidence of death or dependency for those treated with anticoagulation alone.11 Furthermore, there is a lack of consensus for the appropriate therapy for patients with sufficient PTT levels experiencing continued deterioration or patients undergoing rapid clinical deterioration. While these clear limitations are present in the data, clinical deterioration in the setting of sufficient anticoagulation may warrant more aggressive therapies.6–8
A wide variety of methods have been described to address medically refractory CVST by using transvenous endovascular interventions, including direct administration of thrombolytics,12–14 angioplasty,15 ,16 and various methods to mechanically disrupt clots,17 ,18 including those that use rheolytic stream and pneumatic suction devices. A general lack of well controlled trials in the literature complicates therapeutic decision making.6 ,7 ,12 While direct thrombolysis was the earliest reported endovascular intervention,14 more recent reports raised concern about the risk of hemorrhage.1 A recent prospective study with 20 patients found that the risk of direct thrombolytics was significant, particularly in patients with large infarcts or impending herniation.19 A retrospective review concluded that, provided what seems to be a greater risk of hemorrhage associated morbidity and mortality with thrombolytics, systemic anticoagulation with mechanical thrombectomy may be more appropriate.1 At our institution we initially viewed intravenous tPA with MAT as a standard of care for CVST as it was thought to aid in recanalization and MAT itself. However, our empirical experience with both arterial and venous MAT has led us to believe that the additional benefit is uncertain and may not outweigh the risk.
While it has been suggested that mechanical thrombectomy therapies may be superior to direct thrombolytic therapy due to a decreased risk of iatrogenic hemorrhage, the superior mechanical method remains unclear. Balloon angioplasty with or without stent deployment may be beneficial in certain situations,15 ,16 although there is scant literature in support of this method. Other groups have reported the use of rheolytic systems and the Penumbra system.17 ,18 ,20 In a series of 13 patients using an Angiojet rheolytic device, all patients had continued radiographic patency of recanalized vessels at an average 7 month follow-up. Clinical follow-up was available in nine of the 13 patients, with modified Rankin Scale scores of 0 in four patients, 1 in three patients, and 6 in two patients. Similar success has been reported with the Penumbra device.2 In our small series using MAT, we have shown that manual clot removal can be attained using a 20 ml syringe with a large bore catheter. This method allowed us to achieve partial or complete venous sinus patency in all patients undergoing the procedure. It should also be noted that thrombolytics were used along with MAT in four of six patients, thus making it an adjunctive recanalization procedure in most cases. However, as we gained comfort with the technique, MAT was used without thrombolytics, resulting in similar recanalization rates and favorable outcomes, as seen in patient Nos 3 and 6. It should be noted that there was no perceivable technical difference between the procedures done with and without thrombolytics. The clot aspirated easily and the catheters advanced without significant difficult in all patients.
The novelty of this procedure lies in its potential for speed and simplicity. The stated procedural times included arterial access, thrombolytic administration, and multiple arterial runs to assess for progress. In reality, the two procedures foregoing thrombolytics required only 5 and 10 min, respectively, of aspiration to recanalize the sinus. Thus procedural times have the potential to be drastically shortened. The thrombus itself was surprisingly easy to aspirate in all cases and required no mechanical disruption. Foregoing the use of mechanical aspiration pumps or other expensive products with complicated mechanisms may reduce cost. Avoiding bulky devices that are relatively rigid and not designed for the intracranial space, such as the Angiojet, may facilitate widespread application. Trackability and distal access have not been a problem as the aspiration catheters have easily advanced up to, through, and beyond the clot. The only consistent technical limitation was the length of the aspiration catheter, which limited distal access in one case.
Conclusion
In this series, MAT was a feasible venous sinus recanalization technique that produced favorable outcomes. With increasing comfort in the technique, the intrinsic simplicity of using nothing more than a catheter and syringe, the advent of larger and more trackable aspiration catheters, and the hemorrhagic risk of thrombolytics, initial attempts at standalone venous MAT may be warranted. Due to the lack of well controlled data examining the efficacy, selection, and cost–benefit of the various techniques to treat CVST with endovascular intervention, as well as the numerous techniques available, a multicenter randomized controlled trial seems to be warranted.
References
Footnotes
-
Contributors BTJ: design, data collection, manuscript drafting and revision, and technique development. LMB: design, data collection, and manuscript drafting. MJ: design, data analysis, and manuscript revision. ZFS: design, data analysis, and manuscript revision. TGJ: design, data analysis, manuscript revision, and technique development.
-
Competing interests None.
-
Ethics approval The study was approved by the institutional review board.
-
Provenance and peer review Not commissioned; externally peer reviewed.