Article Text

Abstract
Background Onyx is a liquid non-adhesive viscous embolic agent ideal for slow targeted injections which is currently approved for the treatment of intracranial aneurysms and arteriovenous malformations.
Methods We performed a single-center retrospective analysis of consecutive patients who underwent off-label use of Onyx as the single embolic agent for the treatment of traumatic or infectious pseudoaneurysms involving the cerebral or cranial vasculature.
Results A total of nine pseudoaneurysms treated by Onyx embolization were identified. Six of the pseudoaneurysms were post-surgical, one of the pseudoaneurysms was traumatic and two were infectious in nature. The mean pseudoaneurysm size was 5.9 mm (range 2–10 mm). Onyx-34 was used in all cases. Following treatment there was complete exclusion of all pseudoaneurysms including their inflow and outflow zones.
Conclusions Our experience demonstrates the efficacy and applicability of the use of Onyx in the treatment of complex traumatic and mycotic pseudoaneurysms involving the cerebral and cranial vascular tree.
- Aneurysm
- Liquid Embolic Material
- Technique
- Hemorrhage
- Infection
Statistics from Altmetric.com
Introduction
Pseudoaneurysm formation can occur in the setting of trauma or infective endocarditis with fatal complications.1 Histologically, these lesions are not true aneurysms as they are characterized by incomplete disruption of the vessel wall. While the frequency of pseudoaneurysm formation is relatively low, the fragile structure of these lesions makes them particularly susceptible to rupture. Timely and safe embolization of these lesions must often be considered, especially given the high mortality rate after rupture.2 While open surgery has been the traditional approach to this disease, endovascular surgery offers a safe and efficacious alternative.3 ,4
Onyx is a liquid non-adhesive viscous embolic agent ideal for slow targeted injections. Its use has been established in the treatment of intracranial berry aneurysms5 ,6 and arteriovenous malformations.7 More recently there have been reports of its use in the treatment of peripheral vascular pseudoaneurysms8 ,9 as well as reports describing the successful use of Onyx in cerebral pseudoaneurysms.10–13 We present nine consecutive cases of traumatic or infectious (‘mycotic’) distal aneurysms treated successfully with Onyx embolization.
Methods
The procedures were performed on a biplane angiographic unit (Neurostar and Axion Artis; Siemens Medical Solutions, Erlangen, Germany) under general anesthesia. Informed consent was obtained. Access was achieved via a transfemoral approach using standard coaxial technique. All procedures were done with continuous infusion of heparin 4000 units/l through the guide catheter. Systemic anticoagulation was avoided when possible due to the hemorrhagic nature of the disease. Diagnostic angiography was performed with selective positioning of a 5 F MPC Envoy guide catheter (Cordis Endovascular, Miami Lakes, Florida, USA) in the internal and external carotid arteries. A Marathon or an Echelon-10 microcatheter (ev3 Neurovascular) was then advanced coaxially to the afferent limb of the aneurysm. Microcather angiography was used to confirm optimal positioning. The microcatheter was then flushed with 5 ml of saline followed by enough volume of dimethyl sulfoxide (DMSO) to fill the microcatheter dead space. Under road-mapping, Onyx-34 was injected in all cases. Injection was done over 60–90 s to fill the microcatheter and displace the DMSO. Onyx was then slowly introduced using a ‘thumb-tapping’ technique to allow the formation of a ‘plug’ and facilitate antegrade flow of the embolic agent, as previously described.14
Results
We retrospectively analyzed the use of Onyx in nine patients (eight men) who presented with pseudoaneurysms between June 2006 and May 2010. The mean age of the patients was 46 years (range 19–74) and the mean size of the aneurysms was 5.9 mm (range 2–10). Six of the aneurysms developed postoperatively, one was related to a gunshot wound to the face and the other two aneurysms occurred in the setting of infective endocarditis. The two cases of mycotic aneurysm were initially managed with antibiotics. In case 2, the aneurysm grew from 2 mm to 6 mm despite antibiotic use. Embolization was pursued in case 8 due to a high level of concern for aneurysmal rupture in the setting of chronic anticoagulation (which the patient required for systemic lupus erythematosus-associated antiphospholipid antibody syndrome). Three of the patients presented with subarachnoid hemorrhage (cases 1, 5 and 7). Five of the aneurysms were intracranial. Three of the aneurysms occurred on distal branches of the anterior cerebral artery (ACA) whereas the other two intracranial aneurysms occurred on distal branches of the middle cerebral artery (MCA). The extracranial aneurysms involved the extracranial carotid artery (ECA) territory. Two of the aneurysms occurred on the descending palatine artery, one on the lingual artery and one aneurysm occurred on the internal maxillary trunk. The patient characteristics are summarized in table 1.
Characteristics and outcomes of patients with pseudoaneurysm formation treated by Onyx embolization
None of the cases was considered suitable for vessel reconstruction with stent and/or coils. Complete embolization was achieved in all nine cases with a single procedure. Following treatment there was complete exclusion of all aneurysms including their afferent and efferent limbs (figures 1⇓–3). The treatment of one ACA aneurysm was complicated by a distal MCA embolus (in the setting of proximal balloon occlusion for flow control) which was subsequently nearly completely recanalized after mechanical embolectomy and resulted in only mild hemiparesis. The treatment of an anterior temporal aneurysm was complicated by a wire perforation resulting in mild contrast extravasation without any clinical consequences (case 2). Follow-up imaging was available for five of the patients (cases 2, 3, 4, 5 and 8) with CT angiography or MR angiography and showed no recurrence of the aneurysm.
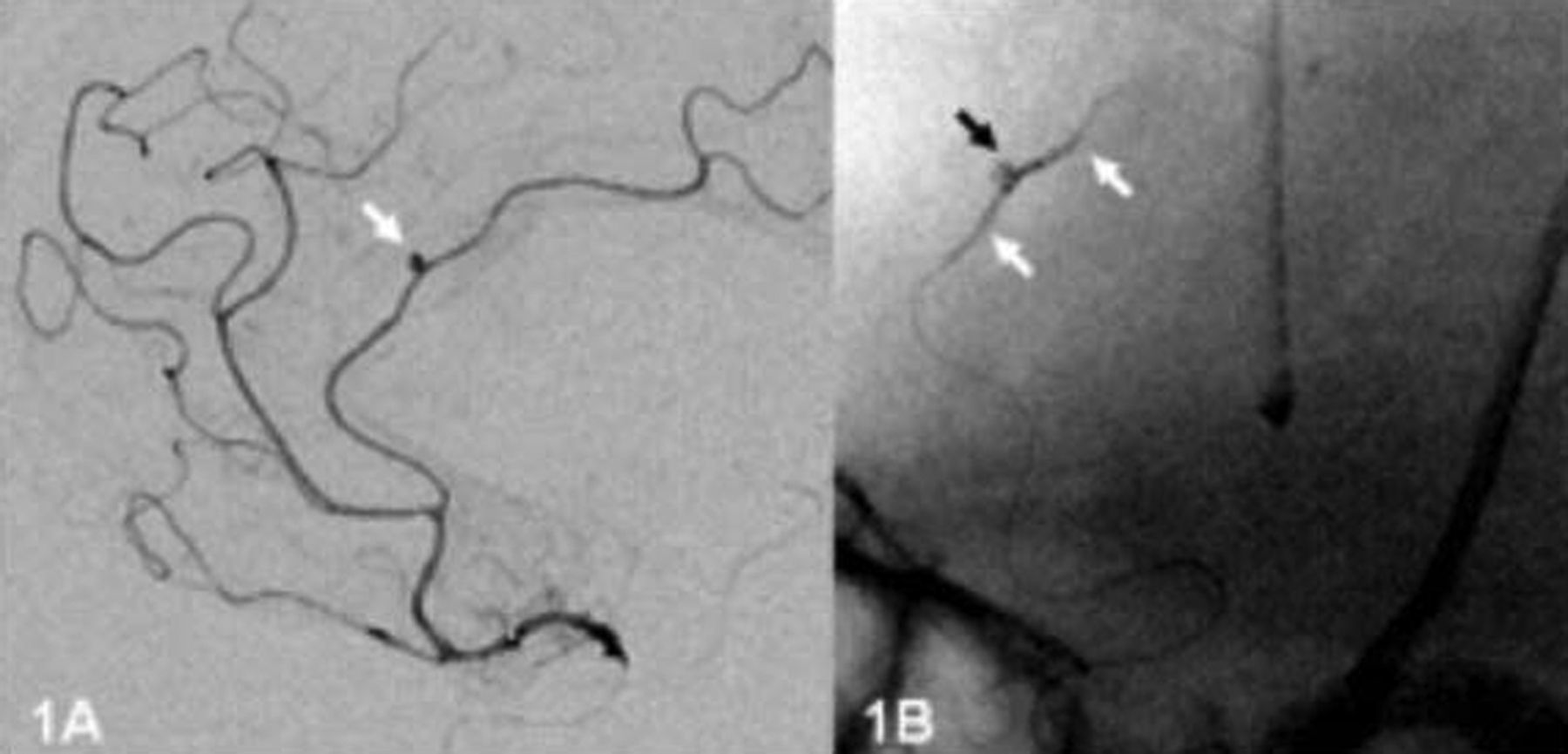
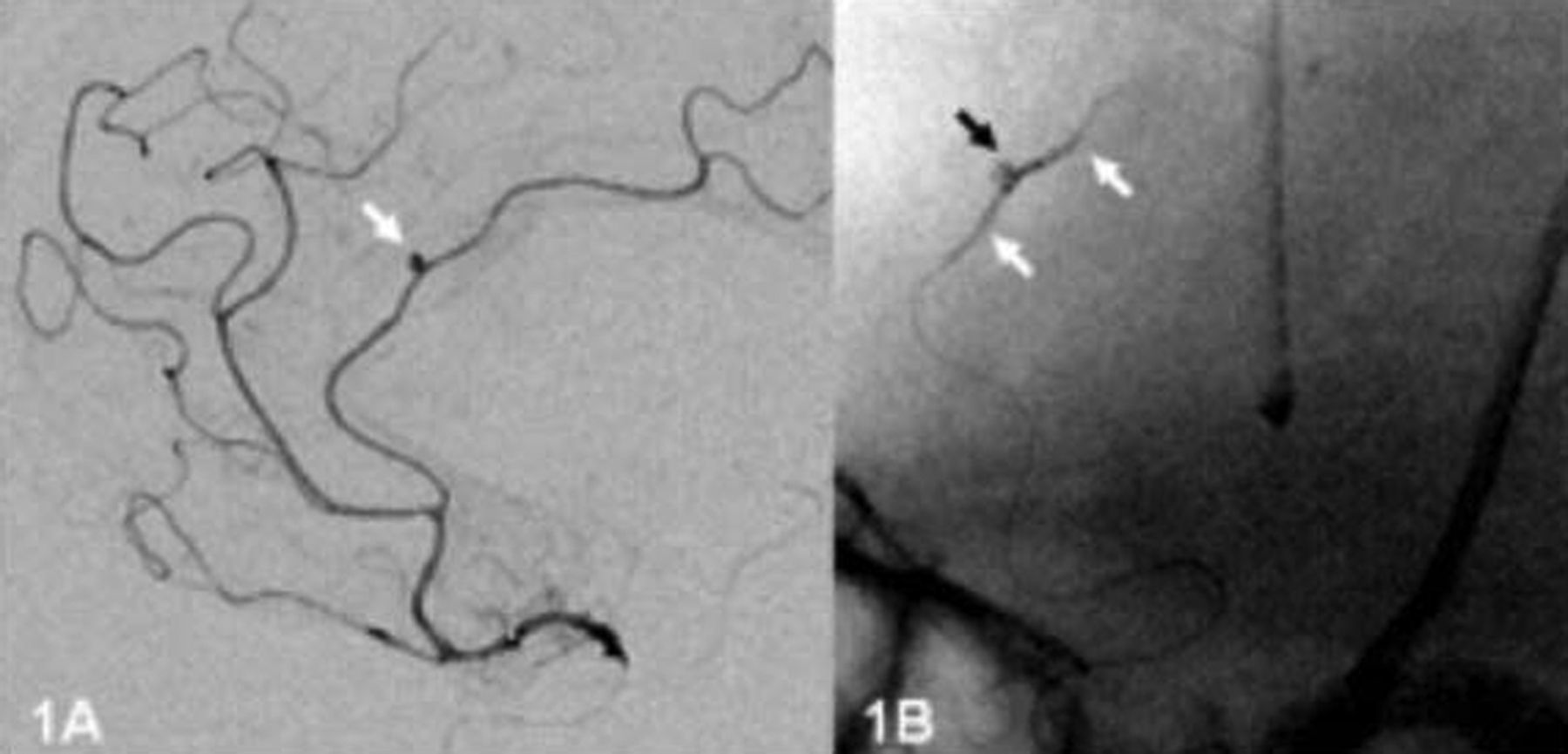
(A) Pretreatment angiography and (B) post-treatment native images of the Onyx cast for case 1. Note the dense penetration of the embolic agent into the pseudoaneurysm as well as the afferent and efferent limbs.

(A) Pretreatment angiography and (B) post-treatment native images of the Onyx cast for case 2. Note the dense penetration of the embolic agent into the pseudoaneurysm as well as the afferent and efferent limbs.

{kind=link}
{kind=link}
{kind=link}
(A) Pretreatment angiography and (B) post-treatment native images of the Onyx cast for case 3. Note the dense penetration of the embolic agent into the pseudoaneurysm as well as the afferent and efferent limbs.
Illustrative cases
Case 1
A 74-year-old patient with progressive recurrent left frontal and corpus callosum glioblastoma underwent resection. Several days after surgery the patient became less responsive. A CT angiogram revealed narrowing of the ACA vessels and a conventional angiogram revealed a 2 mm aneurysm of the distal pericallosal branch of the left ACA (figure 1A). Complete obliteration of the pseudoaneurysm was achieved after Onyx embolization (figure 1B).
Case 2
A 61-year-old patient was diagnosed with aortic and mitral valve endocarditis due to Streptococcus sanguinis. A CT angiogram demonstrated a cerebellar hemorrhage as well as a 2 mm mycotic aneurysm involving the anterior temporal branch of the right MCA. The patient was discharged home on intravenous antibiotics but a repeat CT angiogram and angiography 2 weeks later showed that the aneurysm had grown to 6 mm in size (figure 2A). The patient underwent successful Onyx embolization with complete obliteration of the lesion (figure 2B).
Case 3
A 62-year-old patient developed massive bleeding from the oral cavity after resection of a recurrent left soft palate squamous cell carcinoma. An angiogram showed a 1 cm pseudoaneurysm of the left external carotid trunk distal to the origin of the lingual artery and proximal to the origin of the posterior auricular branch (figure 3A). Onyx embolization was performed with full obliteration of the lesion and preservation of flow to the distal internal maxillary artery via anastomoses (figure 3B).
Discussion
Onyx is a non-absorbable and non-adhesive embolic material approved for the treatment of cerebral arteriovenous malformations. A growing number of studies have demonstrated the safety and efficacy of off-label use of this agent in treating other types of vasculature lesions including spinal dural arteriovenous fistulas,14 pediatric lesions15 and head and neck lesions.16 Here we describe a case series further extending the use of Onyx in the management of infectious and traumatic pseudoaneurysms.
In our experience, this approach is a safe and durable alternative to other endovascular approaches or open surgery. The one significant complication we report (case 7) was related to the lack of anticoagulation in the setting of balloon inflation for flow control as opposed to the use of Onyx itself, that is, the infarct was from balloon thromboembolus. Since then we have modified our technique to include an intravenous heparin bolus before Onyx use if a balloon is required. Interestingly, we did not identify any strokes distal to the vascular territory that we embolized. We suspect that this was due to the presence of collateral flow. In our experience, the use of Onyx is more precise in achieving proximal occlusion than N-butyl cyanoacrylate (NBCA) or coils.
The friable nature of pseudoaneurysmal blood vessels may result in rupture and high mortality.1 In the case of unruptured infectious intracranial aneurysms, intravenous antibiotics may be sufficient to treat the vascular anomaly but the aneurysm can grow in size or new aneurysms may form.17 While the risk of rupture can be low (<2%), the rate of mortality after rupture can be high (25–80%).18 If serial angiography demonstrates an aneurysm that is not regressing or is causing mass effect, further intervention is required.19 Open surgery has been the historical treatment of choice. Surgery can be challenging given the friable nature of the aneurysm which often lacks a satisfactory aneurysmal neck for clip placement. Many of our patients were quite ill due to concurrent infection or malignancy, so the less invasive nature of endovascular embolization seemed to be more favorable.
Endovascular surgery is an emerging approach for the treatment of pseudoaneurysms, particularly in the case of patients at high surgical risk or for surgically inaccessible or multiple lesions. The friability of infected parent vessels and the distal location of these aneurysms have led to parent artery occlusion as a favored approach. Early studies of this approach involved the use of detachable coils with positive results,3 although recurrence of aneurysm formation was observed. Coil placement can lead, on rare occasions, to infection and abscess formation.20 ,21 Furthermore, the small size and atypical morphology of pseudoaneurysms may not be able to accommodate standard coil sizes. Coils have been used adjunctively with stents, but neither technique is feasible in the treatment of distal aneurysms. Furthermore, the need for antiplatelets after stent placement can be prohibitive in cases of ruptured aneurysms.
Liquid embolic agents such as Onyx and NBCA can be delivered downstream of deployment and are unique in their ability to occlude small and distal vessels. NBCA is non-absorbable and adhesive, which allows for directed and controlled embolization. Unfortunately, polymerization occurs quickly and the microcatheter may become glued to the site of deployment.22
Onyx is a non-absorbable and non-adhesive embolic agent with a long precipitation time, allowing for more precise control. This may result in more complete embolization of the pseudoaneurysm including its afferent and efferent limbs, which may be crucial in preventing retrograde filling of the lesion via collateral flow resulting in additional growth and/or rupture. Furthermore, Onyx is highly visible under fluoroscopy and can therefore be injected under direct visualization in a slow and precise manner.
Onyx embolization of pseudoaneurysms has been reported in the kidney,23 pancreas24 and subclavian9 artery. The use of Onyx in pseudoaneurysms in the head and neck has been described in several case reports.11 Our study provides further evidence supporting this treatment option for a rare but potentially catastrophic disease.
References
Footnotes
-
Contributors APJ: drafting/revising the manuscript and acquisition of data. JCP: drafting/revising the manuscript and analysis or interpretation of data. RGN: drafting/revising the manuscript, analysis or interpretation of data and study concept or design.
-
Competing interests RGN is a member of the Scientific Advisory Boards for Concentric Medical, ev3 Neurovascular, CoAxia, Rapid Medical and Neurointervention. JCP is a consultant for ev3 Neurovascular.
-
Ethics approval Ethics approval was obtained from the Institutional Review Board at Massachusetts General Hospital.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.