Article Text

Abstract
A young woman with factor V Leiden thrombophilia presented with headache due to thrombosis of the right transverse sinus (TS) and superior sagittal sinus. Despite appropriate anticoagulation, she experienced worsening headache, progressive neurologic deficits and spontaneous subarachnoid hemorrhage. Endovascular therapy was therefore undertaken. A 6 mm Solitaire FR device was deployed in the TS and withdrawn in a stepwise fashion, resulting in complete recanalization of the sinus. Her headache improved and her neurologic deficits resolved. Endovascular therapy for cerebral venous sinus thrombosis is currently recommended only for those patients with deterioration despite appropriate anticoagulation. The thrombus burden is usually high in this subset of patients, and recanalization can be challenging with currently available endovascular techniques. This is the first report of cerebral venous sinus thrombectomy with the Solitaire FR device, which may offer another option for those patients requiring endovascular treatment.
Statistics from Altmetric.com
Background
Cerebral venous sinus thrombosis typically has a favorable prognosis, but is occasionally associated with neurologic decline despite appropriate treatment with anticoagulation.1 In such cases, endovascular therapy can be considered.2 However, multiple techniques have been reported including local thrombolysis,3 rheolytic thrombectomy4 ,5 or aspiration thrombectomy.6 Furthermore, cerebral thrombectomy devices continue to evolve, as evidenced by the recent introduction of the newest ‘Stentriever’ devices.7 This case illustrates the first reported use of the Solitaire FR thrombectomy device (Covidien Neurovascular, Irvine, California, USA) to successfully treat progressive cerebral venous sinus thrombosis despite adequate anticoagulation.
Case presentation
A 24-year-old woman with a history of migraine presented to an outside hospital with an atypical headache. Her pain worsened and MRI revealed thrombosis of the superior sagittal sinus and right transverse sinus (TS). The examination was normal except for bilateral papilledema. A laboratory investigation for thrombophilia revealed a factor V Leiden mutation. She was treated with unfractionated heparin and transitioned to warfarin, and was discharged with persistent pain but no neurologic dysfunction. However, she returned several days later after her headache worsened and she developed intermittent diplopia. On examination she now exhibited a visual field defect in the right eye. Despite treatment with acetazolamide, her condition continued to deteriorate with a progressive left VI nerve palsy and headache which she now rated 10/10. A repeat MRI showed new cortical vein thrombosis and a small subarachnoid hemorrhage. Endovascular therapy was therefore undertaken.
Treatment
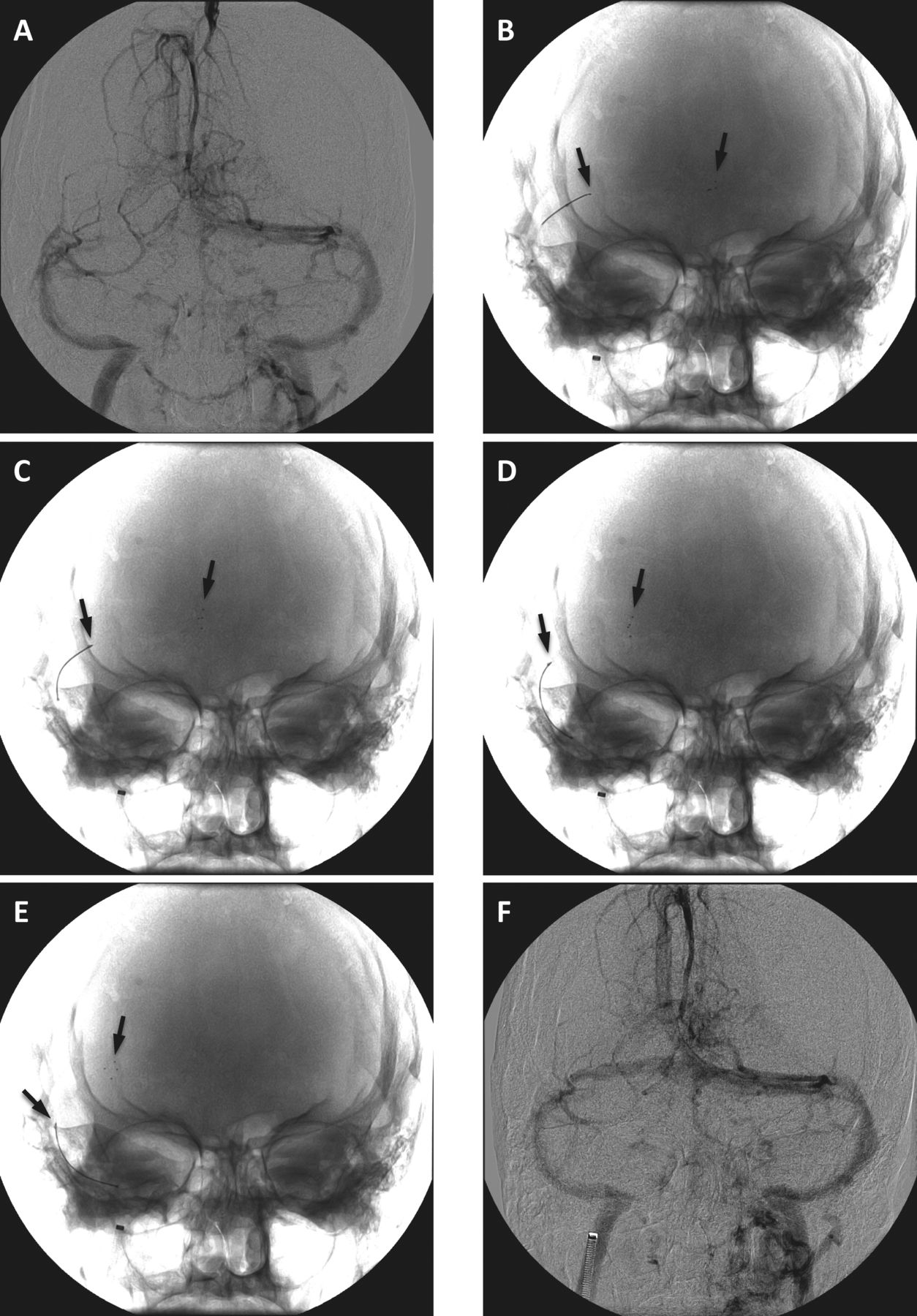
Initial angiography revealed thrombosis and occlusion of the right TS (figure 1A) and portions of the superior sagittal sinus, with significant collateral venous drainage. A 6 F Shuttle sheath was introduced transfemorally and navigated to the right internal jugular vein. A 0.027 inch microcatheter was placed in the thrombus in the right TS and a 4×20 mm Solitaire device was deployed and left in place for 5 min before being retracted into the sheath during manual aspiration through the side port of the sheath with a 60 ml syringe. A small amount of thrombus was recovered, but the sinus remained occluded. Next, 5 mg tissue plasminogen activator was infused into the TS without significant angiographic change. A 6×30 mm Solitaire device was then deployed across the torcular, left in place for 5 min, then retracted several centimeters and again left in place for 5 min. This process was repeated until the device entered the sigmoid sinus (figure 1B–E). The device was then retrieved into the sheath during simultaneous manual aspiration. Angiography revealed recanalization of the right TS (figure 1F).
{kind=link}
(A) Initial left vertebral artery angiogram showing complete occlusion of the right transverse sinus (TS) in the late venous phase. (B–E) The 6 mm Solitaire FR device was initially deployed in the torcular and right TS (B), and was subsequently withdrawn through the thrombus in a stepwise fashion with 5 min pauses at each position (C–E). The arrows indicate the proximal and distal ends of the device. (F) Final left vertebral artery angiogram showing recanalization of the right TS.
Outcome and follow-up
Immediately after the procedure the patient reported persistent headache but by the next day she rated her pain as 2/10. Palsy of the VI nerve resolved over the ensuing 2 days and her vision subjectively improved. She was discharged on postoperative day 3 with aspirin and warfarin. At three month follow-up, all symptoms had completely resolved.
Discussion
This patient exhibited clinical deterioration despite adequate anticoagulation, and subsequent endovascular therapy provided a good clinical result. There have been numerous reports of endovascular treatments for venous sinus thrombosis but, to my knowledge, this is the first report of the use of the Solitaire FR device (or any Stentriever) for this purpose.
Technically, the larger (6 mm) Solitaire device performed much better than the smaller (4 mm) device. Initial deployment of the smaller device did not even result in a temporary channel through the thrombus. In contrast, the 6 mm device immediately re-established flow, and persistent recanalization was observed after retrieving it. This difference may be attributable to size and also to the difference in radial force—the 6 mm device has more than twice the radial force of the smaller device in a 4 mm vessel (Covidien Neurovascular, internal testing). As thrombus in the dural sinus is likely to be organized and highly elastic, more radial force may be necessary to create a channel and to achieve recanalization. Additionally, the 6 mm device may have been successful because it was withdrawn in a stepwise fashion with pauses at each position (figure 1), so the entire thrombus throughout the TS could be retrieved. While this process took nearly 20 min, it also enabled recanalization of the entire sinus with a single deployment of the device and was thus a relatively efficient means of achieving the desired result. This stepwise withdrawal technique may be useful for larger clot burdens.
Mechanical thrombectomy has been proposed as a first-line treatment for cerebral venous sinus thrombosis.5 However, there are currently no data from controlled trials to support this practice, although a clinical trial is now recruiting.8 Most cases will improve with anticoagulation without the need for more aggressive treatment,1 and endovascular therapy should only be considered in those patients with further deterioration and/or at risk for poor prognosis.9 This case demonstrates that, when endovascular therapy is undertaken, the Solitaire FR device provides a new treatment option for cerebral venous sinus thrombosis.
Key messages
-
Endovascular treatment for cerebral venous sinus thrombosis should be considered in the setting of clinical deterioration despite appropriate anticoagulation.
-
The Solitaire FR device can be used effectively for cerebral venous sinus thrombectomy.
-
The larger 6 mm Solitaire device is probably more appropriate for venous thrombectomy than the smaller 4 mm device.
-
Stepwise withdrawal of the device through a long occlusion can achieve recanalization in a single pass.
Footnotes
-
Correction notice This article has been corrected since it was published Online First. The footer did not contain the correct j-title of J NeuroIntervent Surg. This has now been corrected.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.