Article Text

Abstract
Background Spinal epidural arteriovenous fistulas (SEDAVF) are rare and poorly understood clinical entities.
Materials and methods We report a series of five (three men, two women) consecutive cases treated at our center to analyze their characteristic and treatment strategies in their management. We report a successful technique of percutaneous embolization of fistulas in a patient with failed previous attempts.
Results All five patients were symptomatic; three patients presented with a history of back pain, which progressed to myelopathic symptoms, one patient had symptoms of persistent back pain, and one patient had intermittent numbness of the left arm and thigh. Of the three patients who had myelopathic symptoms, two were successfully treated with transarterial embolizations with Onyx copolymer. The third patient who had a prominent epidural venous pouch with numerous arterial feeders was embolized percutaneously with a flat detector CT guided navigation (XperCT) and real time fluoroscopic monitoring of the injected n-butyl cyanoacrylate glue, after previous unsuccessful attempts with surgery and arterial embolizations. All three myelopathic treated patients had complete angiographic remission of the fistulas and symptoms on follow-up (mean 7.2 months).
Conclusions The diagnosis and treatment of SEDAVF can be challenging due to their rarity and intricate pathomechanics. Patients with severe pain or progression of symptoms or myelopathic symptoms need to be treated at the earliest opportunity, while asymptomatic patients can be closely monitored. Percutaneous embolization is an effective strategy to embolize SEDAVF associated venous pouch.
- Arteriovenous Malformation
- Spinal cord
- Liquid Embolic Material
- Fistula
- Angiography
Statistics from Altmetric.com
Introduction
Arteriovenous fistulas (AVF) are the most frequent vascular malformations in the spinal cord, commonly occurring in men in the thoracolumbar region. The fistulous connections of spinal AVF are typically located in the duramater (between the radiculomeningeal artery and the radicular vein as it exits the dural sleeve) or within the spinal cord parenchyma.1 In very rare instances, the fistula occurs extradurally between branches of the radicular artery and the epidural venous plexus, referred to as the spinal epidural or extradural arteriovenous fistula (SEDAVF).
Spinal epidural AVF are rarely symptomatic but may present with symptoms due to a compressive mass effect on adjacent nerve roots or from congestive myelopathy. Very few case reports in the literature have described spinal epidural AVF2–10 and a detailed analysis of their clinical presentation, diagnosis, and management is warranted. We describe five consecutive spinal epidural AVF managed at our center, and analyze their angioarchitechture, pathophysiology, and treatment strategies. We also present a new technique of percutaneous fistula embolization using flat detector CT guided navigation.
Case series
Patient No 1
A 65-year-old patient presented with difficulty walking and episodes of bilateral leg weakness and bowel incontinence. Subsequent MR imaging showed a poorly circumscribed hyperintense lesion of the spinal cord in the lumbar (L3) region, diffuse cord edema, and multiple dorsal flow voids (figure 1A). Spinal angiography revealed an epidural AVF with a single arterial feeder (the right lumbar L3 segmental artery communicating to an epidural vein, which in turn anastomosed with perimedullary veins at the level of T12) (figure 1B). The feeding branch was selectively catheterized (figure 1C) and embolized with 1 ml of Onyx copolymer (eV3 Neurovascular, Irvine, California, USA). Post embolization runs confirmed complete obliteration of the fistula (figure 1D). His symptoms improved, and at the 6 month follow-up, he was completely asymptomatic with a normal neurological examination. Subsequent spinal angiography confirmed the absence of any residual fistula.
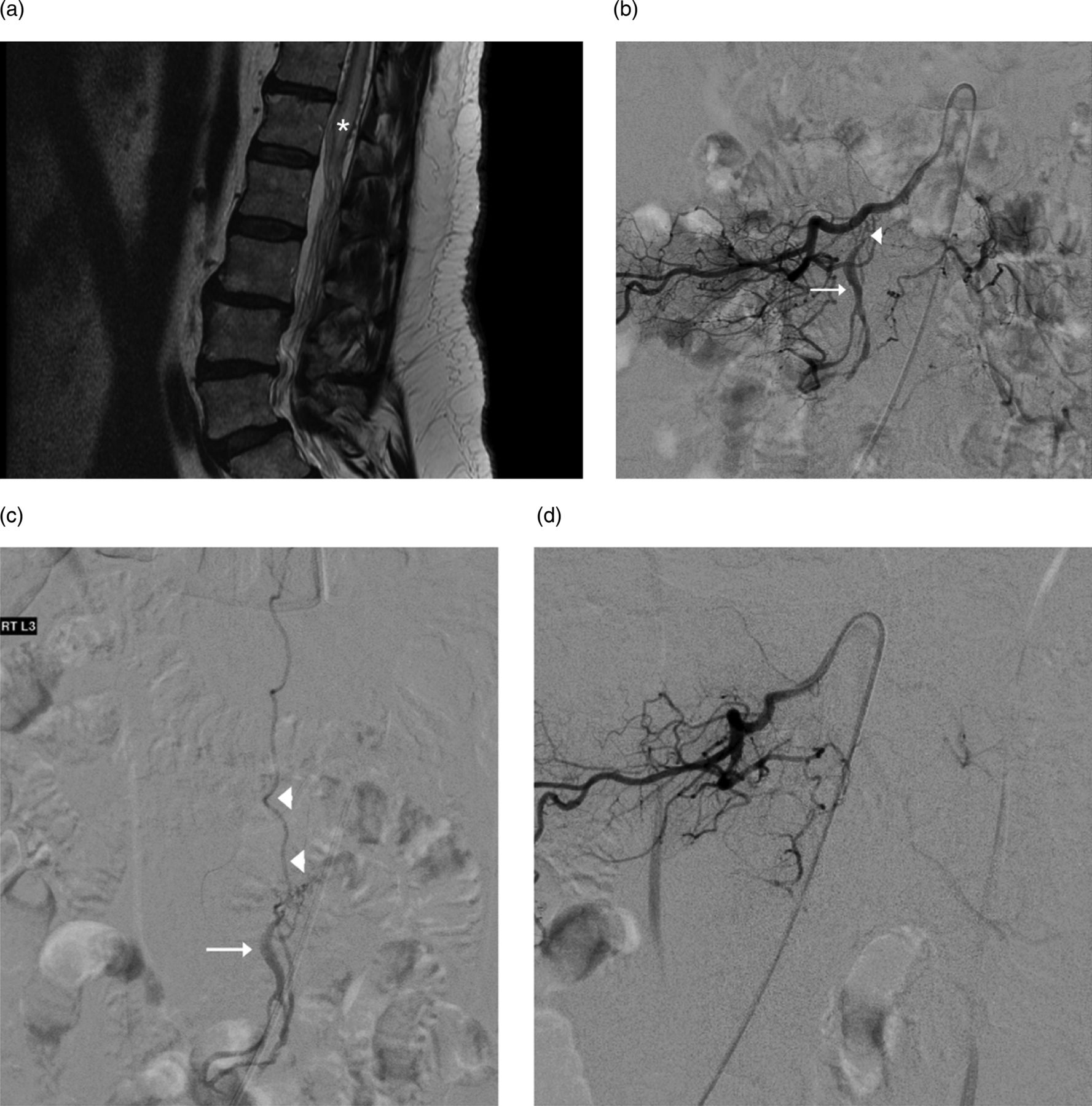
Pre and post embolization images of L3 level spinal epidural arteriovenous fistulas. (A) T2 weighted sagittal MRI of the lumbar spine shows congestive edema of the conus medullaris (asterisk) with abnormal perimedullary flow voids. (B) Spinal angiography showing a fistulous connection (arrowhead) between the right L3 segmental artery and epidural venous pouch (arrow). (C) Superselective spinal angiogram demonstrating an epidural fistulous pouch (arrow) with ascending perimedullary drainage (arrowheads). (D) Spinal angiography status post Onyx embolization of an epidural fistulous pouch. No residual fistula is seen.
Patient No 2
A 59-year-old patient presented with a 2 month history of progressive bilateral foot numbness and weakness with sudden worsening, urinary incontinence, and pain in right lower extremity. Spinal MR imaging revealed a hyperintensity in the dorsal spinal cord extending from T11 to the conus and an associated prominent vessel (figure 2A). Spinal angiography showed numerous anomalous arteriovenous connections from (left) segmental arteries at L1 and L2 to an epidural venous pouch (figure 2B). Despite multiple transarterial embolizations of the arterial feeders with Onyx, the fistula persisted. The patient was referred for laminectomy and surgical obliteration of two additional arterial feeders found in post embolization angiograms. In addition, fibrin glue was injected directly into one of the involved epidural veins. The patient was discharged home with initial neurological improvement but returned to clinic several months later with symptom recurrence. Repeat spinal angiography revealed arterial feeders from right L1 to L2 segmental arteries (not visualized before), and the L1 feeder was successfully embolized with Onyx (figure 2C). The fistula persisted on injection of L2 segmental artery, without obvious feeding vessels. Direct percutaneous embolization of the fistulous pouch was proposed.

Pre and post percutaneous embolization images of persistent lumbar spinal epidural arteriovenous fistulas (patient No 4). (A) Coronal contrast enhanced MR angiography of the thoracic spine demonstrating a large perimedullary draining vein (arrow). (B) Spinal angiography of the left L2 segmental artery feeding the epidural fistulous pouch (arrow). Faint arterial feeders from incomplete contrast reflux into the left L1 segmental artery are also seen (arrowhead). (C) Repeat spinal angiography after previous embolization of the left L1–L2 feeders and surgical disconnection of the fistula demonstrates a persistent fistulous pouch (arrow) fed by branches of the right L1 segmental artery (arrowhead). (D) Flat detector CT (XperCT) of the lumbar spine during percutaneous embolization. Note the hyperdense previous embolization material (arrowheads) and the fluoroscopically guided needle (arrows). (E) Percutaneous embolization of a residual fistula (arrow). CT guided embolization of the fistula was performed with n-butyl cyanoacrylate glue injection.
With the patient positioned prone on the angiogram table, diluted iodinated contrast was intravenously infused, after which a flat detector CT was obtained (XperCT, Philips Inc, Best, The Netherlands) (figure 2D). The enhancing fistulous pouch was identified, and targeting software was used to define a percutaneous trajectory for direct embolization (XperGuide; Philips Inc). Embolization was performed with n-butyl cyanoacrylate glue (Trufill; Cordis Neurovascular Inc, Miami Lakes, Florida, USA) and ethiodol under careful fluoroscopic monitoring with CT overlay to prevent unintended extravasations into the intramedullary compartment (figure 2E). Completion angiography runs confirmed complete embolization of the fistula. On 1 month follow-up, the patient's symptoms had improved, and spinal angiography confirmed complete obliteration of the fistula.
Patient No 3
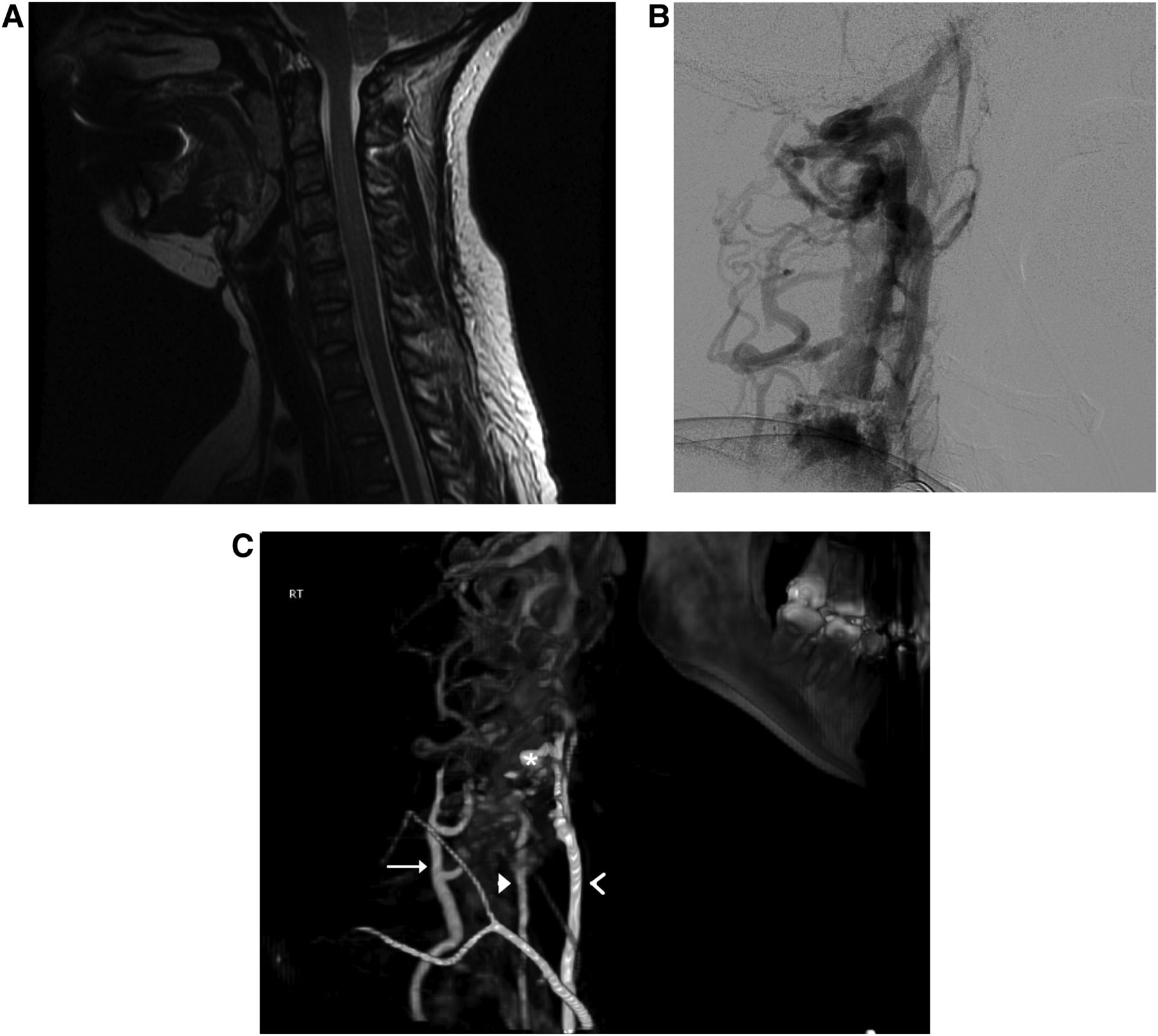
A 46-year-old patient with a previous history of lumbar laminectomy presented with a 4 month history of intermittent upper back pain and bilateral lower extremity weakness. Spinal MR imaging (figure 3A) and CT angiography revealed a large mass lesion in the upper thoracic epidural space (a hemangioma), as well as an arteriovenous malformation in the left shoulder region. Spinal angiography confirmed an epidural AVF, with arterial feeder arising from the C7 muscular branch of the left deep cervical artery communicating to a large venous pouch (figure 3B). Transarterial embolization with Onyx was performed resulting in complete obliterate of the fistula (figure 3C). At the 4 month follow-up, angiography confirmed absence of any residual fistula (not shown).

Pre and post embolization images of the cervical spinal epidural arteriovenous fistulas. (A) Sagittal T1 MRI of the chest, demonstrating vascular flow voids in the epidural space (arrow), above an ill defined epidural mass in the upper thoracic spine (asterisk), consistent with hemangioma. Vascular flow voids from a muscular arteriovenous malformation are also seen (arrowhead). (B) Angiography of the deep cervical artery demonstrates a complex epidural fistula (arrow) with enlarged posterior perimedullary drainage (arrowheads). (C) Angiography after embolization demonstrates complete obliteration of the fistula.
Patient No 4
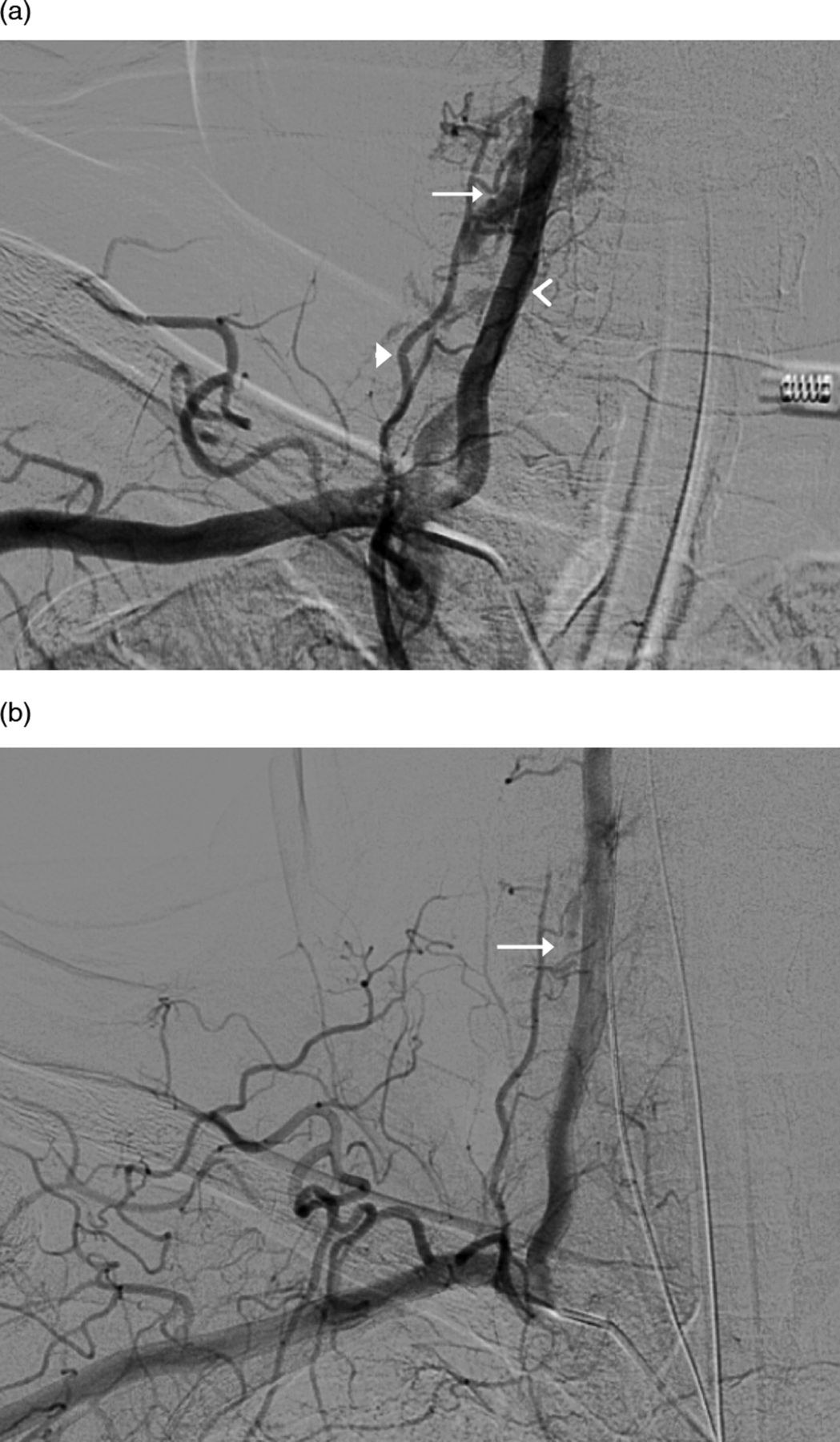
A 58-year-old patient presented with a 2 year history of intermittent pain at the back of the neck that radiated down to the shoulder blade and the upper back. An MRI of the shoulder was performed and the patient underwent shoulder surgery for findings of rotatator cuff injury. The patient underwent repeat shoulder surgery for lack of symptom relief following the first surgery. As the initial symptoms were not relieved, MR imaging of the spine was performed, which showed poorly circumscribed foci of enhancements in the C5–C6 foraminal region and paravertebral soft tissue associated with cord compression at the C6–C7 region. Spinal angiography showed an epidural AVF supplied predominantly by the right vertebral artery, and the ascending branches of the thyrocervical trunk, with drainage into a venous pouch in the epidural space adjacent to the C5–C6 neural foramen (figure 4A). As there were numerous arterial feeders and a prominent venous pouch, venous embolization via percutaneous access was planned. However, 8 weeks later, prior to performing the procedure, the angiogram showed significant reduction in the size of the venous pouch (figure 4B). No intervention was performed given the natural regression of the fistula. On continued follow-up, the patient had complete resolution of symptoms.

Images of the spinal epidural arteriovenous fistulas (patient No 4). (A) Left subclavian angiography, anteroposterior projection, demonstrates an epidural fistulous pouch (arrow) supplied by branches of the vertebral artery (open arrowhead) and ascending cervical branch of the thyrocervical trunk (closed arrowhead). (B) Follow-up subclavian angiography 8 weeks after presentation. Significant reduction in the size of the fistulous pouch (arrow) and number of feeding arteries is noted.
Patient No 5
A 28-year-old patient presented with intermittent balance difficulties and numbness of the left shoulder and left upper thigh. An MRI showed no cord edema or evidence of venous congestion. Spinal angiography demonstrated a complex right-sided C5 epidural AVF with primary feeders from the ascending cervical branches of the thyrocervical trunk, and deep muscle branches from the subclavian, vertebral, and inferior thyroid arteries (figure 5B), and the anatomic relationship to the cervical spine was visualized with a 3DRA-XperCT reconstructed CT angiogram (figure 5C). Venous drainage was into a large venous pouch varix that fed into the epidural venous plexus, which further drained into a tributary to the ipsilateral internal jugular vein and across the epidural space to the contralateral internal jugular vein. The patient also underwent MR imaging of the brain that showed two small cavernous malformations in the left cerebellum and the left posterior occipital region. As the presenting symptoms in this patient could not be entirely ascribed to epidural AVF (with no evidence of cord edema in MRI), close clinical monitoring and intermittent angiographic follow-up were planned, considering the possibility of spontaneous regression of the AVF.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Imaging characteristics of the cervical epidural fistulas (patient No 5). (A) T2 weighted MRI of the cervical spine shows no evidence of spinal cord edema or venous congestion to explain the patient's neurological complaints. (B) Subclavian angiography, lateral projection, demonstrates the complex epidural arteriovenous fistulas supplied by branches of the thyrocervical trunk, vertebral, and inferior thyroid arteries. (C) Combined three-dimensional rotational angiography and XperCT of the cervical spine with injection of the right subclavian artery. The fistula (asterisk) is seen at C5–6 with feeders from the ascending cervical (arrow), vertebral (closed arrowhead), and inferior thyroid (open arrowhead) arteries.
Discussion
Pathophysiology
The symptomatology and structural alterations in epidural fistulas are largely different from those of spinal dural AVF. The epidural venous plexus is a system of vertically continuous, thin walled valveless veins located in the epidural space intermixed with fat and fibrous tissue. They drain the intradural veins and flow towards the azygous and hemiazygous venous system. Abnormal communication between one or more segmental radicular arteries and the veins leads to epidural AVF, whereas abnormal communication between one or more radiculomeningeal arteries and intradural/radicular veins leads to the more common spinal dural AVF. Unlike dural AVF, the epidurals are generally occult and asymptomatic.11 When there is considerable increase in size due to arterializations of the veins, patients may present with compressive symptoms of the expanding varix on adjacent nerve roots.12 Uncommonly, symptoms can occur due to intradural or perimedullary reflux induced cord myelopathy. In general, the epidural fistulas do not develop retrograde flow into the perimedullary venous system, which is thought to be due to resistance from sharp angulations of veins leaving the intraspinal compartment to form tortuous narrow glomeruli-like structures between the two dural layers.13 ,14 It is thought that perimedullary venous drainage develops in rare occasions when the protective mechanisms preventing reflux from the epidural veins fails, which then leads to venous outflow obstruction, secondary ischemia, and myelopathy.4 ,8 ,15
In our series of five patients, three patients presented with myelopathy and had perimedullary venous drainage. The other two patients had epidural venous drainage patterns, of which one presented with back pain (and spontaneously thrombosed during follow-up), while the other was asymptomatic. All three myelopathic patients initially developed symptoms of nerve root compression which later progressed to myelopathic symptoms, similar to other reported cases.8 ,16 This pattern of neurological progression suggests that chronic arteriovenous shunting leads to failure of the natural mechanisms protecting retrograde reflux into perimedullary veins. Other mechanisms such as medullary blood flow steal phenomenon and intraspinal hemorrhage have also been proposed as possible mechanisms for symptoms.17
Treatment
Any progressively enlarging or symptomatic fistula needs to be treated at the earliest opportunity to prevent possible development of perimedullary venous drainage or cord edema. Asymptomatic patients can be treated or closely monitored given the possibility of spontaneous thrombosis of the draining veins and regression of the fistula. Complete treatment of epidural AVF with surgery, transarterial or transvenous embolizations, or in combination has been reported.9 ,15 The treatment strategy is similar to spinal dural AVF: occlude the shunt and proximal venous communication while keeping the distal portion of the vein and proximal artery intact. In general, transarterial embolization of the feeding vessel is a less invasive and effective method to obliterate the fistula when a single arterial feeder is present. Surgical treatment is preferred when the fistula is close to the anterior spinal artery13 or in the setting of multiple arterial feeders to a high flow fistula, which can make arterial embolizations more difficult.
Unlike in spinal dural AVF, the draining veins of epidural AVF are located in the azygous venous system. These veins contain valves as well as numerous metameric connections in paraspinal longitudinal veins.3 These features make transvenous embolization technically difficult and often times anatomically impossible. Nevertheless, successful fistula obliteration via transvenous embolization with glue and coils have been reported, and is considered to be a more effective treatment, especially when multiple arterial feeders are present.7 ,8 We report a successful new technique of direct percutaneous embolization of a epidural venous pouch with n-butyl cyanoacrylate glue in one such patient (patient No 2) with multiple arterial feeders, who was refractory to several transarterial embolizations and surgery. This percutaneous technique has the advantage of providing a relatively easy access to the venous system compared with the conventional transvenous route, especially when a large venous pouch is present. It can be considered as a convenient firstline treatment of epidural fistulas.
Conclusion
The diagnosis and treatment of spinal epidural AVF can be challenging given their rare occurrence and intricate pathomechanics. Prompt diagnosis and treatment of all symptomatic epidural AVF is necessary to prevent potential progression to perimedullary drainage or to possibly reverse myelopathy when present. Embolization of the venous system when possible is a definitive strategy to obliterate the fistula. We have demonstrated a new percutaneous CT guided interventional technique to directly access the venous pouch and embolize the venous system in a case of refractory epridural AVF with multiple arterial feeders. Detailed knowledge of the spinal vasculature, anatomy of feeding vessels, and the venous drainage pattern is necessary to determine the appropriate treatment modality.
References
Footnotes
-
Contributors Conception and design: DR and BVG. Acquisition of the data: all authors. Analysis and interpretation of the data: all authors. Drafting the article: DR, MRL and BVG. Critically revising the article: all authors. Reviewed final version of the manuscript and approved it for submission: all authors. Study supervision: BVG.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.