Article Text

Abstract
Background Recent reports suggest that placement of a venous sinus stent improves symptoms in selected patients with idiopathic intracranial hypertension (IIH). We report our evaluation of the long-term patency of venous stents placed for IIH.
Methods We retrospectively reviewed our clinical database for 30 patients (mean age 33±10 years) with IIH who underwent placement of 36 venous sinus stents between October 2006 and December 2012. Relevant clinical, demographic and radiographic data were extracted after review of these records. All patients underwent retrograde venography to confirm a >50% stenosis and a trans-stenosis pressure gradient. Follow-up catheter angiography was performed beginning 3 months after the procedure.
Results Follow-up imaging was available for 23 (77%) of the 30 patients (mean 23 months). For seven patients, angiographic follow-up of >2 years (mean 45 months) was available. All stents remained patent with mild (<25%) in-stent stenosis observed in four patients. In five patients, however, we observed a narrowing of the sinus proximal to the stent. Although no patient underwent repeat stent placement for persistent or recurrent symptoms, cerebrospinal fluid diversion was performed in five cases.
Conclusions Venous sinus stent placement has emerged as a promising treatment option for the subgroup of patients with IIH with a pressure gradient across a stenotic venous sinus. We observed long-term patency of all stents placed in this patient population. Further prospective investigation is necessary to improve our understanding of the phenomenon of sinus narrowing upstream of a patent stent and to establish definitively the long-term clinical efficacy of venous sinus stent placement for IIH.
- Intervention
- Intracranial Pressure
- Stenosis
- Stent
- Vein
Statistics from Altmetric.com
Introduction
Idiopathic intracranial hypertension (IIH), also known as pseudotumor cerebri, is a neurological disorder characterized by increased intracranial pressure (ICP) in the absence of imaging evidence of primary cerebral disease. This condition occurs most commonly in young obese women and presents with chronic headache and papilledema. In severe cases, transmission of elevated pressure to the optic nerve and disk may result in visual loss. First-line treatment for IIH involves medication and weight loss counseling. Pharmacologic treatment with the carbonic anhydrase inhibitor acetazolamide can be very effective in reducing cerebrospinal fluid (CSF) production, thus reducing ICP and ameliorating symptoms.1
In patients whose symptoms are refractory to conservative management, CSF diversion is typically performed to arrest progression of visual loss. While these techniques are extremely effective in reducing ICP, they are associated with an increased risk of complications.2 For example, patients with IIH often have slit ventricles which can contribute to difficulty in ventricular catheter placement and to subsequent shunt malfunction. The alternative treatment of optic nerve sheath fenestration has also been used to alleviate pressure on the optic nerve in patients with papilledema and progressive visual loss. This procedure is performed by an ophthalmologist and involves longitudinal parallel incisions along the nerve sheath, resulting in an egress of CSF and reduction of pressure. Many authors have noted sustained visual improvement following nerve sheath fenestration.3 However, patients often experience recurrent visual symptoms even after successful fenestration.4
Venous sinus stenosis has been demonstrated in a significant proportion of patients with IIH and is thought to play a role in the disease pathogenesis.5–11 It remains unclear whether this stenosis directly leads to increased ICP or whether primarily elevated ICP produces an extrinsic compression of the venous sinuses.12 Multiple recent series have demonstrated that expansion of a stenotic sinus segment by placement of a stent leads to normalization of the venous pressure gradient and a reduction of CSF pressure.13–16 However, long-term follow-up data to support stent patency are limited. We therefore evaluated our series of patients with IIH treated by venous sinus stent placement to assess the rate of long-term stent patency.
Methods
We retrospectively reviewed our prospectively-maintained clinical database for a total of 30 patients with the diagnosis of IIH who underwent placement of a venous sinus stent between October 2006 and December 2012 at Barrow Neurological Institute and St Joseph's Hospital and Medical Center in Phoenix, Arizona, USA. Relevant clinical, demographic and radiographic data were extracted following review of outpatient clinic and inpatient hospital medical records, operative notesand cerebral angiograms.
Patient cohort
This series included 25 women (83%) and 5 men of mean age 33±10 years (range 14–52). All patients had a clinical diagnosis of IIH with headaches, papilledema and elevated ICP, together with non-invasive imaging evidence suggesting significant venous sinus stenosis. All patients underwent retrograde venography to confirm stenosis of >50% as well as a pressure gradient of >10 mm Hg across the stenotic sinus segment. The extent of venous sinus stenosis was assessed by first subtracting the diameter of the contrast filling channel from the maximal diameter of the adjacent sinus in the B plane. The percentage stenosis was then calculated by dividing this difference by the maximal diameter of the adjacent sinus. Similarly, the extent of in-stent stenosis was determined by subtracting the diameter of the contrast opacified channel from the diameter of the fully expanded stent in the B plane. The percentage of in-stent stenosis was then calculated by dividing this difference by the diameter of the stent. Stenosis was graded as mild (<25%), moderate (26–75%) or severe (>75%).
Venous sinus stent placement and follow-up
The endovascular techniques used for placement of venous sinus stents have been previously described in detail.17 A total of 36 stents were placed in 30 patients. Dual antiplatelet medication with acetylsalicylic acid 325 mg and clopidogrel 75 mg daily was initiated 3 days prior to treatment. Both agents were continued until 3 months after placement, at which point clopidogrel was discontinued. Follow-up imaging for all patients by arteriography or retrograde venography to assess for continued stent patency was performed beginning a minimum of 3 months following the initial procedure. Symptomatic improvement was determined based on each patient's subjective report of headache symptoms as recorded in the medical record.
Results
Radiographic outcome
Follow-up imaging was available for 23 of the 30 patients (77%) with a mean follow-up period of 22 months (figure 1). For seven of these patients, angiographic follow-up for >2 years (mean 45 months) was available. All stents remained patent, with in-stent stenosis observed in four patients (figure 2). Two of these stenoses were graded as mild and two were graded as moderate (table 1). None of these stenoses produced any significant flow limitation. Additionally, in five patients we observed significant narrowing immediately upstream of the previously placed stent (figure 3). In all of these cases robust flow was observed from the vein of Labbe across the wall of the stent with patent anterograde distal outflow through the sigmoid sinus.
Patient characteristics
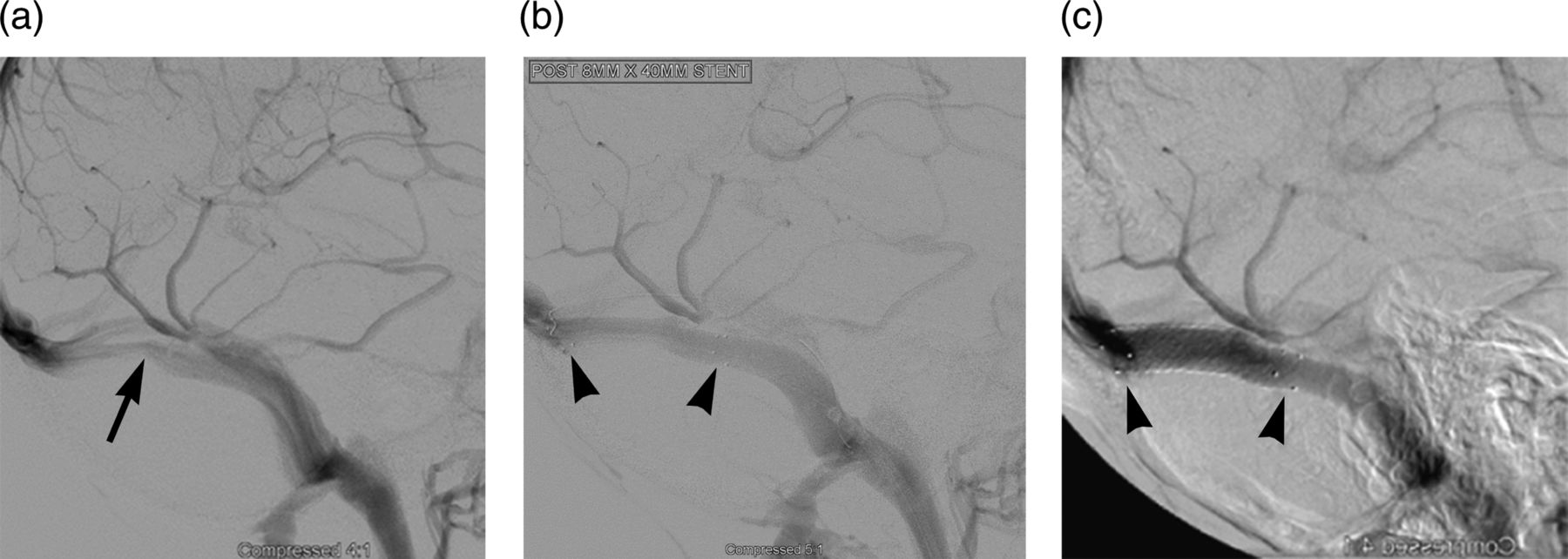
(A) Representative lateral projection of the venous phase of a right internal carotid artery arteriogram of an obese woman with diagnosis of idiopathic intracranial hypertension (IIH). A venous pressure gradient of 26 mm Hg was noted across the right transverse sigmoid junction with a measured stenosis (arrow) of 60%. A Zilver stent (Cook Medical, Bloomington, IN) was placed across the right transverse sigmoid junction, resulting in improvement in blood flow (B) and immediate resolution of the venous pressure gradient. The proximal and distal stent tines are shown by arrowheads. The stent (arrowheads) remains patent at 18 months (C), without evidence of in-stent stenosis. Reproduced with permission from Barrow Neurological Institute.

Non-flow limiting in-stent restenosis (arrow) observed on 6 month follow-up imaging. Reproduced with permission from Barrow Neurological Institute.

{kind=link}
{kind=link}
{kind=link}
A 36 year-old patient with a right transverse sigmoid stenosis (arrow) who underwent placement of a venous sinus stent (A, lateral projection). Following stent placement the patient exhibited improvement in this stenosis accompanied by immediate symptomatic relief (B, lateral projection). (C) Follow-up lateral projection of the venous phase of a follow-up angiogram 6 months after treatment demonstrates a narrowing (arrow) of the left transverse sinus proximal to the stent. The vein of Labbe (asterisk) drains through the stent, as demonstrated in the lateral projection. Reproduced with permission from Barrow Neurological Institute.
Clinical outcome
Long-term clinical follow-up was available for 27 of the 30 patients (90%). Of these patients, 19 (70%) exhibited symptomatic improvement, with the remaining patients showing either persistent symptoms or symptom recurrence following a transient improvement (table 1). No patient underwent placement of an additional stent for persistent or recurrent symptoms. However, five patients underwent subsequent placement of a lumboperitoneal (n=1) or ventriculoperitoneal (n=4) shunt for persistent or recurrent symptoms despite successful placement of a venous sinus stent. Shunt placement occurred at a mean of 1.6 months following the initial stent procedure.
Complications
One patient (3%) developed a right common femoral artery pseudoaneurysm that was treated by placement of a femoral artery stent. Otherwise, there were no permanent complications attributed to venous sinus stent placement.
Discussion
Although a large proportion of patients with IIH exhibit stenosis of one or both dural venous sinuses, generally at the level of the transverse/sigmoid junction, the role that such stenoses play in the development of elevated ICP remains unclear.13 One possibility is that increased venous pressures proximal to a stenosis may impede resorption of CSF at the level of the arachnoid granulations, thus primarily increasing ICP. Alternatively, it has been proposed that such venous sinus stenoses may in fact develop secondary to extrinsic compression by elevated ICP and might then exacerbate the ICP in a feedback-type loop.13 Placement of a venous sinus stent may break such a feedback loop by preventing collapse of a compressible venous sinus in the face of elevated ICP. Regardless of the mechanism of elevated ICP, venous sinus stent placement can result in rapid improvement in symptoms as well as normalization of CSF pressure.13 ,14
A number of reports have described the use of venous sinus stents in the treatment of IIH, but long-term radiographic follow-up is lacking. The largest reported series by Ahmed et al included 52 patients with medically refractory IIH who underwent stenting of a transverse sinus.13 Stent placement immediately eliminated the venous pressure gradient and led to an improvement in symptoms. In six of these patients, clinical relapse was associated with increased venous pressure and stenosis adjacent to the previous stent. Placement of an additional stent led to symptomatic improvement. Overall, the authors reported that 49 of 52 patients were cured of their symptoms. Unfortunately, follow-up angiography/venography was not performed in cases without recurrent symptoms.
Ahmed et al have recently published an update to this series which included an additional 18 cases.15 In total, seven of the 70 patients (10%) required a second stent placement secondary to clinical and hemodynamic deterioration associated with the development of a stenosis proximal to the stent. The authors report two cases of significant neurological complications, including one case of subdural hematoma secondary to a vein perforation and another case of multicompartmental hemorrhage, both treated by immediate craniotomy with full neurological recovery.
Another large series by Kumpe et al14 evaluated 18 patients who underwent placement of 19 venous sinus stents. Follow-up arteriograms were performed in 16 patients at a mean of 25.3 months and revealed patency of all stents without evidence of recurrent stenosis. These authors also noted either a stenosis or filling defect of the transverse sinus adjacent to the stents in four patients (22%). Three of these four patients developed hemodynamic deterioration and one underwent repeat stent placement. Additionally, one major complication was noted involving a patient who developed a subdural and subarachnoid hemorrhage managed by ventriculostomy with spontaneous hematoma resolution.
The most recent series describes a retrospective series of 15 patients who underwent venous sinus stent placement for IIH.16 The authors achieved technical success in all patients without major complication. Of these patients, 10 demonstrated improvement in headaches, and papilledema resolved in all patients. In two cases, persistent headaches prompted subsequent placement of a ventriculoperitoneal shunt. Angiographic follow-up was available in 14 patients at a mean of 9 months. They observed no instances of in-stent or adjacent restenosis. The reasons for this complete lack of stenosis compared with prior reports remain unclear. Although the overall follow-up imaging interval was 9 months, for those patients examined by angiography the mean follow-up interval was only 6 months. A longer follow-up interval would reveal additional stenoses. Furthermore, unlike previous series, these authors performed balloon angioplasty prior to stent placement. It is possible that this procedure serves to mimimize subsequent stenosis.
Our 100% long-term patency rate supports the findings of these earlier series. We noted only four cases (17%) of mild (<25%) in-stent stenosis without flow limitation (figure 2). It appears that in-stent stenosis of venous sinus stents occurs less frequently than in intracranial arterial stents where in-stent restenosis rates may approach 30%.18–20 This probably relates to differences in the size and radial force of these stents, as well as differences in flow dynamics in the venous sinuses. In both of our series as well as in previously published series dual antiplatelet treatment with acetylsalicylic acid and clopidogrel was initiated for a minimum of 3 days prior to the procedure, and these agents were maintained for a minimum of 3 months after treatment.
Interestingly, five of our patients developed a narrowing of the ipsilateral transverse sinus proximal to the stent (22%), similar to the phenomenon described in prior series.14 ,15 In each of these cases the vein of Labbe was observed draining the ipsilateral temporal lobe through the stent, with anterograde drainage through the ipsilateral sigmoid sinus. Additionally, the predominant venous drainage proceeded through the contralateral transverse and sigmoid sinus in these patients. Contrary to prior series, in our patients this phenomenon was not often associated with symptom recurrence. In fact, only one of these five patients exhibited persistent symptoms that required placement of a ventriculoperitoneal shunt, and no patient underwent repeat or additional stent placement. The etiology of this proximal stenosis remains unclear. In cases with recurrent symptoms it is possible that increased ICP results in extrinsic compression of the sinus segment lacking the outward radial force of the stent. Alternatively, in asymptomatic cases with predominant flow through a contralateral transverse/sigmoid sinus, the ipsilateral proximal sinus may simply atrophy if it is not required for venous drainage. Finally, it is possible that the proximal narrowing represents a venopathic process. For instance, in dural arteriovenous fistulas as well as in arteriovenous fistulas created in patients on dialysis, chronically increased venous outflow frequently results in progressive venous stenosis.21–23 Following stent placement in a stenotic sinus, the increased flow through the stented segment may ultimately produce a narrowing of the segment proximal to the stent. Further work is necessary to determine both the etiology and clinical relevance of the proximal narrowing observed in our series as well as in prior series.
The present study is limited by a lack of objective measures of efficacy. For instance, lumbar puncture opening pressures both before and after stent placement could more objectively determine whether expansion of the stenotic sinus improves ICP. Additional information could be gained by rigorous assessment of venous pressures following stent deployment as well as on follow-up venography, particularly in the setting of a proximal stenosis. Furthermore, formal documentation of visual acuity and papilledema before and after stent placement and on follow-up examination would more convincingly establish the long-term efficacy of venous sinus stent placement in the setting of medically refractory IIH.
Venous sinus stent placement has recently emerged as a promising treatment option for the specific subgroup of patients who have a venous pressure gradient across a stenotic venous sinus. A significant proportion of patients treated in this manner demonstrate clinical improvement, and these stents exhibit exceptional rates of angiographic long-term patency. Further investigation is necessary to improve our understanding of the phenomenon of sinus stenosis adjacent to a patent stent. Additionally, a larger prospective study is warranted to definitively establish the long-term clinical efficacy of venous sinus stent placement for patients with IIH.
References
Footnotes
-
Contributors All authors made substantive intellectual contributions to this study.
-
Competing interests None.
-
Ethics approval This study was approved by the Institutional Review Board at St Joseph's Hospital and Medical Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.