Article Text

Abstract
Purpose Thrombus length has been shown to be an important determinant of recanalization using intravenous thrombolysis in hyperacute ischemic stroke. Various studies have attempted to quantify thrombus based on non-contrast CT (NCCT) or CT angiography (CTA). However, thrombus may not be seen on NCCT, and CTA may fail to delineate the distal extent of the thrombus. Contrast enhanced CT (CECT) following CTA can be used to estimate infarct core, but we investigated whether the angiographic data available on these images provided reliable information on thrombus length.
Materials and methods 15 consecutive patients, mean age 81 years (range 63–93), with terminal internal carotid artery or M1-middle cerebral artery occlusions underwent NCCT, CTA (bolus tracked technique), and CECT (acquired 80 s post initial CTA injection). Three radiologists assessed thrombus length on thin slice NCCT, and CTA and CECT.
Results CTA overestimated thrombus length relative to NCCT (p<0.001) and CECT (p<0.001). There was less difference between CTA and CECT estimation in patients with good collateral scores (p<0.05). There was good correlation between NCCT and CECT (Pearson's correlation coefficient=0.90, 95% CI 0.81 to 0.95, p<0.001). Inter-rater reliability assessed using intraclass correlation was 0.95 (95% CI 0.87 to 0.98) for NCCT and 0.98 (95% CI 0.94 to 0.99) for CECT.
Conclusions CTA regularly overestimates thrombus length as the distal end of the thrombus is not delineated. This can be overcome through the use of a CECT acquisition which can reliably be used to estimate thrombus length.
- CT Angiography
- Stroke
- Artery
- CT
- Thrombolysis
Statistics from Altmetric.com
Introduction
Thrombus length has recently been shown to be an important determinant of vessel recanalization using intravenous recombinant tissue plasminogen activator (IV rtPA).1 ,2 Reidel and colleagues1 ,2 demonstrated that thrombus length of >8 mm, assessed using thin slice non-contrast CT (NCCT), was associated with <1% chance of recanalization with IV rtPA. Thrombus length estimation is now being included in trial design for the assessment of the efficacy of mechanical thrombectomy.3.
A hyperdense vessel may only be present in approximately 30–50% of acute middle cerebral artery (MCA) occlusions using standard 3 mm NCCT slice thicknesses.4 ,5 Scrutiny of thin slice (<2.5 mm) NCCT may increase sensitivity for thrombus detection and also the accuracy of thrombus length measurement as partial volume effects are reduced.1 However, more than 10% of patients still show absence of dense thrombus, despite the use of thin slice reconstructions.2 The presence of hyperdense thrombus on NCCT is dependent on thrombus constituents, tending to occur in red blood cell predominant thrombi and not in fibrin predominant thrombi.4 Furthermore, calcified arterial walls and elevated hematocrit could cause vascular hyperdensities that mimic thrombus. An alternative means of estimating thrombus length, independent of thrombus density, would therefore be useful.
For identification or confirmation of arterial occlusion, CT angiography (CTA) has been developed as a useful tool in the acute stroke setting.6 While it has been demonstrated that quantification of intracranial thrombus extent using CTA predicts functional outcome, final infarct size, and parenchymal hematoma formation,7 a recent study failed to demonstrate a relationship between thrombus length measured on fast acquisition CTA maximum intensity projection (MIP) images with ability of IV rtPA to recanalize.8 We hypothesize, as have others,9 that this is due to failure of early arterial CTA to clearly delineate the distal extent of the thrombus and that early arterial CTA is not a reliable tool in thrombus length estimation. Retrograde flow of contrast via collateral pathways to the distal end of the thrombus is necessary in order to accurately assess length of thrombus. Retrograde flow will be dependent on the patency of pial collaterals and therefore early arterial imaging may well overestimate thrombus length, especially when collateral flow is poor.
At our institution, we use both an early arterial fast acquisition CTA and a delayed phase contrast enhanced CT (CECT) acquisition as part of our acute ischemic stroke protocol in order to optimize vascular and parenchymal imaging; the former providing optimal arterial imaging with minimal venous contamination, the latter used predominantly for assessment of core infarct.10–13
Through post processing the delayed phase CECT acquisition to obtain angiographic data, we aim to demonstrate that large differences in vascular non-opacification, and hence thrombus length estimation, can be obtained using early and delayed phase post contrast imaging. As a result, we aim to prove that length estimation using fast acquisition CTA is not reliable and is dependent on collateral flow. Furthermore, we highlight the assessment of delayed phase CECT images as a potentially useful tool for rapid thrombus length estimation through comparison with thin slice NCCT as the gold standard.
Methods
Fifteen consecutive patients with acute ischemic stroke secondary to terminal internal carotid artery (TICA) or M1-MCA occlusions were imaged within 4.5 h of stroke onset using the standard local protocol, between November 2012 and February 2013. The median National Institutes of Health Stroke Scale score was 17 (range 9–30). The study population had a mean age of 81 years (range 63–93), comprising 11 women and four men. Three patients demonstrated TICA occlusion, seven demonstrated proximal M1-MCA occlusion while the remaining five showed distal M1-MCA occlusion. Patients with occlusions starting distal to the M1 segment and posterior circulation occlusions were excluded.
Imaging protocol
All patients underwent NCCT, CTA, and a delayed phase (80 s post CTA contrast injection) CECT using a 64 slice scanner (Siemens Medical Systems, Erlangen, Germany). NCCT and CECT were acquired using the following parameters: 120 kVp, 380 mA, 0.6 mm collimation, 1 s/rotation, and pitch 0.85. CTA was acquired using a contrast bolus of 75 ml of Iomeron 400 (400 mg of iodine/ml; Bracco, UK) followed by a 40 ml saline chaser injected via an 18–20 g cannula in the upper limb with a flow rate of 5 ml/s. A bolus tracking technique was used with marker placed at the ascending aorta, triggering at 120 Hounsfield Units (HU) above baseline with a 10 s delay prior to image acquisition. Images were acquired from aortic arch to vertex. CTA parameters were as follows: 120 kVp; 110 mA; 0.37 s/rotation; 0.6 mm thick sections; and table speed 1.2 mm/rotation.
Imaging analysis
Three radiologists independently used a Siemans Syngo workstation to reconstruct 0.6 mm NCCT, CTA, and CECT slices in three planes and the images were co-registered using an automated system. The axial images were first orientated along the axis of the temporal lobe and then adjusted to an orientation parallel to the axis of the occluded vessel, in order that the full length of the thrombus was identifiable on the NCCT image. Thin (0.6 mm) NCCT slices were compared with co-registered 5 mm CECT MIP images. Co-registered CECT and CTA images were compared using 30 mm MIP images to allow measurement of longer vessel lengths on a single image.
For NCCT images, a pixel lens was used to identify the proximal and distal ends of the thrombus with a range of 45–80 HU assumed to represent thrombus. NCCT thrombus and CTA/CECT vascular occlusion measurements were orientated along the central axis of the thrombus on the co-registered NCCT, CECT, and CTA images. When sylvian branches failed to opacify for longer lengths on CTA images, the length of the non-opacifying vessel was measured using the co-registered CECT image as a roadmap. Occlusions in curving vessels were measured using curved reformatted images. When thrombus branched into two or more M2-MCA vessels, the longest thrombus length was measured. For TICA occlusion, the horizontal thrombus within the A1 anterior cerebral artery and M1-MCA was measured but vertical thrombus within the distal internal carotid artery was not included in the measurement. Collateral vessels were assessed on 30 mm CTA MIP images using a scale of 0–314 ,15: 0=absent collateral supply to the occluded MCA territory; 1=collateral supply filling <50% but >0% of the occluded MCA territory; 2=supply filling >50% but <100% of the MCA territory; and 3=100% collateral supply of the occluded MCA territory.
Statistical analysis
Results were compared statistically (Medcalc V.12.4.0, Ostend, Belgium). Thrombus length estimation using NCCT, CTA, and CECT was compared using a two tailed t test. Analysis of variance was used to compare the length of vascular non-enhancement relative to collateral score. Correlation between thrombus length assessed using NCCT and delayed phase CECT was compared using Pearson's correlation coefficient. Inter-rater reliability for NCCT and CECT was assessed using intraclass correlation coefficient.
Results
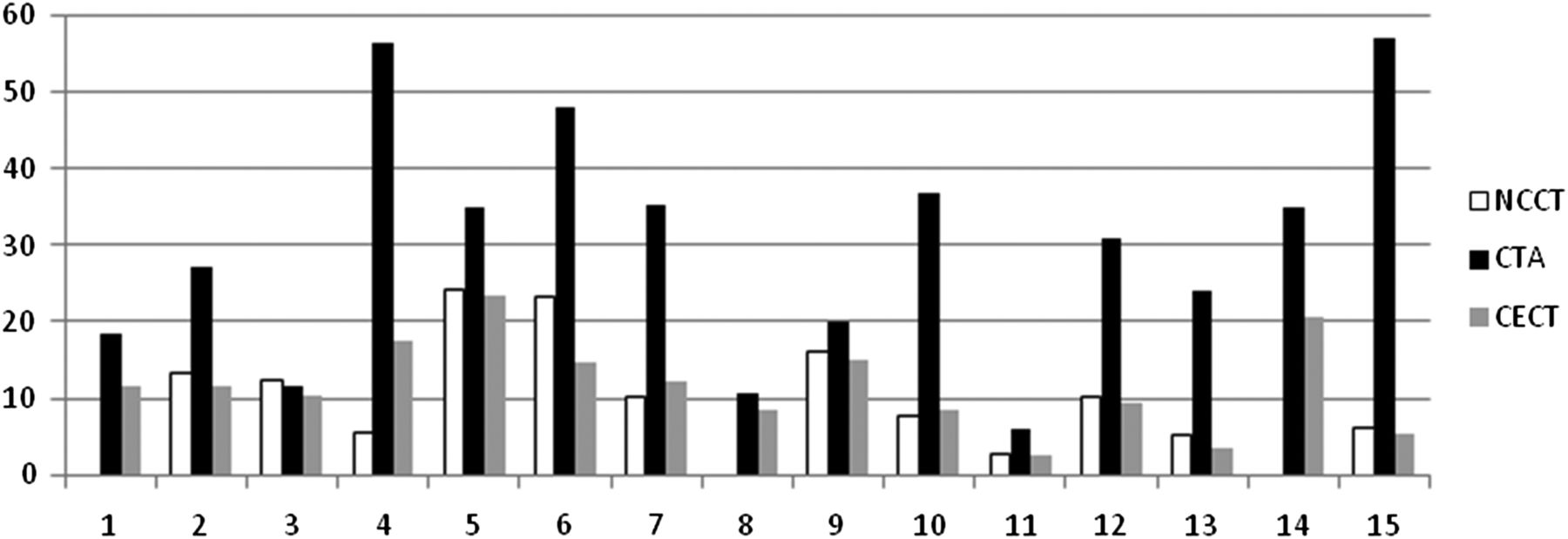
CTA markedly overestimated thrombus load relative to NCCT (p<0.001) and CECT (p<0.001), with significantly longer lengths of sylvian MCA non-enhancement. Mean thrombus lengths/vascular non-enhancement assessed using NCCT, CTA, and CECT are displayed in table 1 and figure 1. Two example cases are shown in figure 2. Ten patients with low collateral scores on CTA (scores 0–1) demonstrated a much greater mean difference between thrombus length assessed using CTA and CECT (24.1 ± 8.77 mm) compared with five patients with good–excellent collateral vessels (scores 2–3) who demonstrated a mean difference of 7.2 ± 12.44 mm (p=0.03). This indicates that the non-opacifying vessel distal to an occlusion on fast acquisition CTA only starts to approximate to true thrombus length in patients with good–excellent collateral flow.
Thrombus length estimation for non-contrast CT, CT angiography, and contrast enhanced CT
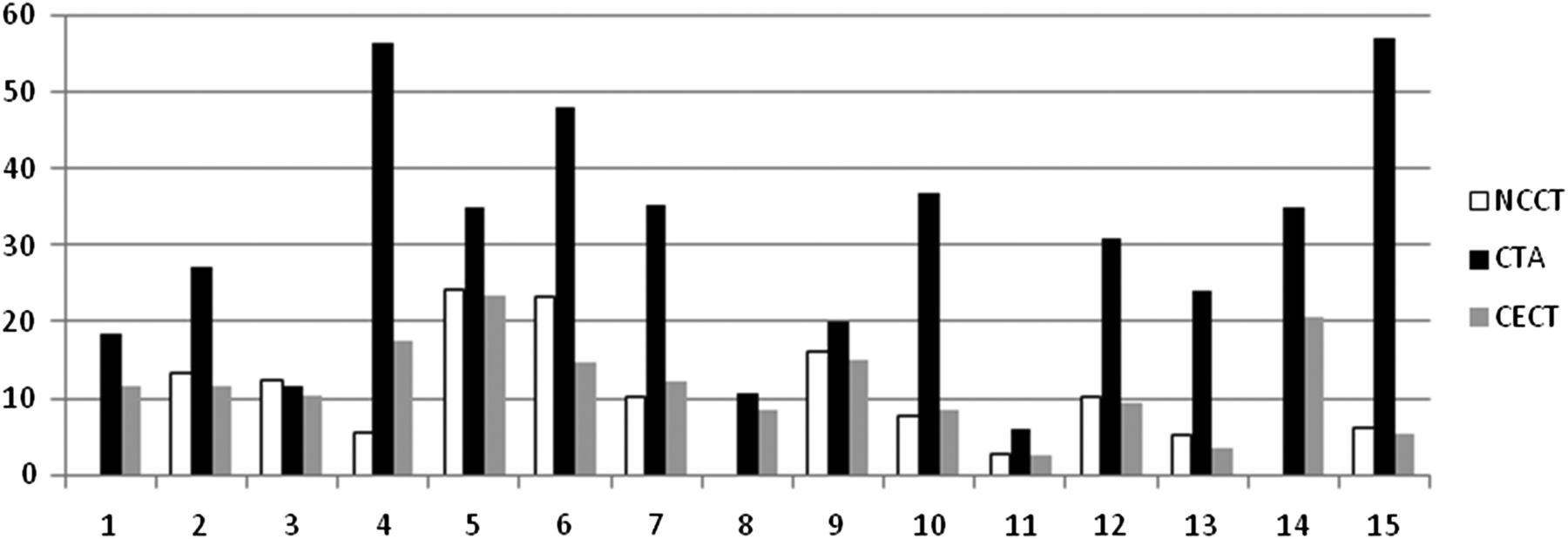
Mean thrombus length estimation (mm) using non-contrast CT (NCCT), CT angiography (CTA), and contrast enhanced CT (CECT) for individual patients (numbered).

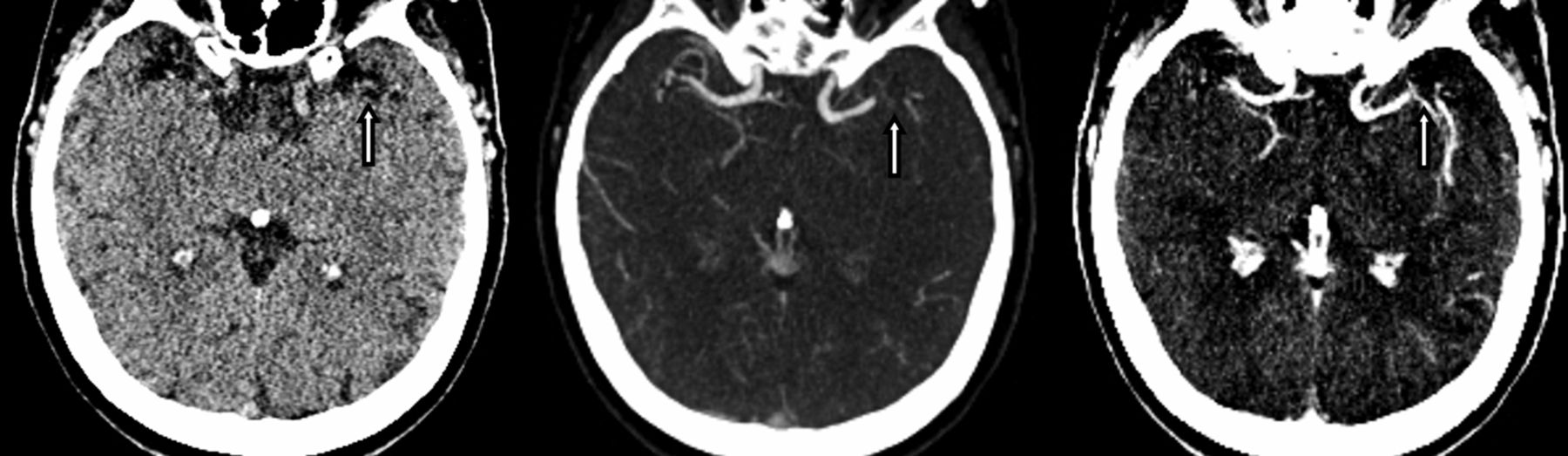
Axial thin slice non-contrast CT (left), thick maximum intensity projection CT angiography (CTA) (centre), and contrast enhanced CT (CECT) (right), demonstrating a right M1-middle cerebral artery occlusion in two patients (A) (top row) and (B) (bottom row). Thrombus is seen as hyperdense material (arrow), the distal extent of which is overestimated by CTA but clearly delineated by delayed phase CECT (arrow).
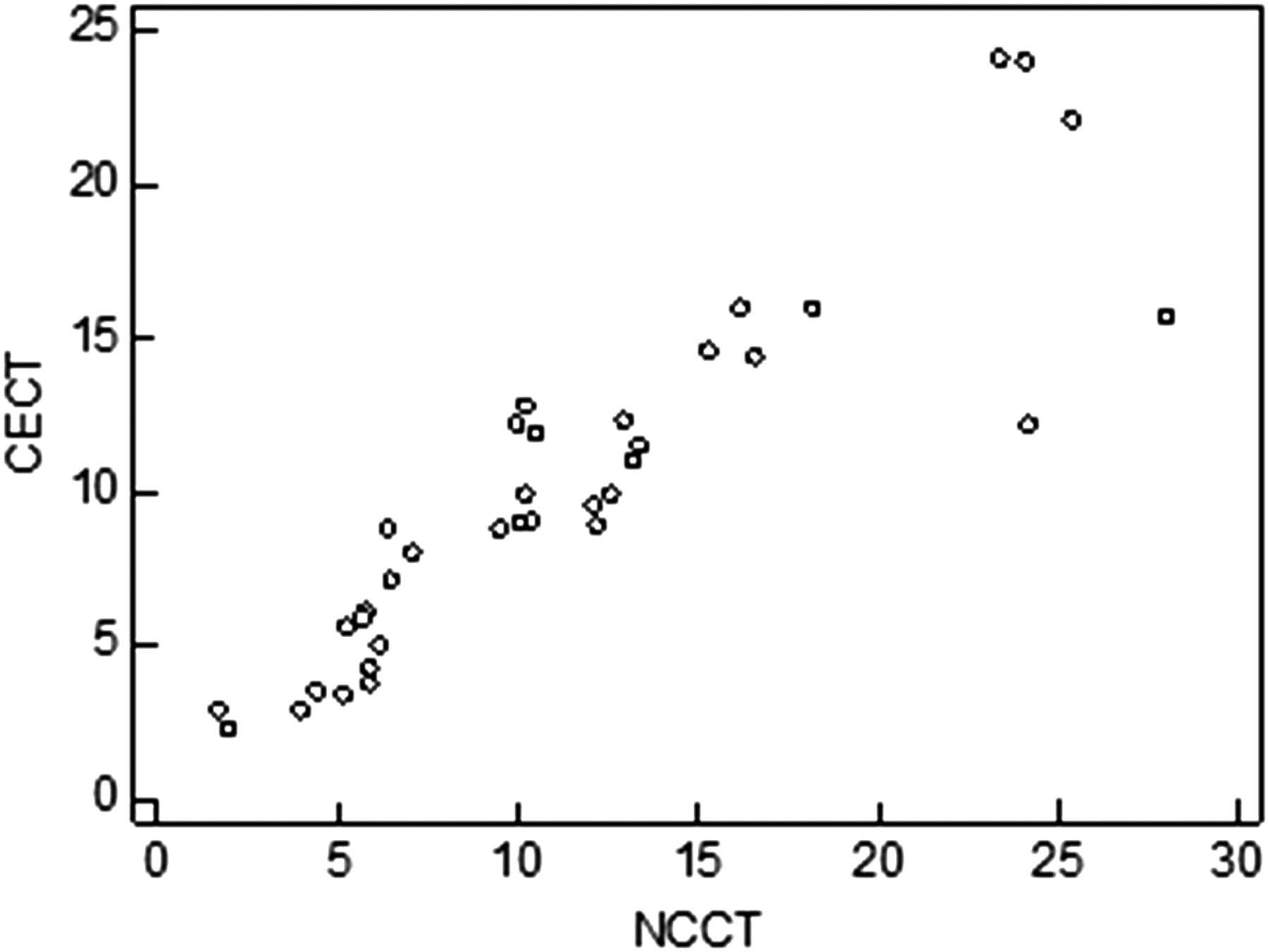
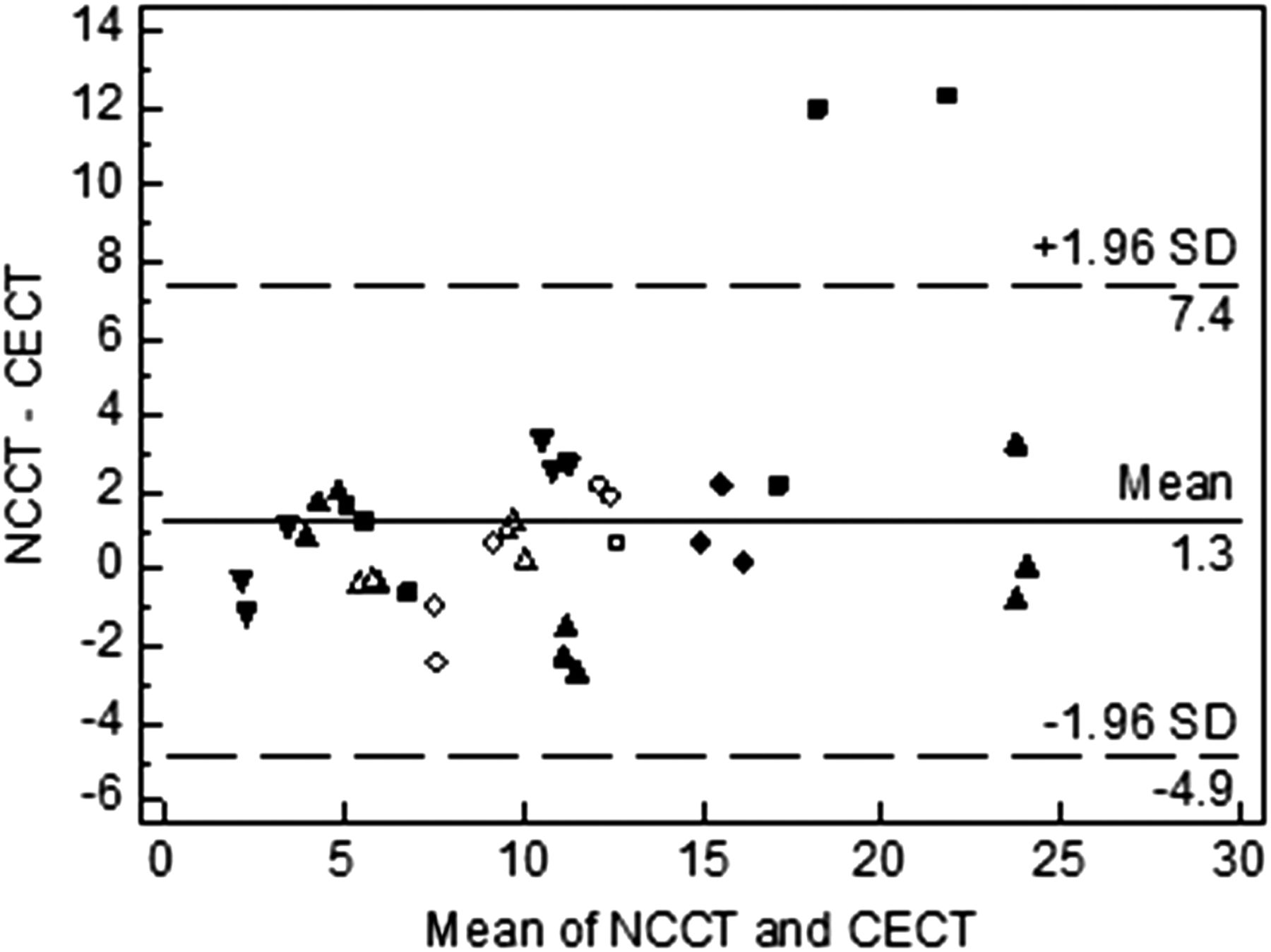
Thrombus could not be identified on NCCT thin slices in three of 15 patients (figure 3). In the remaining 12 patients there was good correlation between NCCT and CECT (Pearson's correlation coefficient=0.90, 95% CI 0.81 to 0.95, p<0.001). This is displayed graphically in figure 4. There was no significant difference between values obtained for NCCT or CECT (p=0.94). The mean difference was 1.3 mm. A Bland–Altman plot demonstrating thrombus length measurements for each subject by each radiologist can be seen in figure 5. Inter-rater variability assessed using intraclass correlation was 0.95 (95% CI 0.87 to 0.98) for NCCT and 0.98 (95% CI 0.94 to 0.99) for CECT.
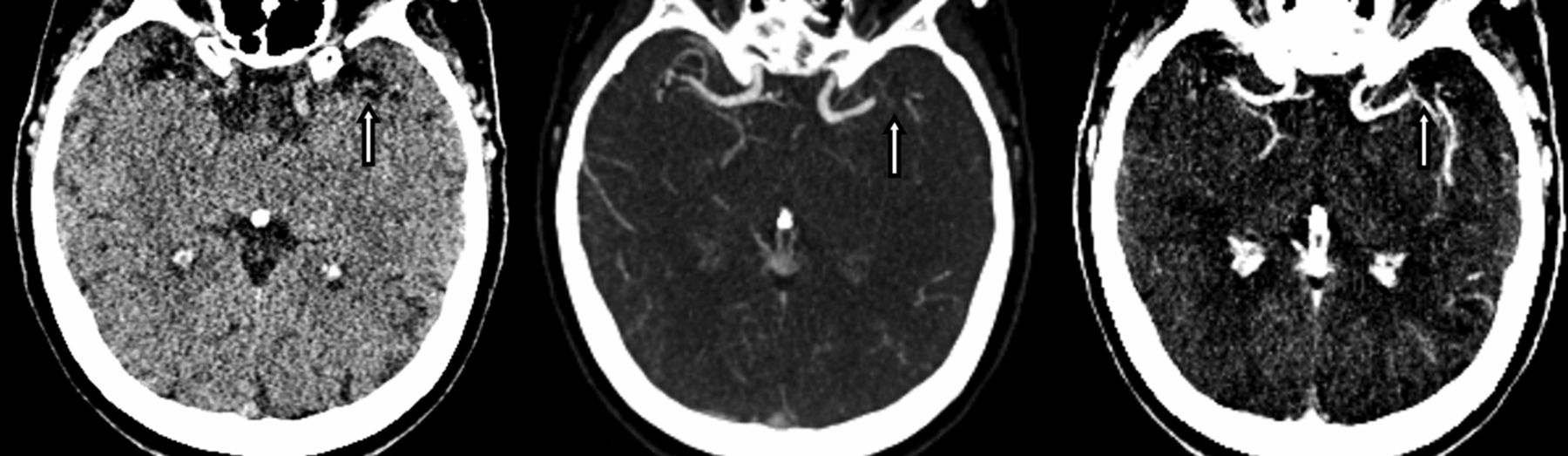
Distal left M1-middle cerebral artery (MCA) occlusion not seen on thin slice non-contrast CT (left, arrow) but clearly identified on CT angiography (centre, arrow) and contrast enhanced CT (CECT) (right, arrow). There is closer approximation between the two contrast enhanced scans in this example although the distal end of the thrombus can be identified with more confidence on CECT.
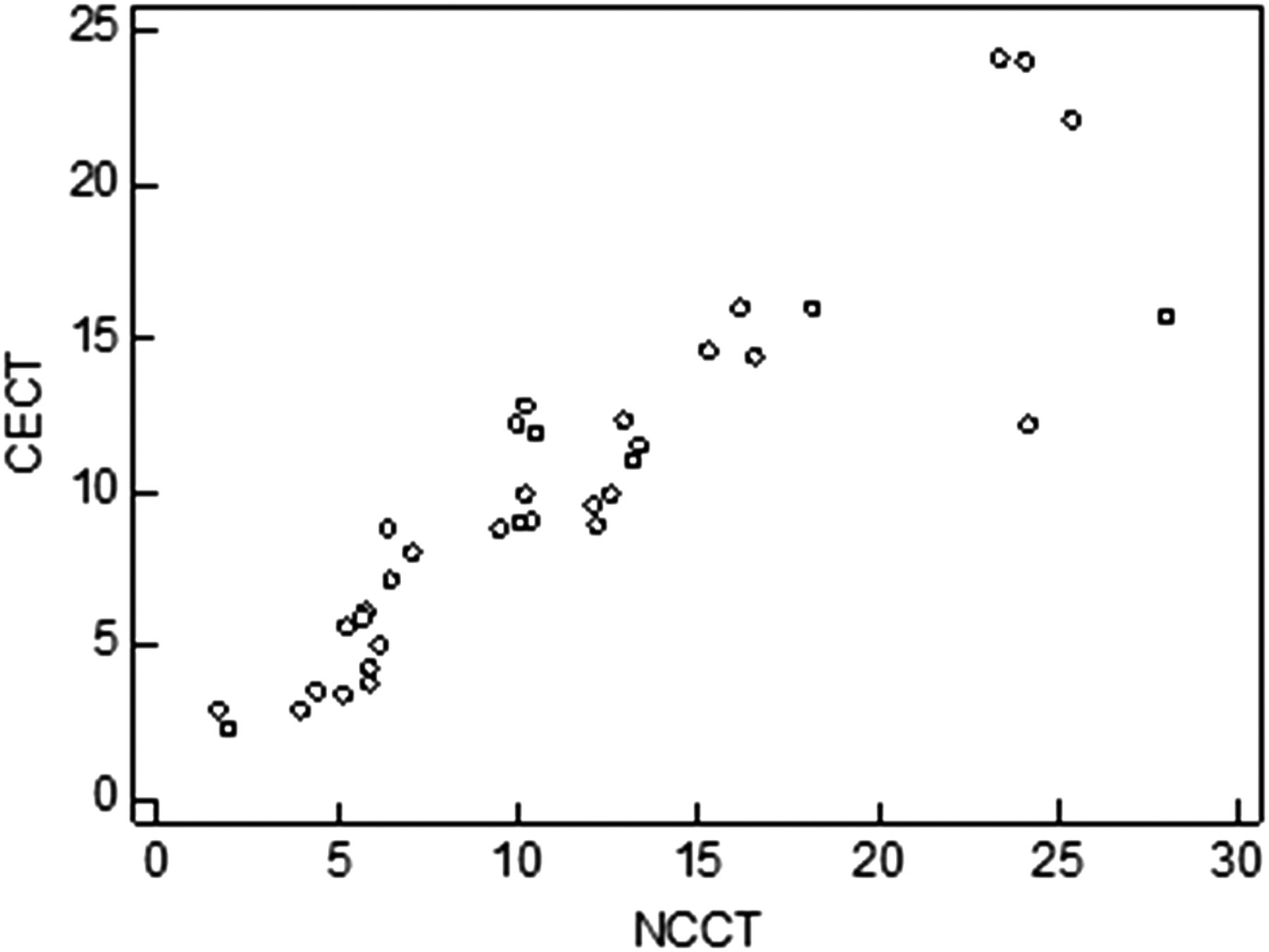
Scatterplot demonstrating the relationship between thrombus length (mm) on non-contrast CT (NCCT) and contrast enhanced CT (CECT) on three radiological reads.

Bland–Altman plot comparing thrombus length measurement on non-contrast CT (NCCT) and contrast enhanced CT (CECT) on three radiological reads.
Discussion
Thrombus length estimation is increasingly recognized as an important variable in the likelihood of a response to IV rtPA,1 ,2 and longer thrombus length could become an indication for endovascular treatment.3 Accurate thrombus length measurement is therefore an important parameter to assess on initial imaging. We have shown that CECT showed good agreement with thin slice NCCT which has previously been used as a tool to accurately assess thrombus length.1 ,2 ,16 This finding is of value as, depending on thrombus structure, it may not be seen on NCCT4 and vascular calcification or polycythemia may mimic thrombus or preclude accurate measurement using NCCT. Indeed, dense thrombus was not seen in three of 15 patients in our study despite the use of 0.6 mm slice thicknesses. Alternatively, CECT will demonstrate site of vascular occlusion and display thrombus length independent of thrombus density. CECT is swift and requires very little post processing, and we have shown that length estimation using this technique shows good inter-rater reliability.
The mean difference between NCCT and CECT was 1.3 mm. These differences (both over and underestimation of length relative to NCCT) will stem partly from experimental error but the co-registration used in this investigation allowed us to simultaneously compare thrombus on NCCT and CECT using on-screen cursors. As a result, we hypothesize that in some cases, CECT may underestimate full thrombus length as it only demonstrates the occlusive length and non-occlusive thrombus at proximal and distal ends of the lesion may be obscured by contrast. Additionally, CECT may underestimate occlusion length as dense thrombus mimics contrast opacification (figure 6). This likely accounted for the most extreme outlier in our study. Conversely, NCCT may underestimate thrombus length as, depending on its constituents, less dense material may fail to be recognized as thrombus.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Long left middle cerebral artery thrombus demonstrated on non-contrast CT (left, arrows). The advantage of early arterial CT angiography in clearly demonstrating the site of occlusion (centre, arrow) relative to delayed contrast enhanced CT, on which it is difficult to differentiate thrombus from contrast without careful re-windowing (right, arrows).
We have also demonstrated that fast acquisition CTA significantly and consistently overestimates thrombus load. This study confirms the hypothesis that early arterial fast acquisition CTA fails to delineate the distal extent of the thrombus and that it is not a reliable tool in thrombus length estimation. In many cases, these images are acquired prior to collateral dependant retrograde flow of contrast to the distal end of the thrombus. Our findings also suggest that retrograde flow is dependent on the quality of pial collaterals: patients with better collateral status demonstrated a smaller difference in the length of the MCA that failed to opacity with contrast when CTA and CECT were compared. While 50% of patients demonstrated distal clot delineation in one conventional angiographic study,17 in our cohort, few patients had sufficient collateral flow to clearly delineate the distal thrombus extent on early arterial CTA, with only two of 15 patients demonstrating length measurements within 2 mm of each other on both CTA and CECT. However, delayed phase imaging with CECT allows several passes of contrast and therefore there is greater potential for slower retrograde flow of contrast via pial collaterals so that the distal clot face is delineated.
When designing acute stroke imaging protocols, one option is to perform a single acquisition CTA on the venous side of the perfusion curve in order to obtain this information. However, in our opinion, fast acquisition CTA is useful in acute stroke imaging. There is less venous contamination and the site of occlusion is often more clearly demonstrated, especially with short thrombi or when the hyperdensity of the thrombus can mimic contrast medium, so obscuring thrombus on a more delayed acquisition. Additional information can also be obtained through imaging the cervical vessels, especially if intervention is being considered. However, estimation of core infarct on fast acquisition CTA source images is overestimated compared with diffusion weighted MR imaging,10 ,11 and parenchymal hypodensity approximating to cerebral blood flow rather than cerebral blood volume CT perfusion maps.13
A delayed phase CECT has drawbacks of extra irradiation but as well as the information on occlusion length, there are additional benefits in terms of the information gleaned from this examination: it can be used as an estimate of core infarct. Pulli et al11 suggested that a delay of approximately 40 s post contrast injection will result in imaging equivalent to CT angiographic source images acquired using older, slower CT scanners that demonstrated hypodensity that closer approximated to core infarct on diffusion weighted imaging. Others suggest a longer delay of 80–120 s.12 ,13 Sharma et al13 have demonstrated approximation of cerebral blood volume infarct volume with CECT, obtained at 120 s following injection.
This was a small retrospective study and we accept that there will be a degree of error in thrombus length measurement. However, the findings do highlight a simple clinically feasible technique that may prove useful in the future clinical setting for rapidly estimating thrombus length, especially in the absence of thrombus hyperdensity on NCCT. It is possible that the principles underlying our findings can be applied to the use of CT perfusion source images, or time resolved/4D CTA, for estimation of thrombus length. However, currently, this technique is a simple accessible way of obtaining these data.
References
Footnotes
-
Contributors All authors contributed to the conception and design, acquisition of the data, or analysis and interpretation of the data. All authors played a role in drafting the article or revising it critically for important intellectual content, and all authors were involved in final approval of the version to be published.
-
Competing interests None.
-
Ethics approval The study was approved by the Institutional Clinical Effectiveness and Audit Department.
-
Provenance and peer review Not commissioned; externally peer reviewed.