Article Text

Abstract
We present a young woman with rapidly progressive neurologic decline in the setting of malignant cerebral edema due to extensive superior sagittal sinus thrombosis and cortical venous thrombosis despite intravenous heparin administration. Complete revascularization of the occluded sinus was achieved using suction thrombectomy with the 5 max Penumbra catheter in combination with the Solitaire FR clot retrieval device. The successful endovascular treatment halted the progression of her cerebral edema, and the patient eventually had an excellent recovery after prolonged intensive medical therapy. To our knowledge, this is the first reported case describing such a combined mechanical approach for cerebral venous sinus thrombosis. The clot retrieval properties of the Solitaire device combined with direct aspiration via the newest generation Penumbra catheters may allow more rapid, safe and efficient revascularization than all previously reported endovascular treatments for this potentially devastating condition.
- Vein
- Thrombectomy
- Hemorrhage
- Intracranial Pressure
- Stroke
Statistics from Altmetric.com
Background
Endovascular therapy for cerebral venous sinus thrombosis (CVST) is currently accepted as a second-line treatment for patients who have failed or those in whom systemic anticoagulation is contraindicated.1 A number of different mechanical and pharmacologic endovascular strategies have been reported, either as separate or combined approaches. The newest generation thrombectomy devices designed for arterial recanalization in acute ischemic stroke, including the Penumbra aspiration system (Penumbra, Alameda, California, USA) and the Solitaire FR thrombectomy device (Covidien Neurovascular, Irvine, California, USA), have also been used with acceptable safety and efficacy. This is the first reported case to illustrate the additive benefit of both devices applied in combination for the successful treatment of CVST causing rapidly progressive malignant edema and impeding fatal herniation.
Case presentation
A 27-year-old woman on oral contraceptives with a history of prior deep vein thrombosis presented with acute left-sided weakness and headaches followed by a generalized seizure. A non-contrast head CT scan demonstrated increased attenuation within the anterior portion of the superior sagittal sinus (SSS) and few cortical veins, associated with subtle bifrontal edema (figure 1). Subsequent multimodal CT confirmed the diagnosis of SSS thrombosis (figure 2). The patient was treated medically with hydration, anticoagulation and antiepileptics. However, she became more lethargic over the next 24 h and follow-up imaging demonstrated progression of her SSS thrombosis with worsened bilateral R > L frontoparietal edema, 5 mm midline shift, as well as petechial hemorrhage in the right perirolandic region (figure 3). Given the progressive thrombosis and clinical deterioration despite maximum medical therapy, a decision was made to proceed with endovascular intervention.

Initial non-contrast head CT demonstrating increased attenuation within the anterior portion of the superior sagittal sinus with only subtle bifrontal edema.
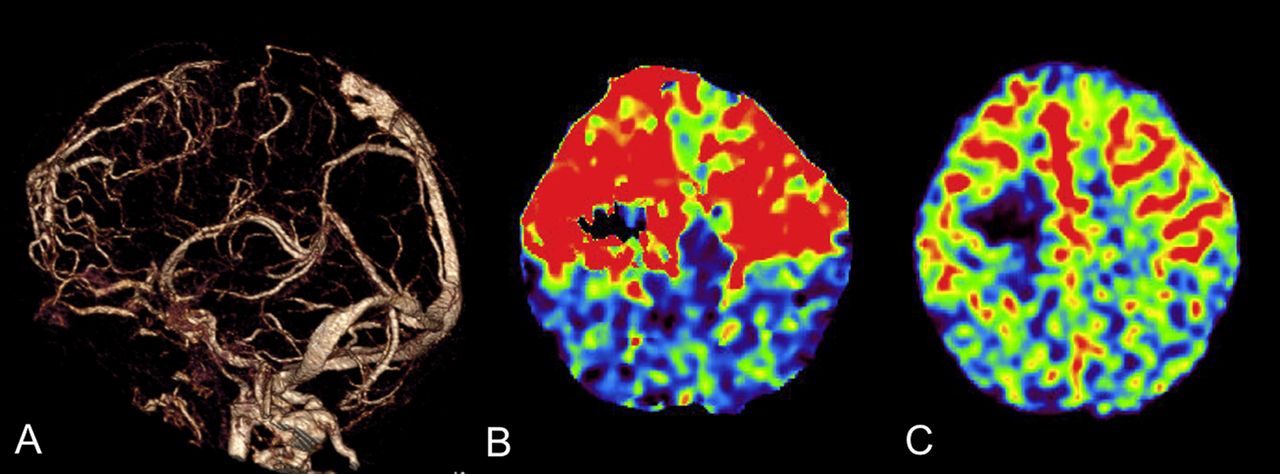
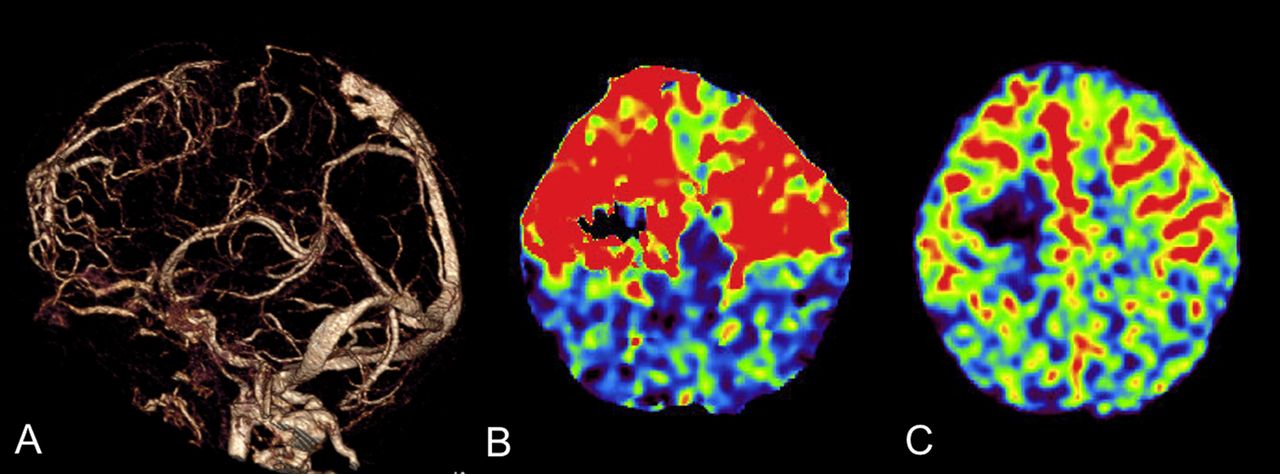
Multimodal CT demonstrating absence of continuous flow within the anterior two-thirds of the superior sagittal sinus (A) with associated prolongation of mean transit time (B) and increased cerebral blood volume (C) in both frontal hemispheres.

Follow-up non-contrast head CT (A) and MR FLAIR sequence (B) demonstrating worsening R>L, frontoparietal edema with mass effect on the right lateral ventricle and septal shift. There are small petechial hemorrhages in the perirolandic region (arrows).
The initial diagnostic angiogram demonstrated near complete occlusion of the anterior two-thirds of the SSS as well as occlusion within multiple cortical veins with associated severely delayed R > L arteriovenous transit time (figure 4).

Lateral view of the right internal carotid artery angiogram demonstrating near complete occlusion within the anterior two-thirds of the superior sagittal sinus (large arrows) and several cortical veins (small arrows).
Treatment
An 80 cm 6 Fr shuttle sheath was inserted in the right internal jugular vein. Next, a 5 Max Penumbra reperfusion catheter was navigated within the anterior portion of the SSS over a coaxially inserted Marksman microcatheter and Traxcess 14 microguidewire (figure 5). A Solitaire FR 4×20 mm clot retrieval device was then deployed in the anterior portion of the thrombosed SSS. Once the device was fully deployed, the microcatheter was completely removed to allow more space for aspiration via the 5 Max. The Solitaire FR was then pulled into the 5 Max, which was connected to the Penumbra aspiration system. Using the same technique, two more sequential passes from the proximal to the distal aspect of the SSS were made with a Solitaire FR 6×30 mm under continuous aspiration via the 5 Max catheter, which remained positioned within the SSS. Large clot fragments were removed from the Solitaire FR after each pass (figure 6). Additional clot aspiration throughout the thrombosed SSS was performed through the Penumbra 5 Max catheter with the use of the separator. Although there was antegrade flow in the SSS at this point, residual wall adherent thrombus in the SSS was targeted with two more pulls with the Solitaire 6×30 mm device while aspirating via the 5 Max. The final post-intervention angiogram revealed complete recanalization of the previously occluded SSS with some residual cortical venous thrombosis and significantly improved arteriovenous transit time (figure 7).
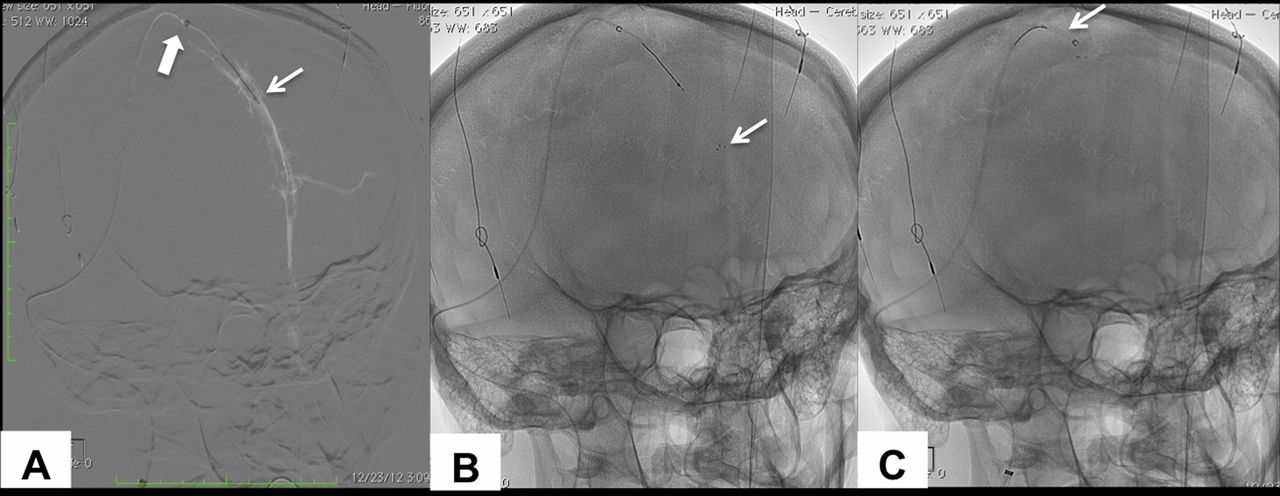
(A) Oblique road map view of the occluded superior sagittal sinus (SSS) demonstrating the coaxially inserted Marksman (small arrow) within the more proximally positioned 5 Max Penumbra catheter (large arrow). (B) Plain unsubtracted view of (A) demonstrating the deployed Solitaire FR within the anterior portion of the occluded SSS (arrow). (C) Solitaire FR device retrieved into the 5 Max Penumbra catheter.

Clot removed from the Penumbra canister and the Solitaire FR retriever.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Right internal carotid artery (ICA) angiogram lateral projection demonstrating improved intraluminal flow with residual partially obstructive thrombus within the superior sagittal sinus (SSS) (arrows). (B) Road map view of (A) showing the Solitaire FR (small arrows) deployed within the SSS through the 5 Max (arrow). (C) Final right ICA angiogram demonstrating complete recanalization of the SSS with no residual wall-adherent thrombus and persistently occluded cortical veins. (D) Right ICA angiogram 2 weeks after the intervention demonstrating complete patency of the previously occluded SSS and cortical veins with normalized arteriovenous transit time.
Outcome and follow-up
The patient had a lengthy and complicated hospital stay over the course of 6 weeks, requiring a prolonged period of barbiturate-induced coma and multiple combinations of antiepileptic regimens to achieve control of her refractory seizures. She remained on full-dose intravenous heparin throughout her hospital stay followed by oral long-term anticoagulation.
The follow-up angiogram performed 15 days after the intervention demonstrated complete recanalization of her cortical venous thrombosis with essentially normal venous vasculature (figure 7). Three months later the patient was completely independent with no significant cognitive dysfunction and only minimal and improving left hand and foot weakness (modified Rankin Scale score=1).
Discussion
Despite the overall favorable outcome with systemic anticoagulation, CVST can be potentially devastating, particularly in a clinically identifiably subgroup of patients presenting with rapid neurologic deterioration.2 The severity of the clinical symptoms is proportional to the degree of vasogenic and cytotoxic edema secondary to compromised venous collateral flow, particularly in cases with cortical venous extension.3–5 These pathophysiologic changes can lead to fatal herniation, sometimes requiring decompressive life-saving craniectomy.6
While the therapeutic effect of systemic anticoagulation is mainly to prevent thrombus propagation, endovascular intervention can lead to immediate revascularization and restoration of normal venous flow.7 As such, mechanical thrombectomy has been proposed as a first-line approach for CVST.8 The authors used various sizes of AngioJet catheters designed for use in the coronary and peripheral vasculature. A potential disadvantage of this device over all other devices for intracranial use is its navigability, especially in larger sizes required for large clot burdens, and the high risk of clot fragmentation and emboli.9
Both the Penumbra aspiration system and the Solitaire FR device have been used separately for the treatment of CVST.10 ,11 However, none of the reported cases clearly demonstrates the benefit of either device for impeding fatal herniation with septal shift and avoidance of decompressive hemicraniectomy. Our goal was to achieve complete revascularization without surgical intervention, which would have required reversal of anticoagulation and potential further clot propagation.
We elected to use the combination of these devices for several reasons. First, both devices have been designed and proved safe and efficacious for intracranial use. Second, the ability to position the 5 Max at the clot allowed direct continuous aspiration during the Solitaire retrieval, which maximized the recanalization efficacy and potentially minimized the chance of pulmonary emboli. The 5 Max allowed persistent and immediate re-access after each pass with the Solitaire FR. Finally, we aimed for complete recanalization and removal of residual wall-adherent clot from the orifices of the cortical veins, as partial recanalization of the occluded sinus may not improve the compromised venous outflow.12 This was achieved by the clot engagement properties of the Solitaire FR.
In our opinion, the use of both devices halted the progression of the patient's malignant edema and also prevented potentially more costly and invasive surgical decompression.
It is important to emphasize that the technical success was an addition rather than an alternative to the systemic anticoagulation. The aggressive management of the patient's edema and seizures also prevented potentially irreversible brain damage and eventually led to an excellent clinical outcome.
Conclusions
This case report describes a novel and previously unpublished technical approach to CVST that can be immediately applied to clinical practice. It also raises awareness among the neurosurgical and neurological community about novel potentially life-saving endovascular treatments without the need for decompressive hemicraniectomy in patients with malignant edema due progressive CVST.
Key messages
-
Complete mechanical revascularization combined with aggressive medical therapy may reverse malignant cerebral edema and obviate the need for decompressive surgery in the setting of rapidly progressive cerebral venous sinus thrombosis.
-
The Penumbra system offers efficient intraluminal recanalization of the occluded sinus, while the use of the Solitaire FR device allows complete removal of residual wall-adherent clots.
-
The application of both devices in combination can be particularly useful in cases with large clot burdens and compromised cortical venous outflow requiring complete revascularization for prevention of fatal herniation.
Footnotes
Republished with permission from BMJ Case Reports Published 10 September 2013; doi:10.1136/bcr-2013-010866
-
Contributors RR, ST, SR and AB performed the procedure. RR and BY were involved in the initial management of the patient. PV, JS, and MB were involved in the management of the patient during the course of her hospitalisation.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.