Article Text

Abstract
Purpose New ischemic brain lesions are common findings after cerebral diagnostic angiography and endovascular therapy. Diffusion-weighted MRI (DWI) can be used for detection of these lesions. The aim of the present study was to investigate the incidence of DWI lesions after stent-assisted coiling and the evaluation of possible risk factors.
Methods The study included a total of 75 consecutive patients treated with stent-assisted coiling. Post-procedural DWI of the brain was performed to detect ischemic lesions. Demographic data, aneurysm characteristics and angiographic parameters were correlated with properties of DWI lesions.
Results In post-procedural DWI, 48 of the 75 patients (64%) had 163 DWI lesions in a pattern consistent with embolic events. The number of patients with DWI lesions was significantly increased in older patients (≥55 years) and longer intervention times (≥120 min). The ischemic brain volume was significantly increased in older patients (≥55 years) as well as in patients who were implanted with a shorter stent (<20 mm).
Conclusions Thromboembolic events are common after stent-assisted coiling with an incidence comparable to DWI studies after coiling alone. Despite several devices and low operator experience, stent-assisted coiling for intracranial aneurysms has a very low risk of permanent neurologic disability. Further studies are necessary to improve the safety of stent-assisted coiling for patients in conditions with increased risk potential (age, procedure time, stent length).
- Aneurysm
- Coil
- Stent
Statistics from Altmetric.com
Introduction
Stent-assisted coiling has improved the ability to treat complex aneurysms such as fusiform and wide-necked aneurysms.1 Self-expanding stents provide mechanical, hemodynamic and biological benefits by preventing coil protrusion into the parent artery, reducing intra-aneurysmal flow and promoting vessel wall healing.2 Further studies have shown this device to be an effective tool in treating pathological entities that were not previously considered suitable for endovascular therapy.3 ,4 However, while stent-assisted coiling provides another treatment option for endovascular repair, additional risks are associated with supplemental stent placement compared with coiling alone.1
Some authors have hypothesized that the use of an adjunctive device could increase the rate of periprocedural thromboembolic events.5 ,6 These events can have different causes including friable plaques, dissection of parent vessels, air bubbles and thrombi within aneurysms and catheters.7 In most cases these thromboembolisms cause small ischemic brain lesions and remain clinically silent.8 These lesions are therefore only detectable by postprocedural diffusion weighted imaging (DWI).9 However, there is increasing evidence that the cumulative burden of ischemic brain injury might cause minor deficits or aggravate vascular dementia,10 especially in older patients with smaller brain volumes and decreased neuronal plasticity. It therefore seems reasonable to monitor and investigate those small ischemic lesions (DWI lesions). Moreover, DWI lesions might be established as a surrogate parameter for potential risk factors in order to optimize stent-assisted coiling in future.
Although a number of studies have investigated the incidence of DWI lesions after interventional procedures using coiling alone,11–14 to our knowledge only two DWI studies have assessed the use of adjunctive devices for aneurysm treatment including stent-assisted coiling.15 ,16 However, case numbers were relatively low and study design heterogeneous. Data focusing solely on the stent-assisted coiling procedure are lacking.
In the present study we retrospectively evaluated the characteristics of DWI lesions after stent-assisted coiling in patients with unruptured aneurysms and thereby analyzed possible risk factors associated with DWI lesions.
Materials and methods
Patients
We retrospectively analyzed all patients with unruptured cranial aneurysms who consecutively underwent endovascular stent-assisted coiling procedures within our institution between January 2003 and September 2011 (n=87). For therapy control the standard follow-up protocol consisted of a post-procedural MRI including DWI. Patient age and sex, aneurysm location, aneurysm size, type and size of stent, number of coils and neurologic complications were recorded. In order to homogenize the study group, 12 cases were excluded due to implantation of more than one stent (n=5) or a post-interventional interval for diagnostic MRI of >5 days (n=7). All types, sizes and locations of aneurysms were included. Table 1 summarizes the characteristics of the cohort (n=75).
Characteristics of study cohort (n=75)
Medication
Until February 2006, all patients were temporarily administered therapeutic heparinization (typically 5000 U during the procedure). Activated clotting times were checked prior to the procedure. In addition, aspirin and clopidogrel were given prior to the procedure (either 100 mg aspirin +75 mg clopidogrel over a period of at least 7 days or 500 mg aspirin +300 mg clopidogrel on the day of the procedure). Heparin was discontinued after the procedure. 75 mg clopidogrel/day was continued at least for 6 weeks after procedure and 100 mg/day aspirin was given lifelong continuously after treatment. After February 2006 a regimen change in the administration of heparin was done to reduce the risk of periprocedural bleeding. Patients were pre- and post-procedurally given only dual antiplatelet therapy (aspirin and clopidogrel) as mentioned above. All flushing solutions including the guiding catheters and microcatheters were heparinized (1000 U/L).
Procedure and analyses
The stent-assisted coiling procedure was performed under general anesthesia. In 82.7% of cases (n=62) Neuroform stents (Stryker, Kalamazoo, Michigan, USA) were used, in 12% of cases (n=9) Enterprise stents (Codman, J&J, Raynham, Massachusetts, USA) were used and in 5.3% (n=4) LEO stents (Balt, Montmorency, France) were implanted. The stent length ranged between 15 and 50 mm. Different types of coils were implanted (Guglielmi detachable platinum coils, Stryker, Fremont, California, USA; bare and hydrogel coated coils, MicroVention, Tustin, California, USA). The stent-assisted coiling procedure was performed by four different interventional neuroradiologists with ample experience in all types of stent-assisted neurointerventional procedures. Diagnostic MRI was performed 0–5 days after endovascular treatment (mean 2 days) on a 1.5 or 3 Tesla MRI (Sonata, Symphony, Avanto, Espree, Aera, Skyra; Siemens Healthcare, Erlangen, Germany). The MRI protocol included diffusion-weighted sequences (a typical protocol example for the 1.5 T Sonata: section thickness=6 mm, TR/TE 2900/84, field of view 230, b values 0 s/mm2 and 1000 s/mm2; and for the 3 T Skyra: section thickness=6 mm, TR/TE 4000/84, b values 0 s/mm2 and 1000 s/mm2). If DWI abnormalities were detected, their number, location and size were recorded.
In order to compare the dimension of the patients’ ischemic brain lesions, the whole ischemic volume in each patient was determined. By means of manual segmentation, the maximal area of a lesion was measured and multiplied by the slice thickness of the DWI. Each measurement was done at a standard PACS work station.
Statistical analyses
Values are presented as mean±SD. The Fisher exact test and Student t test were applied for analysis. A two-sided p value<0.05 was considered significant.
Results
DWI lesions numerical data
A total of 75 consecutive cases were included for analysis (72% women, 28% men; mean age 52.6±10.4 years). Overall, 163 ischemic lesions were observed in 48 of the 75 patients (64%); an example is shown in figure 1.
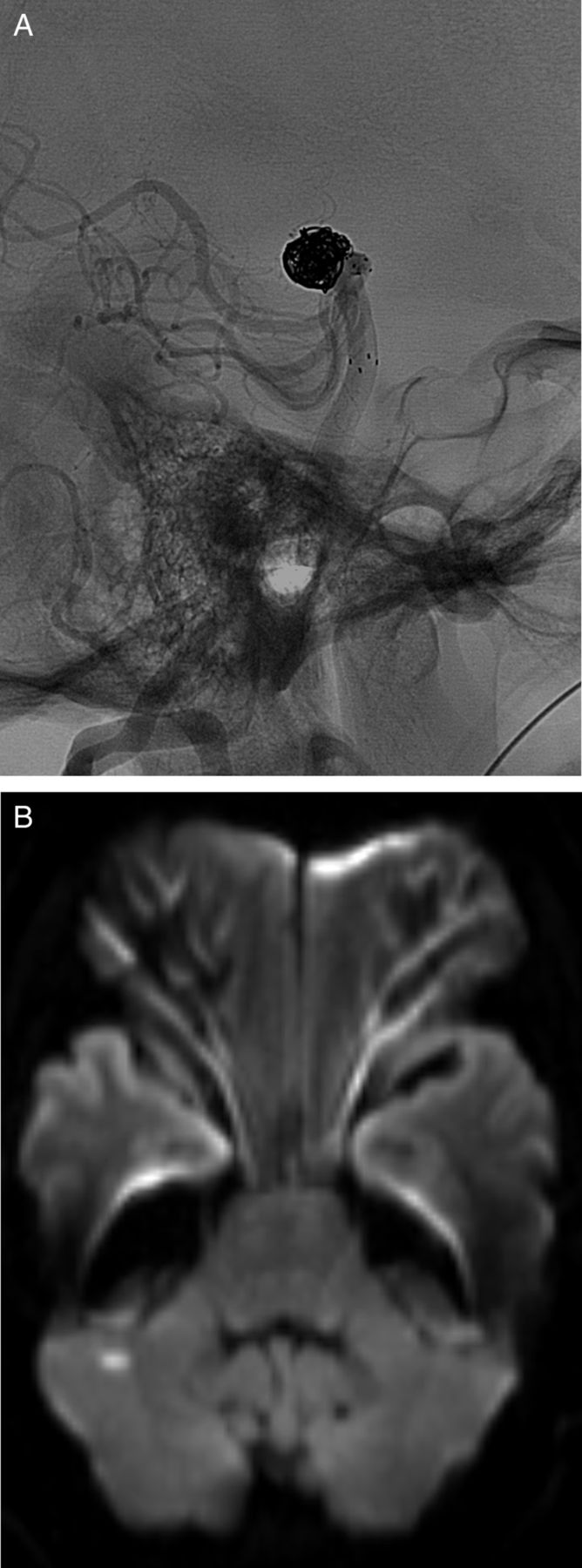
(A) Cerebral angiogram of a patient with silent embolism after stent-assisted coiling of a basilar artery aneurysm. (B) Diffusion-weighted imaging shows a small ischemic lesion in the right cerebellar hemisphere 1 day after stent-assisted coiling.
We found only embolic types of ischemic lesions. The size and distribution in the vascular territory were indicative of their embolic origin; 34 of the 48 patients (45.3%) had 1–3 ischemic lesions, 12 patients (16%) had 4–9 lesions and only two patients (2.7%) had ≥10 lesions (mean number of lesions 2).
Five of the 48 patients developed a new apparent neurologic deficit after stent-assisted coiling (6.7% based on 5/75). Four of these five patients fully recovered before discharge, the remaining patient (1.3%; 1/75) developed a permanent deficit (hemiparesis).
As shown in table 2, most of the ischemic lesions were <5 mm in diameter (87.1%); 18 lesions (11%) had a diameter between 5 and 15 mm, 2 lesions (1.2%) had a diameter between 15 and 25 mm and 1 lesion (0.6%) had a diameter of >25 mm.
Characterization of ischemic lesions observed
In 44 of the 48 patients (91.7%), new ischemic lesions were found only in the territory of the endovascular treated vessel. Two of the remaining four patients revealed new ischemic lesions in different vascular territories, including the territory downstream from the treated aneurysm. The other two patients showed new ischemic lesions only in a vascular territory remote from the treated aneurysm. All of the four patients received diagnostic angiography within 5 days before treatment and the post-procedural DWI.
Characteristics of patients with ischemic lesions
Lesions were significantly more frequent in older patients (≥55 years, p=0.007) and in patients with longer procedure times (≥120 min, p=0.027). Patients’ mean age did not differ between the group with procedure times <120 min (50.9 years, SD 11.3, n=45) and ≥120 min (55.3 years, SD 8.2, n=30). No significant association was found with respect to sex, aneurysm location, aneurysm size, length of stent, number of implanted coils, heparin administration and pre-interventional antiplatelet therapy.
Analysis by means of calculation of the total volume of the ischemic lesions
In order to compare the volume of the ischemic lesions between patients, the total volume of ischemic lesions was determined. Total ischemic volumes ranged from 68 to 4958 mm3 (mean 338 mm3, median 136 mm3). Ischemic lesion volume was found to be significantly increased in older patients (≥55 years) compared with younger patients (<55 years, p=0.03; figure 2A). Patients with a shorter stent (<20 mm) had a significantly increased ischemic lesion volume compared with patients with a longer stent (≥20 mm, p=0.03, figure 2B). Sex, location of the aneurysm, aneurysm size, procedure time, number of coils, heparinization and pre-interventional antiplatelet therapy had no significant effect on the post-procedural ischemic volume.

{kind=link}
{kind=link}
Analyses by means of calculation of the total volume of the ischemic lesions. Significantly higher ischemic brain volume was seen in patients aged ≥55 years compared with patients aged <55 years (A) and in patients implanted with a stent <20 mm in length compared with patients implanted with a stent ≥20 mm in length (B). *p<0.05.
Discussion
Ischemic brain lesions after diagnostic and interventional cerebral angiography and their significance for clinical outcome are still a matter of debate. Our retrospective study revealed a very low permanent neurologic complication rate (1.1%), whereas small and usually clinically asymptomatic ischemic lesions (DWI lesions) are found to be relatively frequent after stent-assisted coiling (64%). Only 5 of 75 patients (6.7%) had neurologic deficits and only 1 (1.3%) of these 5 patients maintained a permanent deficit. We found a correlation between the incidence of DWI lesions and age of the patients, as well as between the incidence of DWI lesions and procedure time. DWI lesions occurred more often in older patients (≥55 years) and in patients with longer procedure times (≥120 min). These correlations have already been described by other authors investigating DWI lesions after coiling alone.17 ,18 Both findings might be explainable by an increased grade of atherosclerosis in older patients leading to prolonged procedure times.19
To our knowledge, only two studies have investigated DWI after stent-assisted coiling.15 ,16 Brooks et al15 found DWI lesions in only 15% of 14 patients with unruptured aneurysms after stent-assisted coiling and Altay et al16 found DWI lesions in 30% of 46 patients with unruptured aneurysms treated with stent-assisted coiling. Compared with our results, both studies clearly showed a lower incidence of DWI lesions after stent-assisted coiling. We observed DWI lesions in 64% of all cases investigated (n=75). Additionally, we compared our data with studies of conventional coiling alone in order to estimate the risk of the stent-assisted coiling procedure compared with the more commonly performed procedure. In DWI studies only considering conventional coiling, patients with DWI lesions were encountered in 10–71% of cases.11–14 20–22 Our results were in line with the data of Soeda et al12 (61%) and Lim Fat et al14 (71%). Both studies have sufficient case numbers and describe the occurrence of DWI lesions after conventional coiling of unruptured cerebral aneurysms ranging from 61% to 71%. In contrast, the DWI study of Biondi et al20 demonstrated a considerable lower proportion of patients with DWI lesions (10%) after conventional coiling. However, they evaluated only 20 patients with ruptured and unruptured aneurysms. In another approach applying microembolic signal monitoring, Schubert et al23 compared the rate of embolic events in patients treated with stent-assisted coiling versus those treated with coiling alone. The authors observed no significant difference between the two procedures. These results support our findings that stent-assisted coiling does not seem to be associated with an increased risk of sustaining embolic events compared with coiling alone. This is a surprising result since stent-assisted coiling involves increased technical complexity.
Another issue investigated in our study was the size of the DWI lesions. In the majority of cases (87.1%) DWI lesions were of small size (<5 mm in diameter). However, three of our patients had large DWI lesions with a diameter >15 mm.
Concerning the distribution of the DWI lesions, in four patients (8.3%) the lesions were not located in the vascular territory of the treated artery. Retrospectively, we reviewed the MR angiograms of these four patients and found that their vascular anatomy did not allow for any collateral flows. We therefore assume that these DWI lesions originated from diagnostic angiography before stent-assisted coiling. Accordingly, Bendszus et al8 reported an occurrence of DWI lesions in diagnostic angiography in 26% of their cases.
In order to reduce embolic events and to minimize the risk of bleeding, the efficacy of peri- and post-procedural anticoagulation and antiplatelet regimes is still a subject of controversy.14 ,23–29 In contrast to studies demonstrating the anticoagulation effect of heparin during coiling of cerebral aneurysms,14 ,23 ,26 ,27 we found no significant difference in the incidence of DWI lesions in patients with and those without heparinization. Since recent studies on humans lack a control group of patients without heparin treatment,14 ,23 ,26 ,27 no definite statement is possible about the appropriate anticoagulation regime. Notably, a swine model showed the effect of systemic heparinization on the in vivo thrombogenicity of various micro- and guiding catheters.30 The catheters demonstrated an increased debris accumulation without systemic heparinization using scanning electron microscopy. For this reason, we consider that further studies are needed to adequately measure the effect of heparin treatment.
Finally, we analyzed the amount of ischemic brain tissue in each patient after the stent-assisted coiling procedure. Bearing in mind the differences in brain volumes in general, determination of lesion volumes might allow a better quantitative comparison of the dimension of damaged brain. Besides number and size, the location of a DWI lesion is the key factor leading to a neurologic deficit. Our analysis revealed that older patients (≥55 years) had significantly higher ischemic lesion volumes, which confirms that patient age is a risk factor for DWI lesions.
Interestingly, although a previous study of periprocedural complications during carotid artery stenting reported a higher incidence of DWI lesions with increasing stent length,31 this trend was not found in our series. In contrast, we found higher amounts of ischemic brain volumes in patients with shorter stents (<20 mm). However, it has to be considered that stents were placed in completely different locations—intracranially in our study and extracranially in the study by Gröschel et al.31 For instance, the extracranial part of an internal carotid artery frequently shows another quality of atherosclerotic plaques (eg, grade of calcification, diameter of plaques) compared with intracranial parts of the same artery. A possible explanation for the higher ischemic brain volumes in patients with shorter stents might be the insertion of shorter stents in more complex and risk-associated artery areas. Another explanation might be a longer stenting procedure due to the need for better targeting of shorter stents. However, the reason for the effect could not be explained by the data.
Study limitations
While we believe that the results of our study have significant value, the study has several limitations. Based on its retrospective nature, there was no standardized protocol for the periprocedural anticoagulation regime and antiplatelet therapy. Another limitation of the study is the lack of acquisition of a pretreatment DWI sequence, so we cannot completely eliminate the possibility that some of the DWI lesions may have been due to other causes including pre-procedural diagnostic angiography. Additionally, the acquisition of DWI sequences in 1.5 T and 3 T magnets is not homogeneous and is not completely comparable to most of the primary coiling DWI studies which were performed on 1.5 T magnets. It should also be mentioned that, as described in the literature,32 the use of different stent types greatly impacts the periprocedural complication rate because of different safety profiles. Furthermore, the Neuroform stent has undergone several modifications during the time of the study.
Conclusion
Our study found a relatively high incidence of DWI lesions after stent-assisted coiling. However, despite several devices and low operator experience, stent-assisted coiling for intracranial aneurysms has a very low risk of permanent neurologic disability and does not to lead to more lesions than coiling alone. Risk factors for ischemic lesions are age of the patient and a long procedure time. Further studies should focus on the relationship between grade of arteriosclerosis and the risk of cerebral embolization. Based on these data, augmented algorithms for patients in conditions with increased risk potential should be developed to prevent potentially neurologic complications.
References
Footnotes
-
MLH and AR contributed equally.
-
Contributors All authors gave final approval of the submitted manuscript. MLH, AR and MS: data collection, data analysis, manuscript preparation and writing. IW, SG and CM: study design, technical help and proofreading. MF, IES and US: general support and proofreading.
-
Competing interests The Institute of Diagnostic and Interventional Radiology and Neuroradiology, University Hospital of Essen, Germany, acknowledges financial support for furthering research and education in interventional neuroradiology through institutional grant support from Boston Scientific/Stryker.
-
Provenance and peer review Not commissioned; externally peer reviewed.