Article Text

Abstract
Introduction Outcome studies in acute ischemic stroke (AIS) have focused on time from symptom onset to treatment. The purpose of this study was to investigate whether time to achieve vessel recanalization from groin puncture affects outcomes.
Methods We studied all AIS cases that underwent intra-arterial therapy between May 2008 and October 2012 at a high volume center for anterior circulation occlusions. Candidacy for thrombectomy is determined by CT perfusion imaging, irrespective of time of onset. Patients were then dichotomized into two groups: ‘Early recan’ assigned in which recanalization was achieved in ≤60 min from groin puncture and ‘Delayed recan’ in which procedures extended beyond 60 min. Time to recanalize was also studied as a continuous variable.
Results 159 patients (53.5% women, mean age 66.4±15.2 years) were identified. The mean National Institutes of Health Stroke Scale (NIHSS) score was similar between ‘Early recan’ patients (16.8±6.1) compared with ‘Delayed recan’ patients (15.4±5.8, p=0.149). Among the ‘Early recan’ patients, recanalization was achieved in 40.7±13.6 min compared with 101.7±32.5 min in the ‘Delayed recan’ patients (p<0.0001). The likelihood of achieving a good outcome (modified Rankin Scale score 0–2) was higher in the ‘Early recan’ group (53.6%) compared with the ‘Late recan’ group (30.8%; p=0.009). On logistic regression analysis, time to recanalization from groin puncture, baseline NIHSS, revascularization, diabetes, and hemorrhages were found to significantly impact on outcome at 90 days, as measured by the modified Rankin Scale.
Conclusions Our findings suggest that extending mechanical thrombectomy procedure times beyond 60 min increases complications and device cost rates while worsening outcomes. These findings can serve as a time frame of when it is prudent to abort a failed thrombectomy case.
- Thrombectomy
- Stroke
Statistics from Altmetric.com
Introduction
Ischemic stroke is the third leading cause of death, and accounts for one out of every 17 deaths in the USA. It is the leading cause of long term disability in the USA, with an estimated cost of US$68.9 billion in 2009.1 Treatments for ischemic stroke have rapidly evolved over the past decade and include administration of systemic intravenous tissue plasminogen activator (IV tPA) as well as intra-arterial (IA) thrombolysis and mechanical thrombectomy.2–,4 While the administration of IV tPA remains the gold standard, IA therapy continues to have a role.5–,11 For those patients who qualify for endovascular intervention, there are a variety of treatment options. Balloon angioplasty, IA thrombolysis, stenting, aspiration, and mechanical maceration are some of the techniques currently available, with novel therapies continually emerging.3 ,4 ,12–15
By convention, outcome studies assessing treatment success following acute ischemic stroke (AIS) have focused on time from symptom onset. However, recent evidence suggests that patients can be safely and effectively selected for IA therapy with perfusion imaging, irrespective of time of onset.16 Additionally, there is increasing evidence to suggest that the faster reperfusion is achieved, the more brain tissue is preserved.17 The purpose of this study was to review a single institution's experience with IA therapy for AIS and investigate whether time to achieve vessel recanalization, from groin puncture rather than symptom onset, had an effect on recanalization status, intraprocedural complications, and functional outcomes.
Methods
We retrospectively studied a prospectively maintained database of cases of AIS involving the anterior circulation that underwent IA therapy between May 2008 and October 2012 at a tertiary care center (Medical University of South Carolina). The study was approved by the institutional review board of the Medical University of South Carolina. At our institution, mechanical thrombectomy is the preferred treatment modality for AIS. Candidacy for intervention is determined by CT perfusion imaging, irrespective of time of onset. Cerebral blood flow was compared with cerebral blood volume. Patients with mismatches corresponding to regions of penumbra that could account for significant contributions to their presenting National Institutes of Health Stroke Scale (NIHSS) score were considered candidates for intervention following a discussion between the attending neurointerventionalist and stroke neurologist.
Patients who receive IV tPA are also candidates for mechanical thrombectomy. During the study period, the primary device for mechanical thrombectomy utilized was either the Penumbra aspiration system (Penumbra Inc, Alameda, California, USA) or newer generation ‘stent retrievers’, such as the Solitaire device (ev3 Endovascular Inc, Plymouth, Minnesota, USA), Trevo Pro (Stryker Neurovascular, Kalamazoo, Michigan, USA), or Penumbra 3D separator (Penumbra Inc).18
Patient charts, procedural records, and angiograms were reviewed. Data were extracted on age, gender, initial NIHSS score, time of symptom onset, whether IV tPA was given, whether IA thrombolytics were administered, the intracranial vessel affected, Alberta Stroke Program Early CT (ASPECT) score, recanalization status of the affected vessel, as determined by the Thrombolysis in Cerebral Ischemia (TICI) scale, intraprocedural complications, time to recanalization, and the presence of hemorrhage on postprocedure head CT scan. Every patient underwent a postprocedure CT within 12–24 h routinely and the presence of hemorrhage on CT was determined by a blinded neuroradiologist. In cases where there was question of contrast staining versus petechial hemorrhage, subsequent CTs were reviewed to assess for washout of contrast. If the follow-up imaging did not clarify contrast staining versus petechial hemorrhage, petechial hemorrhage was assumed. Functional outcome was assessed by 90 day follow-up modified Rankin Scale (mRS). Patients were then dichotomized into two groups: ‘Early recan’ assigned for those in which recanalization was achieved in ≤60 min and ‘Delayed recan’ for those in which procedures and recanalizations extended beyond 60 min. For portions of the statistical analysis, time to recanalize was studied as a continuous variable.
Time to vessel recanalization was determined from percutaneous groin access (time zero) to the time that the affected vessel was recanalized. Time was monitored in minutes and seconds based on review of the time stamp of the angiographic images. If the patient suffered an intraprocedural complication requiring abortion of the procedure (eg, vessel rupture), recanalization time was defined as the time of groin puncture to the time when the complication was documented on the angiographic run, not the final procedural time.
Statistical analysis
Statistical analyses were performed using SAS V.9.2 (SAS Institute, Cary, North Carolina, USA). A population of 159 subjects was analyzed using descriptive statistics to characterize demographics and other clinical variables describing treatment, complications, and outcomes. Differences between the recanalization time groups (procedure lasting up to 60 min vs more than 60 min) based on these variables were tested using the Student’s t test for continuous measures and a χ2 test for categorical measures. Differences between the device groups were tested using Fisher's exact test for categorical measures with expected cell sizes <5. All tests were two sided and assessed at a significance level of 0.05. Multivariate logistic regression was used to predict the outcome mRS score at 90 days of 0–2 based on several prespecified prognostic variables, including time to recanalization. Model performance was assessed using the Hosmer–Lemeshow test and the c statistic.
A logistic regression analysis was performed on 143 out of the 159 subjects in the cohort to determine if the probability of a good outcome at 90 days was affected by prespecified prognostic variables. A good outcome was defined as a score of 0, 1, or 2 on the mRS completed at 90 days. There were 57 subjects (39.9%) with a good outcome included in the model. There were 12 subjects with a missing outcome and four subjects with missing values for a prognostic variable that were excluded from the model. The variables included in the multivariate model were recanalization time in minutes, baseline NIHSS score, revascularization (post-TICI flow of 2B or 3), the presence hemorrhages or procedural complications, time from symptom onset to CT in hours, time from CT to procedure start in hours, treatment with IA or IV TPA, age, and indicators of atrial fibrillation, diabetes, hypertension, and general anesthesia. There were no significant interactions in the model and it had a c statistic of 0.82.
Results
Patient baseline characteristics
A total of 159 patients (53.5% women, mean age 66.4±15.2 years) underwent IA therapy for AIS during the study period (table 1). Patients presented with an average NIHSS score of 15.9±5.9 and were treated 9.2±8.3 h from symptom onset on average. The mean NIHSS score was similar between ‘Early recan’ (16.8±6.1) and ‘Delayed recan’ (15.4±5.8, p=0.149) patients. Average age was similar between the two groups and both groups were also similar in the rates of preprocedural IV tPA administered and time from symptom onset to groin puncture. Patients in whom an ‘Early recan’ was achieved were more likely (50.0% vs 20%; p<0.0001) to have a history of atrial fibrillation. A significant difference was identified in time from initial image acquisition (noncontrast CT) to procedure start (1.8±1.3 vs 1.4±0.7 h; p=0.019).
Patient characteristics
Recanalization
Overall, mean time for recanalization was 79.0±40.0 min and IA tPA was administered at a similar frequency in the two groups. Among the ‘Early recan’ patients, recanalization was achieved in 40.7±13.6 min compared with 101.7±32.5 min in the ‘Delayed recan’ patients (p<0.0001). Among all patients, TICI 3 was achieved in 31.5% (n=50) and 2B in 47.2% (n=75). Thus a TICI score of 2B or greater was achieved in 78.6% (n=125) of patients. Patients in the ‘Early recan’ group were more than twice as likely to achieve a TICI 3 (49.2% vs 21%; p=0.002) and a TICI of 2B or 3 (89.8% vs 72%; p=0.009) compared with the ‘Delayed recan’ group. In addition, more devices were utilized in the ‘Delayed recan’ group, resulting in a higher material cost per procedure ($12, 824.89±7217.02 compared with $10, 311.58±3821.08; p=0.005).
Procedural events
The two recanalization groups underwent general endotracheal anesthesia at similar rates (overall rate 93.1%). The overall procedural complication rate was 8.2%. Ten patients had arterial dissections, three of which underwent acute intraprocedural stenting, and one underwent stenting as a separate procedure at a later date. All three cases had follow-up mRS scores of 0 at 90 days, and two of three had recanalization times of more than 1 h. Three patients had arterial perforation and three required intraprocedural balloon occlusion which resolved the perforation. The complication rate was higher among the ‘Delayed recan’ patients (11%) compared with the ‘Early recan’ patients (3.4%; p=0.05).
The overall rate of hemorrhage on postprocedure CT was 19.5% (n=31), which was not significantly different between the two groups based on time to recanalization. No differences between the two groups were identified when hemorrhage on CT was further stratified according to subtype (intracerebral hematoma, intraventricular hemorrhage, subarachnoid hemorrhage, and petechial hemorrhage).
Neurologic outcomes
Ninety day mRS was available for 147 of the patients (92.5%) at the time of data interpretation. Overall, 58 patients (39.5%) achieved an mRS score of 0–2 at 90 days. The likelihood of achieving a good outcome (mRS 0–2) was higher in the ‘Early recan’ group (53.6%) compared with the ‘Late recan’ group (30.8%; p=0.009). The likelihood of patients being either dead or in a persistent vegetative state (mRS 5–6) was significantly higher in the ‘Late recan’ group (31.9% vs 14.3%; p=0.019) (figure 1).

Distribution of 90 day outcome, as determined by the modified Rankin Scale (mRS), comparing the ‘Early recan’ patients (recanalization times achieved in ≤60 min) to the ‘Delayed recan’ patients (recanalization times extended beyond 60 min). ‘Early recan’ patients were significantly more likely to achieve an mRS score of 0 or 0–2 while ‘Delayed recan’ patients were more likely to achieve an mRS score of 5–6.
Factors impacting on outcome
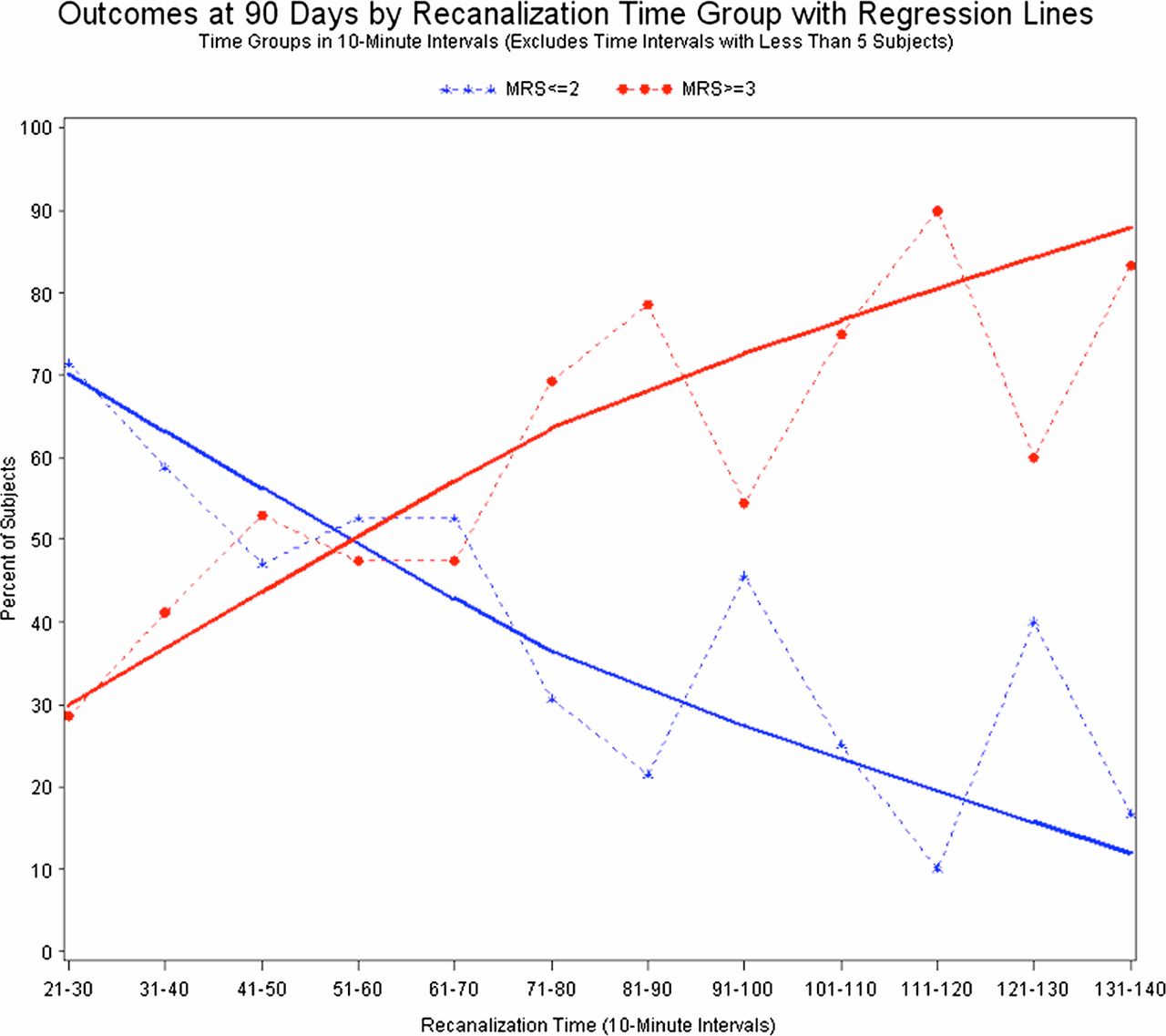
On logistic regression analysis, recanalization time, baseline NIHSS, revascularization, diabetes, and hemorrhages were found to significantly impact on mRS outcome at 90 days (table 2). Subjects with higher recanalization times were less likely to achieve an mRS ≤2 at 90 days. For each 10 min increase in recanalization time, subjects were 0.87 times as likely to have a good outcome after controlling for other variables (figure 2). A higher NIHSS score at baseline and incurring a hemorrhage also decreased the likelihood of a good outcome, with ORs of 0.88 and 0.27, respectively. Subjects achieving revascularization (2B or 3) were 3.45 times as likely to achieve a good outcome at 90 days. Subjects with diabetes had a decreased likelihood of a good outcome, with an OR of 0.27. On multivariable analysis, patients in whom no core infarct was identified on CT perfusion imaging (ASPECT score 10), there was a stronger association between TICI 2B or greater recanalization and favorable outcome (p=0.008).
Results of both univariate and multivariate logistic regression analysis of parameters and outcome at 90 days

{kind=link}
{kind=link}
Likelihood of achieving a ‘Good’ (modified Rankin Scale (mRS) score of 0–2) versus ‘Poor’ (mRS 3–6) outcome at 90 days as a function of procedural time.
Discussion
Mechanical thrombectomy devices have improved over the past 5 years, allowing disruption and removal of acute occlusions for reperfusion of an ischemic penumbra. Anecdotally, we have observed that employing the best available thrombectomy devices, recanalizations are often achieved with the first few attempts at thrombectomy, while the likelihood of achieving a safe recanalization decreases with increasing attempts. Thus recanalization is likely to occur relatively quickly, or not at all. This has been demonstrated specifically with the Merci retrieval system (Concentric Medical, Mountain View, California, USA), although utilization of this device has since decreased with the introduction of newer generation thrombectomy devices.16 This challenge reflects our relatively poor understanding of the underlying acute clot morphology. Furthermore, this raises the possibility that increasing number and more aggressive attempts to achieve mechanical thrombectomy may result in higher complication rates. It is for these reasons that we tested the hypothesis that longer procedure times may affect outcomes.
This is the first study to directly investigate the procedural time required to recanalize an acutely occluded vessel, not the time from symptom onset, with functional outcomes. Traditionally, studies assessing outcome following AIS and thrombectomy success have focused on whether or not recanalization was achieved with the only time variable considered being time from symptom onset to either mobilization of the neurointerventional team or vessel recanalization. However, there is an increasing awareness that due to inherent variability in collateral support and vascular reserve, each patient presenting with AIS likely has a unique ‘time window’ for treatment. For this reason, we utilize CT perfusion imaging to determine candidacy for IA therapy, regardless of time from symptom onset.19 Thus every patient undergoing groin puncture for attempted mechanical thrombectomy has an image verified region of penumbra. In this manner, every patient, regardless of time from symptom onset, is at the same starting point at the beginning of the procedure.
We found that longer procedure times are associated with a lower likelihood of achieving recanalization (TICI 2B or 3), significantly higher device costs, and intraprocedural complications. Importantly, these differences translate into poorer outcomes at 90 day follow-up. Patients in whom procedures lasted >60 min had a significantly higher likelihood of being dead or in a persistent vegetative state, while patients in whom recanalization was achieved in <60 min were more likely to have an mRS score of 0–2. These findings corroborate those of Hassan et al.20 In fact, after accounting for clinical factors, each 10 min increment in procedural time negatively impacted on the likelihood of achieving a good long term outcome in our experience. These findings are likely multifactorial. Increasing procedure time will further tax compensatory collaterals supplying an ischemic penumbra and further push that region towards irreversible injury. In other words, there is diminishing return of successful recanalization with longer procedure times due to progression of ischemia. While patients in the ‘Early recan’ group and ‘Delayed recan’ group had similar times from symptom onset to procedure start (groin stick), the ‘Early recan’ patients had lower times from the start of CT acquisition to groin puncture than the ‘Delayed recan’ group. This difference likely contributes to the disparity in functional outcomes, as patients may have progressed from penumbra to infarction prior to recanalization, regardless of recanalization time.21 However, neither time from symptom onset to groin puncture nor time from CT to groin puncture was found to be a predictor of outcome on both univariate and multivariate analysis.
Strengths of this study include the relatively large number of patients enrolled from a single institution with a relative homogenous approach to treatment over a relatively short time period. This minimizes procedural variability and postoperative patient care that could impact on patient outcomes. Recent data indicate that higher volume stroke centers are more efficient at delivering appropriate patients to the angio suite, reflected in shorter imaging to recanalization times, higher rates of recanalization, and more favorable outcomes.22 Limitations of this study include the retrospective nature of the study, although the data were obtained from a prospectively maintained database. Final TICI scores were determined by the primary operator and mRS was determined by the treating stroke neurologist at 90 days, neither of which were blinded to the procedure and which could represent a source of bias. Another limitation is that patients who were considered for IA thrombectomy but were excluded based on CT perfusion criteria were not tracked, also representing another selection bias. Also, increased operator proficiency over time would be expected with a particular thrombectomy device although this is difficult to quantify and account for.
This study further demonstrates that technical factors specifically related to the thrombectomy procedure itself also largely impact on long term outcome. This finding is important because it provides a potential endpoint for a thrombectomy case. As our data demonstrate, between 60 and 70 min of procedural time, there is a negative balance for further efforts—that is, further attempts at achieving recanalization, despite our best intentions, are more likely to cause harm than good. For our own practice, while clinical judgment by the operator at the time of the procedure will ultimately determine whether or not the case should be continued, this general time frame now factors into the decision making process.
Conclusion
Mechanical thrombectomy has a role in AIS. Our data suggest that extending procedure times beyond 60–70 min increases complications and cost while diminishing the likelihood of good outcomes. These findings can serve as a time frame of when it is prudent to abort a failed thrombectomy case.
References
Footnotes
-
Contributors Each author listed should receive authorship credit based on the material contribution to this article, their revision of this article, and their final approval of this article for submission to this journal.
-
Competing interests None.
-
Ethics approval The study was approved by the institutional review board of the Medical University of South Carolina.
-
Provenance and peer review Not commissioned; externally peer reviewed.