Article Text

Abstract
Background and purpose The use of Onyx has become the mainstream for the treatment of cranial dural arteriovenous fistulas (AVFs) and arteriovenous malformations, but the reported success for type I spinal dural arteriovenous fistulas (sDAVFs) remains limited. We review our experience with Onyx and report its limitations in the treatment of spinal AVFs.
Materials and methods We retrospectively reviewed the Interventional Neuroradiology Procedure database at Washington University for cases of sDAVF embolization. Radiology reports were reviewed for fistula classification, treatment technique, and initial and follow-up results. Angiographic images were reviewed to confirm diagnosis, treatment, and penetration of embolisate into the draining vein.
Results With the use of Onyx, sDAVFs were obliterated in six of seven patients at the time of treatment. Follow-up angiography confirmed sDAVF obliteration in two patients, and recurrence in two cases. Two patients had no follow-up. One patient not cured at the time of treatment was treated surgically. Of the nine total treatments, Onyx successfully crossed the nidus into the draining vein in only four cases. Successful venous embolization was facilitated with positioning of the microcatheter to less than 5 mm from the nidus in three of the four cases. The use of n-butyl cyanoacrylate (NBCA) resulted in venous penetration in eight of 10 cases, and short term follow-up cure in seven of 10 patients.
Conclusions Our experience with Onyx for type I sDAVF embolization has been tempered by difficulty in achieving venous penetration and, consequently, a high rate of recurrence. For management of these fistulas, we favor NBCA or surgical treatment.
- Fistula
- Embolic
- Spine
- Vein
- Catheter
Statistics from Altmetric.com
Introduction
The addition of Onyx (Covidien, Mansfield, Massachusetts, USA) has greatly improved the interventional treatment of many vascular lesions. The successful use of Onyx in the transarterial embolization of cranial dural arteriovenous fistulas (cDAVFs) with cortical venous drainage treatment has been reported extensively with good results.1–5 As a result, Onyx has become the agent of choice over n-butyl cyanoacrylate (NBCA) (Codman Neuro, Raynham, Massachusetts, USA) in the interventional treatment of cranial arteriovenous fistulas (AVFs).6
The most common type of spinal dural arteriovenous fistula (sDAVF) is the type I AVF with the arterial supply along the dural root sleeve.7 ,8 This fistula, as described by Spetzler et al, is composed of a radicular feeding artery that communicates with an intradural dorsal vein at the dural sleeve.7 ,8 Treatment of these lesions with NBCA has been reported in multiple series, with cure rates of 70–90%.9–11 Although there has been wide adoption of Onyx for cDAVF, reports for its use in treating spinal AVFs is limited to only a few cases.12–14
In this report, we review our own experience with Onyx 18 and NBCA for the treatment of type I spinal AVFs. The specific purpose was to review the technical aspects of Onyx embolization and evaluate venous penetration and AVF recurrence relative to our experience with NBCA.
Methods
Following institutional review board approval, we retrospectively reviewed the Interventional Neuroradiology Procedure database at Washington University from 2006 (our first use of Onyx) to 2011 to identify all treated spinal AVFs. Individual charts were reviewed to determine the type of malformation treated and embolisate used.
Embolization was performed with Onyx 18 or NBCA. In all Onyx cases, an attempt was made to persuade penetration of material into the draining vein using the standard technique of injection followed by up to 2 min of pause to allow formation of a kernel at the catheter tip and redirection of Onyx. Embolization was terminated if there was successful venous penetration or if significant reflux along the microcatheter prohibited additional embolization. Onyx 34 was not used in any case due to its higher viscosity.
Post embolization angiography was performed at the time of the procedure in all cases. This was performed at the level of embolization as well as levels above and below embolization. Images were reviewed in addition to the reports for definitive assessment of venous penetration.
We routinely perform delayed follow-up angiography for all spinal embolizations to confirm continued fistula occlusion. Follow-up angiography images were compared with pretreatment and post treatment images.
Results
From 2006 to 2011, a total of 20 patients with sDAVFs were treated via endovascular embolization. Seven patients were treated with Onyx 18 and 13 with NBCA.
There were a total of nine treatments in the seven Onyx patients, all of whom had a type I spinal AVF. An Echelon 10 microcatheter (Covidien) was used in eight treatments and a Marathon microcatheter (Covidien) was used in one case.
Of the 13 patients treated with NBCA, 10 had a type I sDAVF. All were embolized via a single pedicle in a single injection. In seven patients a ratio of 1:5 NBCA and ethiodized oil (Guerbet, France) was used, and in three patients a 1:4 ratio was used.
Treatment 1 and outcome—Onyx group
Seven patients were treated with Onyx 18 for a type I spinal AVF. Six of seven patients demonstrated angiographic cure at the time of treatment. The one patient without angiographic cure at the time of the procedure was treated with a surgical ligation (table 1, patient No 5).
Patients treated with Onyx
Follow-up angiography was available in four patients. Only two patients were cured with a single treatment at follow-up angiography (patient Nos 1 and 2). Two patients had recurrence of their AVF.
Two patients had no follow-up angiography after treatment and could not be reached to schedule follow-up imaging. Both patients showed AVF obliteration at the time of treatment.
Treatment 2 and outcome—Onyx group
Patient Nos 3 and 4 showed angiographic recurrence at 1 month and 2 years, respectively (Figure 1). They subsequently underwent repeat treatment. Both patients were cured at the time of retreatment. Patient No 3 had a 2 month follow-up angiogram showing stable obliteration. Patient No 4 had no follow-up angiography.
Venous penetration and outcome—Onyx group
Of seven initial treatments, only three cases had definitive venous penetration. Including retreatments, nine procedures were performed in seven patients. In four of nine procedures, venous penetration was achieved.
One patient without venous penetration had no recurrence at the 2 month follow-up. Of the three patients with initial treatments indicating venous embolization, one demonstrated no recurrence at follow-up (patient No 2) while two recurred (patient Nos 3 and 4). In both cases the amount of venous embolisate was minimal, with only a few millimeters of cast formed in the vein.
Two patients underwent a second treatment for recurrent fistulae (patient Nos 3 and 4). Patient No 3 was retreated but there was no venous penetration of Onyx. The AVF was cured at the time of treatment and at the 2 month follow-up. Patient No 4 was retreated after a delayed recurrence at 2 years. There was successful venous embolization and cure during the second treatment without follow-up.
Microcatheter position during embolization was less than 1 cm from the nidus in four cases. When the catheter was positioned less than 1 cm from the nidus, venous embolism was achieved in three of four cases (Figure 2). With the microcatheter positioned greater than 1 cm away from the nidus, venous embolization could be achieved in only one of five cases.
NBCA treatment results
Ten patients were treated with NBCA for type I sDAVF. In eight of 10 patients, there was successful delivery of NBCA into the proximal draining vein. In these eight patients with venous embolization, follow-up angiography was available in seven patients, ranging from 1 to 10 months (average 3.4 months). One patient had no follow-up angiography although the fistula was obliterated at the time of treatment.
In two of 10 patients, there was no embolisate identified in the draining vein. One patient was taken for surgical ligation as the NBCA also did not make it into the nidus. The second patient had NBCA delivered into the nidus and had no residual filling at the time of treatment. There was no follow-up angiography to evaluate recurrence.
Of 10 patients in total, seven had angiographic follow-up with stable obliteration (average 3.4 months), one proceeded to the operating room for surgical ligation, and two had no follow-up. There were no retreatments.
Discussion
Spinal dural AVFs can be successfully treated with both open surgical and endovascular approaches. Surgical treatment has a high obliteration rate and, because the treatment is directed at the vein, complications are low despite the intradural approach.15 Moreover, surgery affords protection when the segmental feeding artery also supplies a spinal cord artery—a relative contraindication to endovascular treatment.
Nevertheless, endovascular treatment of spinal AVFs remains attractive due to the less invasive nature, avoidance of postoperative pain, and association with a shorter hospital stay.9 Endovascular embolization with NBCA has been effectively used in the treatment of sDAVFs with obliteration rates of around 80%.9 ,11 ,16 However, NBCA is technically difficult to control, and its distal flow is sometimes unpredictable. Embolization beyond the nidus and deep into the draining vein can result in aggravation of venous congestion and neurologic deterioration. Embolization without penetration into the vein can lead to collateralization and recurrence.15
Onyx is a newer permanent embolisate that has the advantage of improved control. Its delivery is over minutes, and its course can be manipulated with a stop and restart technique. Onyx has been shown to be useful in the treatment of cDAVFs but the reported literature in its use for sDAVF is sparse.2 ,3 ,5 ,6 ,17
Several reports have been published on the use of Onyx for treatment of less common spinal malformations. Lanzino et al18 treated seven consecutive patients with extradural spinal arteriovenous malformations and intradural drainage using Onyx 18 or 34. The arteriovenous malformations described were very similar to the traditional type I sDAVFs, although the fistulae were entirely extradural with some drainage to intradural veins. The results were encouraging, and complete occlusion was seen in six patients at the 6 month follow-up (one refused imaging but improved clinically). Successful venous embolization was not specifically addressed.
Rangel-Castilla et al19 evaluated a group of spinal extradural AVFs with and without intradural venous drainage. Patients were treated primarily with Onyx 18 and 34 but two patients were also treated with NBCA. Similar to the results by Lanzino et al, following embolization with Onyx, six of seven AVFs were occluded at follow-up, ranging from 12 to 24 months. The authors do comment that Onyx could not be delivered distally enough in one case, and NBCA was used successfully for obliteration.
Despite the promising results of Onyx in the treatment of uncommon extradural spinal AVFs, data for the more common type I AVFs are limited to five cases. Warakaulle et al reported two type I AVFs treated with Onyx 18.13 In one case there was good venous penetration resulting in cure on follow-up MRI at 7 months but in the second there was no venous penetration, and the fistula recurred angiographically.
In another study, Nogueira et al reported three more patients with type I sDAVFs.12 All three patients were cured with Onyx 18 embolization at a mean follow-up of 12 months. One patient, however, did require two procedures and embolization of three pedicles to achieve angiographic cure.
Successful embolization into the draining vein is particularly important for durable occlusion.16 In this small series, we noted considerable difficulty in achieving satisfactory penetration of Onyx 18 into the venous system. In all nine treatments performed, only four procedures resulted in venous embolization. In none of the cases was there significant (>5 mm) venous penetration, and this may explain our two recurrences even with some minimal venous penetration. Surprisingly, in one case where the microcatheter was positioned 7 mm away from the nidus (patient No 7), we were still unable to achieve a successful venous cast.
When we evaluated microcatheter location in relation to the chance of venous embolization, we found that in three of four instances the microcatheter was less than 1 cm from the nidus. In only one instance did venous embolism occur from a large distance of 1.9 cm. In almost all cases we used an Echelon 10 microcatheter. When we were unable to get close to the nidus, we did not make attempts to use a smaller Onyx compatible microcatheter, such as the Marathon or UltraFlow (Covidien), and this may be a possible improvement in future cases. However, these catheters only accept 0.010 inch wires and are not coil compatible. Unfortunately, due to the small and tortuous nature of these radicular branches, close positioning of the microcatheter is often not possible, regardless of the choice of microcatheter.
Unlike cDAVFs in which Onyx appears distinctly useful, we have found that for spinal type I AVFs, penetration of Onyx into the draining vein is difficult and requires very close positioning of the microcatheter to the nidus. In comparison with Onyx, NBCA was able to penetrate the nidus and draining vein in eight of 10 cases. Although by no means a rigorous comparison, the results for NBCA were slightly better in this small series. An additional consideration is the expense of Onyx which, when the chance for cure is unlikely, should preclude its routine use as surgical treatment offers established durability with low morbidity.
Conclusion
The use of Onyx for the treatment of type I sDAVFs is attractive due to the handling characteristics of the material. However, we have found that successful nidal and venous penetration requires very close positioning of the microcatheter to the nidus. In many cases this cannot be achieved, and Onyx embolization should be discouraged due to its expense and low efficacy. If endovascular treatment is to be performed, we favor the use of NBCA for these sDAVFs.⇓⇓
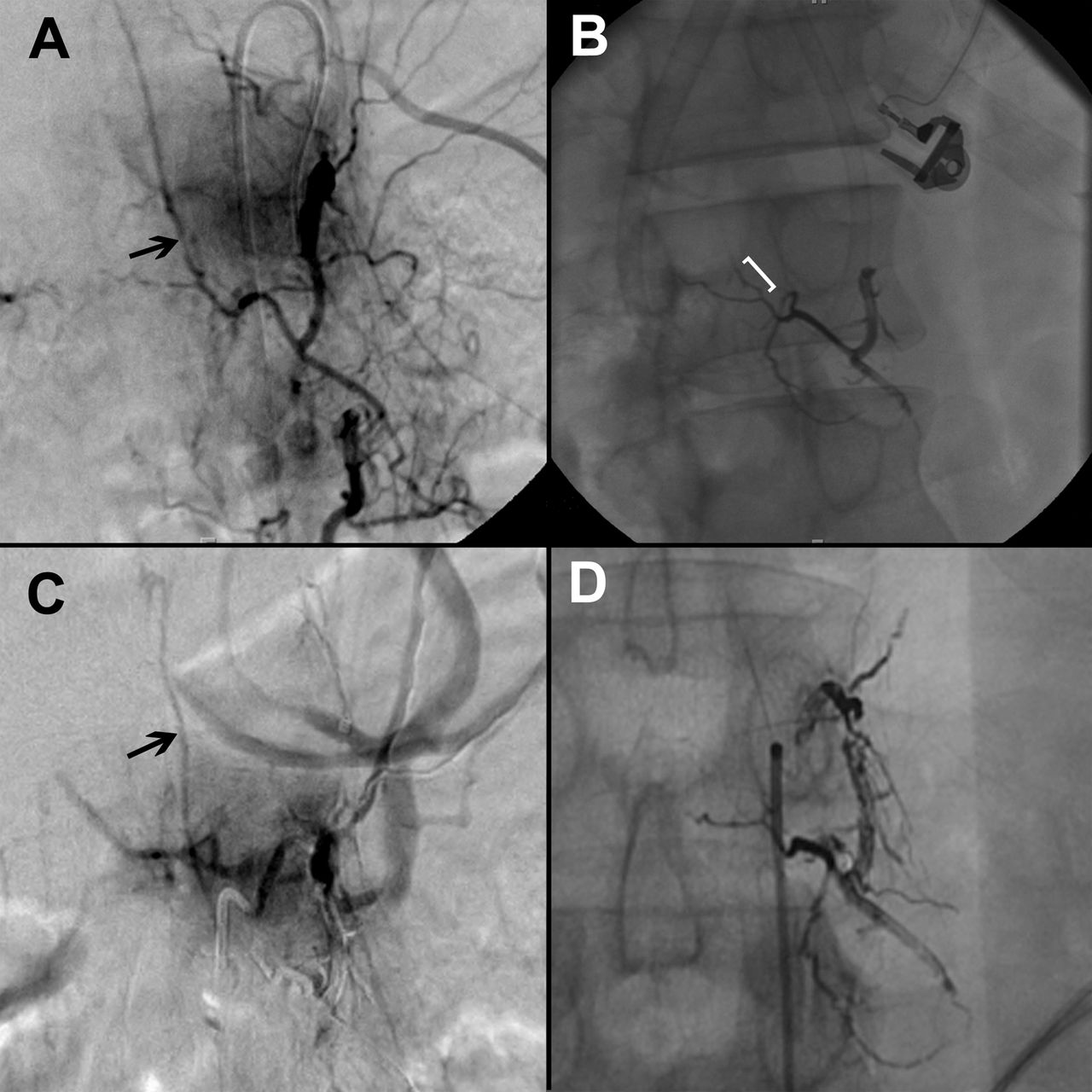
Images for patient 3. A 48 y/o male with myelopathy and bladder dysfunction. (A) Angiography demonstrates a Type I AVF supplied by the Left L1. (B) Onyx cast after embolization. The bracket indicates the small amount of Onyx cast in the proximal vein. (C) Follow-up angiography at 1 month demonstrates a very small feeder from the same level with faint venous filling. (D) This pedicle was embolized more proximally to completely occlude the proximal left L1 pedicle. There was no additional venous penetration, but follow-up angiography at 2 months showed no residual and no collateral supply (image not shown) from adjacent levels.
{kind=link}
{kind=link}
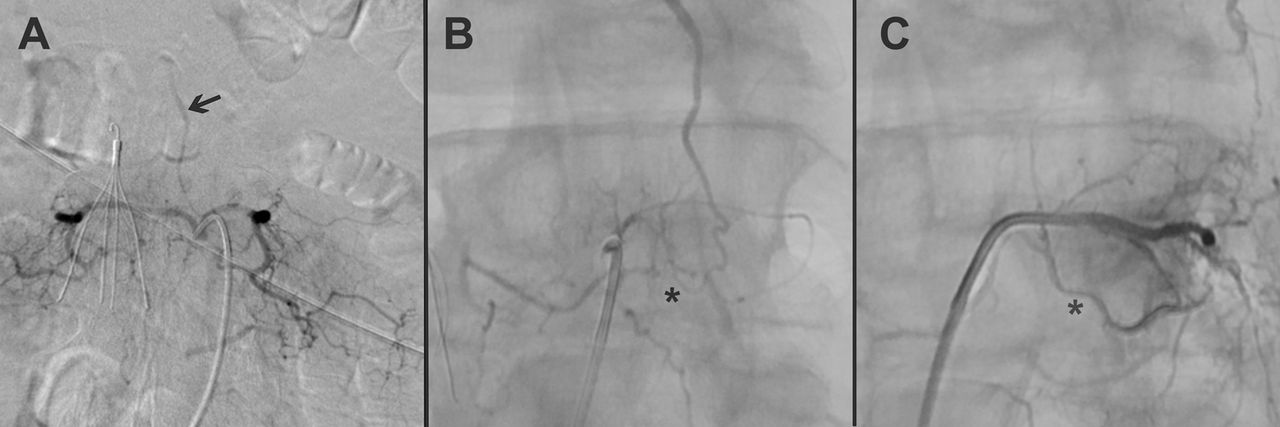
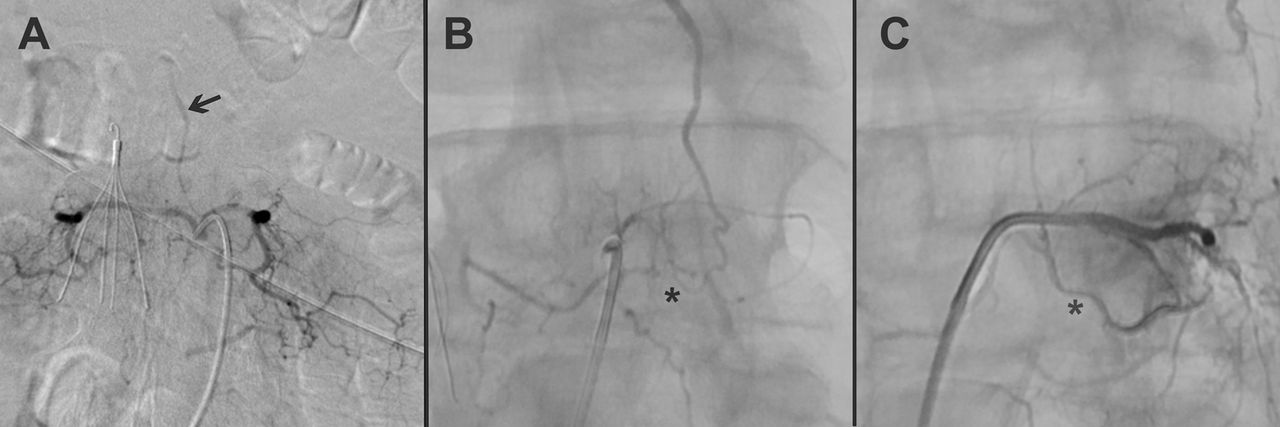
Patient 7. 66 y/o male with a two year history of progressive lower extremity weakness and bladder dysfunction. (A) Spinal angiography demonstrates supply from the left L2 in the guide catheter angiogram from the right and left L2 trunk. (B) microcatheter angiography showing filling of the vein and nidus. The AVF was embolized from this location, 7 mm from the nidal connection (asterisk). (C) Post treatment, the Onyx cast is seen but does not cross the nidus into the draining vein. Asterisk shown to indicate where nidus should be located.
References
Footnotes
-
Contributors SLB was the primary author and data collector. WZR and YK participated in writing portions of this paper, and also performed data collection and radiological image review, and analysis. GJZ, DTC, CJM, and CPD critically edited this paper and the multiple revisions. CPD was the senior author and project coordinator.
-
Competing interests WZR is a consultant for Depuy and Ulrich. CJM is a consultant for Codman and eV3. CPD is a consultant for Gore.
-
Ethics approval The study was approved by Washington University institution review board (IRB approval No 201206078).
-
Provenance and peer review Not commissioned; externally peer reviewed.