Article Text

Abstract
Introduction Endovascular embolization for tumors and vascular malformations has emerged as an important preoperative adjunct prior to resection. We describe the advantages of utilizing a recently released dual lumen balloon catheter for ethylene vinyl alcohol copolymer, also known as Onyx (ev3, Irvine, California, USA), embolization for a variety of head and neck pathologies.
Methods A retrospective review of all cases utilizing the Scepter C balloon catheter (MicroVention Inc, Tustin, California, USA) for use in balloon augmented embolization was performed over a 4 month period from October 2012 to February 2013 at the Medical University of South Carolina, Charleston, South Carolina, USA. Charts and angiographic images were reviewed. Representative cases involving diverse pathologies are summarized and illustrate the observed advantages of balloon augmented Onyx embolization with a dual lumen balloon catheter.
Case illustrations Balloon augmented Onyx embolization utilizing a novel dual lumen balloon catheter was employed to treat both ruptured and unruptured arteriovenous malformations, intracranial dural arteriovenous fistulae, intracranial neoplasms, carotid body tumors, a thyroid mass, and an extracranial arteriovenous fistula.
Conclusions The dual lumen balloon catheter has several advantages for use with Onyx embolization over older devices, including more efficient proximal plug formation and enhanced navigability for placement deep within the pedicles. The balloon augmented Onyx embolization technique represents a valuable tool to add to the armamentarium of the neurointerventionalist to address a variety of head and neck lesions.
- Balloon
Statistics from Altmetric.com
Introduction
Endovascular embolization for tumors and vascular malformations has emerged as an important preoperative adjunct prior to resection. Embolization destroys the blood supply to these lesions, reducing tumor volume and intraoperative blood loss. These advantages may translate into shorter operative times, cleaner surgical bed, and present less risk to the patient. The use of liquid embolisate for vessel sacrifice can be an effective method to achieve embolization in carefully selected cerebrovascular diseases and as part of the pretreatment of neoplastic lesions of the brain and spine.1–4 Unlike coil embolization, the use of a liquid embolic agent presents several unique challenges—namely, retrograde reflux of liquid embolisate that could occlude flow in non-target vessels. The need for such precise delivery of material can necessitate access to distal small caliber arteries to ensure that large, non-target vessels are spared. In order to obviate such complications, the use of balloon catheters has been described as an effective method for creating a proximal plug to prevent reflux of embolisate.5–7
The recently released Scepter C (MicroVention Inc, Tustin, California, USA) dual lumen balloon catheter, originally intended for use in balloon assisted coil embolization of intracranial aneurysms, has been used at our center to assist with embolization of a variety of cerebrovascular and neoplastic lesions. We have previously described our experiences with this device in balloon remodeling, stent delivery for stent assisted coil embolization of cerebral aneurysms, and angioplasty for vasospasm.8–10 We now describe the advantages of utilizing this novel device for ethylene vinyl alcohol copolymer, known as Onyx (ev3, Irvine, California, USA), embolization for a variety of head and neck pathologies.
Methods
A retrospective review of all cases utilizing the Scepter C balloon catheter for use in balloon augmented embolization was performed over a 4 month period from September 2012 to January 2013 at the Medical University of South Carolina, Charleston, South Carolina, USA. Charts and angiographic images were reviewed. Nine related cases are summarized along with indications for embolization, experience using Scepter C, and observed advantages of balloon augmented Onyx embolization (table 1).
Summary of Scepter C balloon augmented Onyx embolization in cerebrovascular and neoplastic lesions
Technique description
All procedures were performed under general endotracheal anesthesia in the neuroangiography suite utilizing transfemoral arterial and/or venous access. Heparin was administered to achieve an activated clotting time of greater than twice the patient's baseline value during the case. A 6 French (Fr) guide catheter was positioned into the proximal vessel of interest, either the internal or external carotid artery, vertebral artery or venous sinus system, and connected to a heparinized flush. The Scepter C balloon catheter was prepared according to the manufacture's recommendation. We utilized 60% dilute contrast for the balloon mix. A 6 Fr guide catheter allows for sufficient deadspace for contrast administration around the balloon catheter for control angiography as well as roadmap creation. Using a 0.014 inch microwire, the balloon catheter was navigated more distally into the relevant vasculature. Intermittent superselective angiography was performed via a hand injection of contrast through the balloon catheter with a 1 mL syringe. This allows for a detailed interrogation of the lesion without vessel overlap which would occur from a more proximal guide catheter injection, obscuring the relevant anatomy.
Under high magnification, contrast injection via the balloon catheter was also performed as required to create detailed working roadmaps for more distal navigation. In some cases, an intermediate catheter, such as a Penumbra reperfusion catheter (Penumbra Inc, Alameda, California, USA), was employed to provide support for more distal navigation of the balloon catheter. Ultimately, the balloon catheter was delivered to the target vessels and the balloon was inflated under fluoroscopic guidance. The balloon catheter's deadspace (0.44 mL) was filled with dimethyl sulfoxide. Onyx was administered for embolization under fluoroscopic guidance until satisfactory penetration and occlusion of target vessels was accomplished.
Case illustrations
Case No 1: transarterial embolization of an unruptured medial frontal arteriovenous malformation
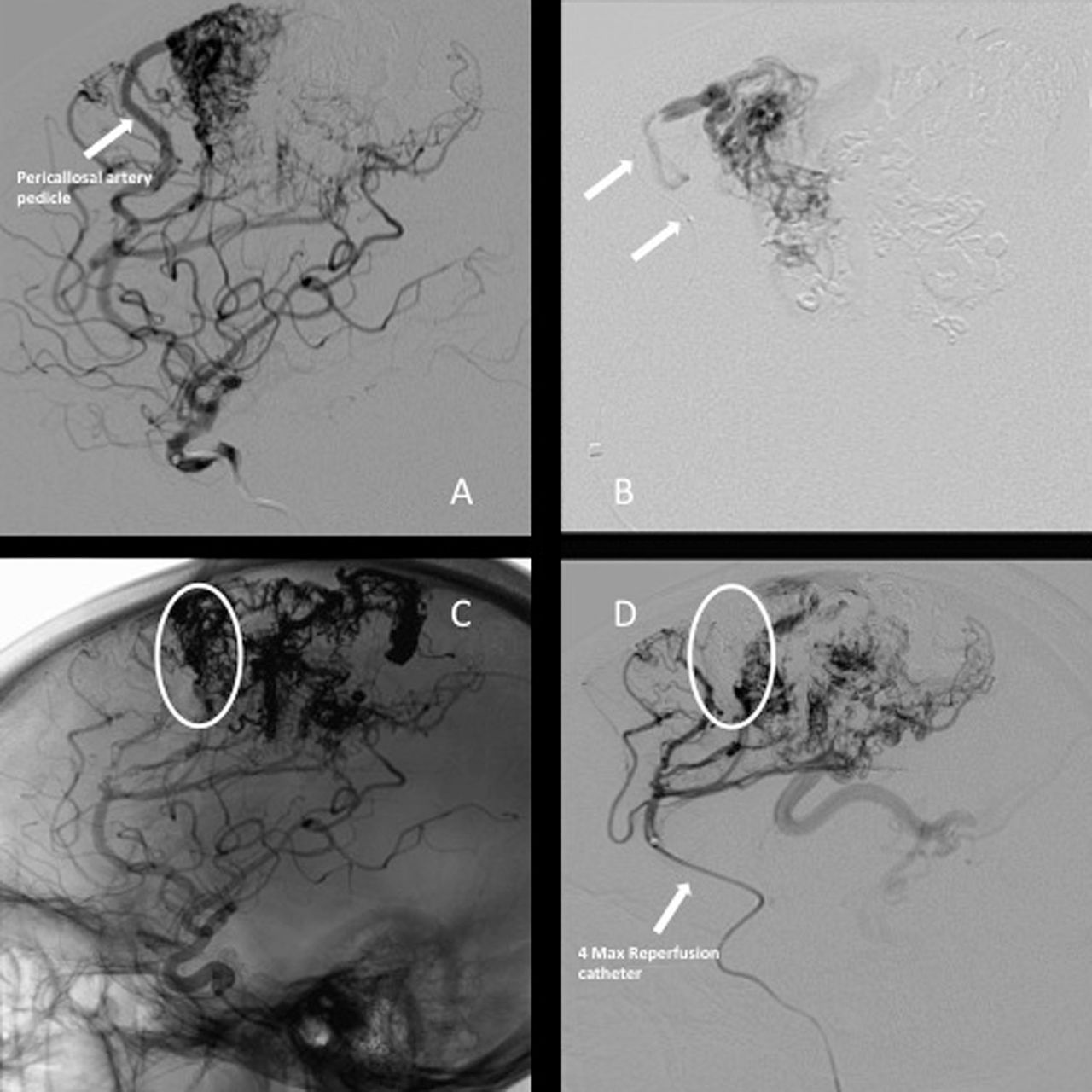
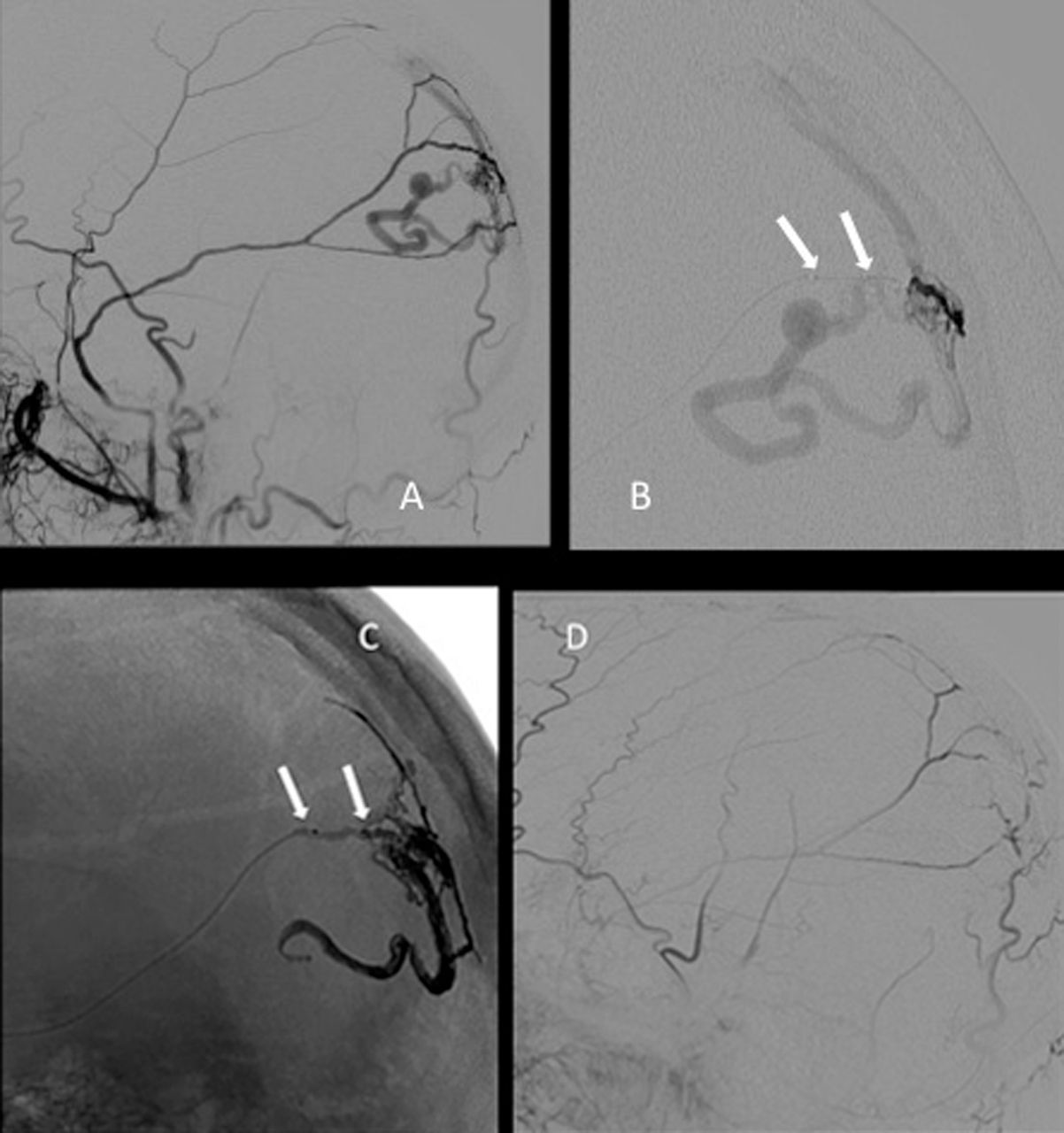
Case No 1 was a 19-year-old patient who previously underwent staged Onyx embolization of a Spetzler Martin grade III arteriovenous malformation (AVM) involving the medial frontal convexity with an arterial supply from the cortical branches of the anterior and middle cerebral arteries in addition to lenticulostriate perforators. Due to concerns of cumulative radiation doses and with the ability of the novel dual lumen balloon catheter, the third stage of embolization was performed with the balloon augmented technique. A 4 Max Penumbra reperfusion catheter (Penumbra Inc) was positioned into the proximal ipsilateral pericallosal artery. A 4.0×10.0 mm Scepter C balloon catheter was navigated over a 0.014 inch Traxcess microwire (MicroVention Inc) into the distal (A4) anterior cerebral artery immediately adjacent to the malformation nidus, and embolization was performed from two pedicle feeders (figure 1). The procedure was uneventful and the patient was discharged home on post-procedure day 2.

Medial frontal convexity arteriovenous malformation (AVM). (A) Pericallosal artery pedicle. (B) Inflated Scepter C balloon catheter (white arrows) superselective angiogram of the pericallosal artery pedicle supplying the AVM. (C) Post-embolization native image demonstrating Onyx cast of the anterior portion of the AVM embolized (white circle). (D) Post-embolization control angiogram with the anterior portion of the AVM no longer opacifying (white circle).
Case No 2: transvenous embolization of a ruptured posterior fossa AVM
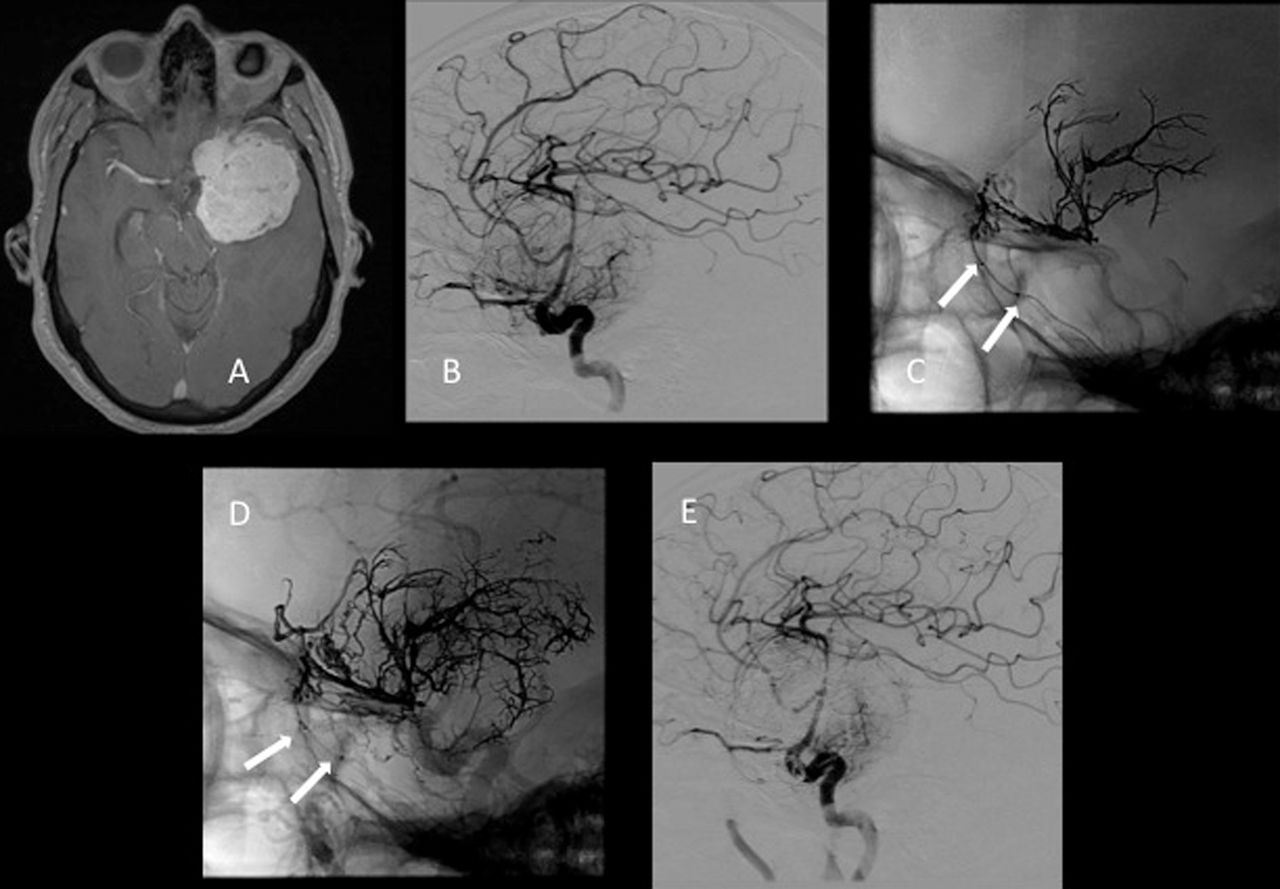
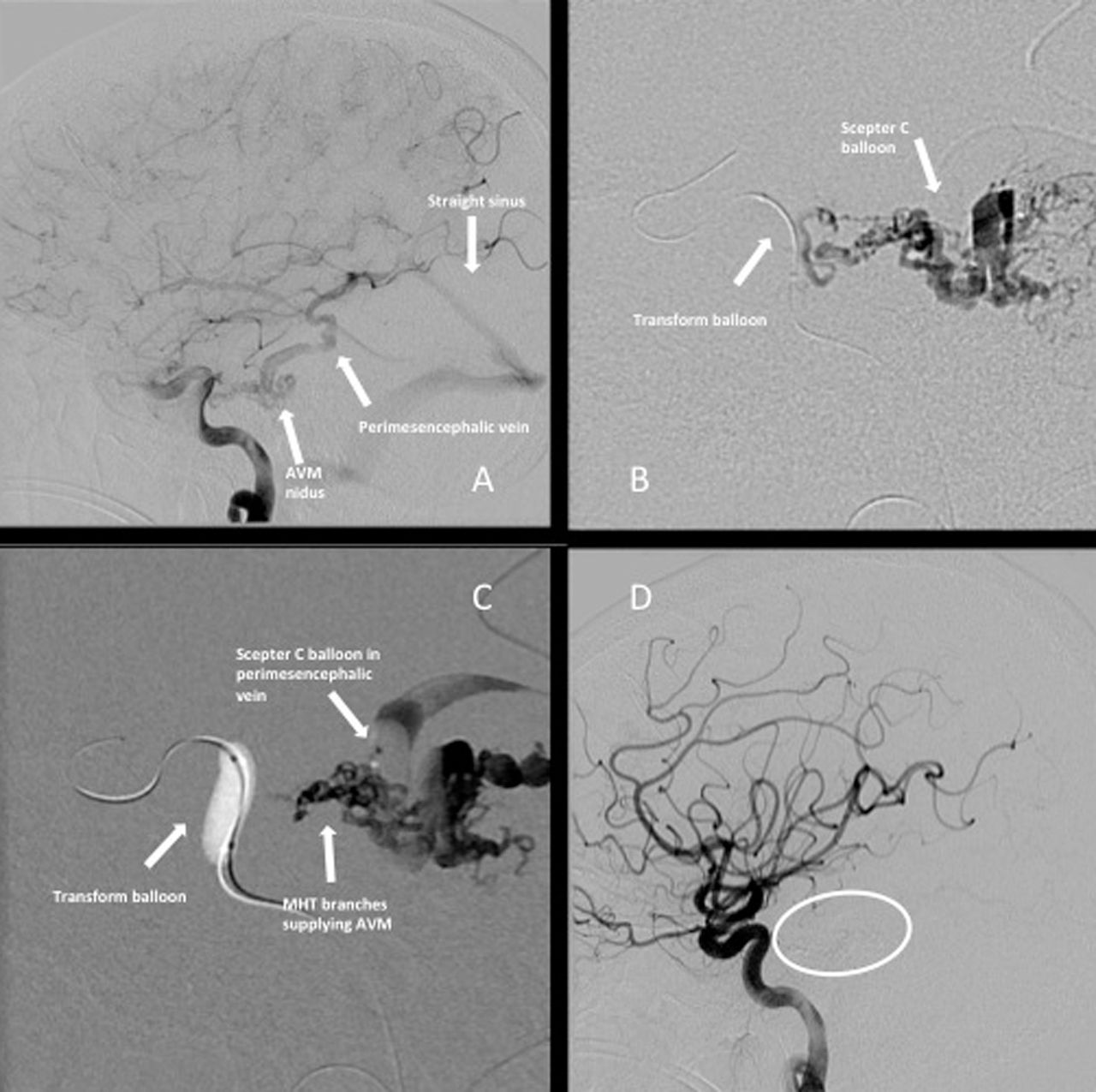
A 45-year-old patient initially presented with a left cerebellopontine angle AVM and underwent gamma knife radiation. The patient represented 18 months later, obtunded, and was found to have a large left-sided cerebellar and pontine hemorrhage with obstructive hydrocephalus. An external ventricular drain was placed and the patient clinically improved to hemiparesis, intermittently following commands over the course of a week. The patient underwent repeat cerebral angiography which demonstrated persistent opacification of the AVM with supply from tiny arterial feeders arising from the meningohypophyseal trunk, with brisk venous drainage into a dilated perimesencephalic vein and subsequently into the straight sinus (figure 2).

Ruptured cerebellopontine angle arteriovenous malformation (AVM). (A) Left internal carotid artery (ICA) angiogram, late arterial phase, demonstrating AVM supply from tiny meningohypophyseal trunk branches with early venous outflow via the dilated perimesencephalic vein. (B) Transvenous approach: inflated Scepter C balloon catheter in the perimesencephalic vein with superselective venogram opacifying the tiny meningohypophyseal trunk branches supplying the AVM and the draining perimesencephalic vein. (C) Negative roadmap image demonstrating a silhouette of the Transform balloon catheter in cavernous segment ICA as a warning for the ICA during embolization; and Onyx embolization with Scepter C balloon catheter into tiny meningohypophyseal trunk branches and draining perimesencephalic vein. (D) Post-embolization control angiogram with AVM no longer opacifying (white circle).
A 6 Fr Neuron 070 guide catheter was advanced over a 5 Fr Select Berenstein catheter (Penumbra Inc) and a 0.038 inch guidewire (MicroVention Inc) to the level of the right transverse sinus. The patient underwent successful balloon augmented Onyx embolization using a 4.0×10.0 mm Scepter C balloon catheter which was advanced through the straight sinus into the perimesencephalic vein to the level of the nidus. Complete angiographic resolution of the malformation was obtained from a single injection at this site. After embolization, the patient remains clinically at his neurological baseline.
Case No 3: transarterial embolization of a dural arteriovenous fistula
A 68-year-old patient was evaluated for headaches and was found to have a Borden I dural arteriovenous fistula in the right posterior parietal convexity with supply from the middle meningeal artery. Venous drainage was to a single cortical vein that drained into the superior sagittal sinus. A 6 Fr Chaperone guide catheter was advanced into the right external carotid artery. A 4.0×10.0 mm Scepter C balloon was advanced over a 0.014 inch Transend EX platinum (Boston Scientific Corp, Natick, Massachusetts, USA) microwire into the middle meningeal artery and navigated immediately adjacent to the fistulous connection point with balloon inflation. A single injection of Onyx lasting 7 min was performed to cross the fistulous shunt and achieve angiographic obliteration (figure 3). The patient did not suffer any complications and was discharged home following a routine overnight observation.

Posterior parietal convexity dural arteriovenous fistula (dAVF). (A) Posterior middle meningeal artery supply to the dAVF. (B) Inflated Scepter C balloon catheter (white arrows) superselective angiogram demonstrating a fistula with the cortical vein draining into the superior sagittal sinus. (C) Inflated balloon (white arrows) with Onyx cast extending through the fistulous connection to the draining vein. (D) Post-embolization control angiogram with dAVF no longer opacifying.
Case No 4: left-sided paraclinoid/cavernous sinus meningioma
A 53-year-old patient presented with left visual field loss, minimal short term memory loss, fatigue, and increased confusion. On examination the patient had a right-sided lateral visual field deficit in the right eye and decreased visual acuity in the left eye. The patient's left pupil was approximately 5.0 mm and sluggish in response to light. The patient subsequently had an MRI that demonstrated a left-sided clinoidal/cavernous sinus mass measuring 5.6×5.5×4.9 cm, consistent with meningioma.
The patient had successful balloon augmented Onyx embolization using a Scepter C balloon catheter via an anterior division branch of the left middle meningeal artery (figure 4). Single injection of a middle meningeal artery branch allowed for efficient and deep penetration embolization. Total time for embolization was 30 min. The patient experienced no post-embolization complications and was taken for resection of the mass 3 days later. The postoperative course was uneventful and the patient tolerated both the embolization and resection without complications. The patient was discharged on postoperative day 2. On follow-up, improved vision in the right eye was reported but poor vision in the left eye was still maintained.
Left skull base meningioma. (A) MRI with gadolinium demonstrating homogeneously enhancing left skull base mass. (B) Lateral projection demonstrating a hypervascular tumor. (C) Inflated Scepter C balloon catheter (white arrows) in the middle meningeal artery branch with early single injection Onyx cast. (D) Progressive single injection Onyx cast of the middle meningeal artery pedicle. (E) Post-embolization control angiogram with a significant decrease in tumor vascularity.
Case No 5: carotid body tumor
A 46-year-old patient presented with continued headache and dizziness. The patient had a previous diagnosis of bilateral carotid body tumors and had the left side resected 1 year previously with resulting left vocal cord paralysis. As a result of continued headaches, dizziness, and elevated blood pressure, the patient underwent balloon augment embolization of the right-sided carotid body tumor. The carotid body tumor was successfully embolized (figure 5) but the patient suffered right vocal cord paralysis post-embolization and experienced difficulty breathing. The patient was initially placed on biphasic positive airway pressure, and breathing requirements lessened over the next few post-embolization days until the patient tolerated room air. The vocal cord paralysis persisted and on follow-up the patient suffers from dysphonia and mild dysphagia likely related to acute edema of the tumor with resulting compression of the recurrent laryngeal nerve. The patient's headaches, dizziness, and blood pressure symptoms have resolved since embolization.

Carotid body tumor. (A)Inflated Scepter C balloon catheter superselective angiogram demonstrating a hypervascular mass supply from the occipital artery branch. (B) Occipital artery branch single injection Onyx embolization. (C) Post-embolization control angiogram with a significant decrease in tumor vascularity.
Case No 6: thyroid mass
A 56-year-old patient presented with an enlarging neck mass and dysphagia. The patient was evaluated by the ear, nose, and throat department for a 5.0×6.0 cm hypervascular thyroid mass and referred for pre-resection embolization. Angiography revealed a robust tumor blood supply primarily from an enlarged left inferior thyroid artery. A Scepter C balloon catheter was advanced into the feeding pedicle and Onyx embolization was performed, which also penetrated into the left superior thyroid artery feeding branches to the tumor. With balloon inflation we were able to obtain deep penetration and decreased time to complete embolization (figure 6). Embolization was also performed via single Scepter C balloon catheters in the right superior and inferior thyroid arteries. Resection was performed the following day. There were no neurological complications.
Thyroid mass. (A) Hypervascular thyroid mass with a supply from the left inferior thyroid artery. (B) Inflated Scepter C balloon catheter (white arrows) superselective angiogram demonstrating a hypervascular thyroid mass supply in the inferior thyroid artery. (C) A Scepter C balloon catheter was withdrawn more proximally to achieve Onyx embolization of both dilated inferior thyroid artery (white arrows) branches supplying the tumor. (D) Post-embolization control angiogram with a significant decrease in tumor vascularity.
Case No 7: extracranial occipital arteriovenous fistula
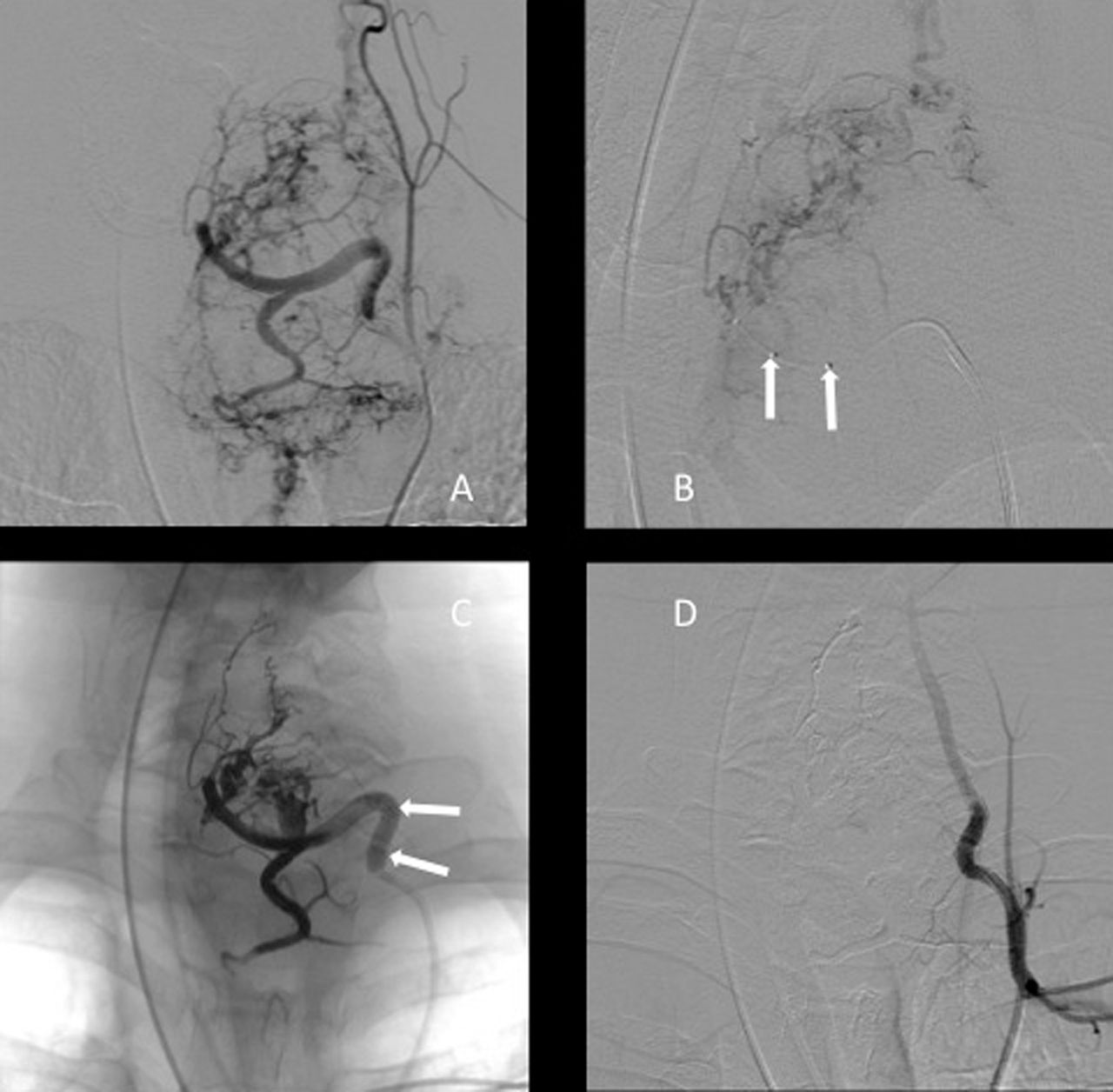
A 33-year-old patient presented with occipital headaches and an enlarging tender occipital mass. An extracranial occipital arteriovenous fistula was discovered. A Scepter C balloon catheter was advanced successfully deep into the tortuous left occipital vein to achieve transvenous embolization of the fistula. Another Scepter C balloon catheter was successfully navigated distally through a tortuous right occipital artery to complete embolization of the fistula (figure 7). The patient was seen in clinic 1 month after the procedure and the headaches and scalp tenderness have resolved.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Extracranial occipital arteriovenous fistula. (A) Arteriovenous fistula with a supply from the right occipital artery and brisk venous outflow via the bilateral occipital veins. (B) Inflated Scepter C balloon catheter (white arrows) with left occipital vein transvenous Onyx embolization. (C) Inflated Scepter C balloon catheter (white arrows) with right occipital artery branch Onyx embolization. (D) Post-embolization control angiogram with the fistula no longer opacifying.
Discussion
The Scepter C balloon catheter was intended for use in balloon remodeling for aneurysm coil embolization. We have described our experiences with this device for that indication as well as stenting of cerebral aneurysms and treating vasospasm following subarachnoid hemorrhage.8–10 In this report, we summarize our experience utilizing the Scepter C catheter for balloon augmented Onyx embolization in diverse head and neck pathologies (table 1). The Scepter C is a dual lumen balloon catheter with an outer lumen for balloon inflation and a second inner 0.0165 inch working lumen for a microwire. This allows for use of standard 0.014 inch microwires that are more navigable and provide more support for over the wire navigation, permitting the Scepter C balloon catheter to be deployed more distally in the vasculature despite its larger diameter. We have found that the Scepter C balloon catheter can be delivered to similar locations as most flow directed Onyx delivery microcatheters.
Only a few previous cases of balloon augmented embolization have been reported in the literature. These were used for treatment of dural arteriovenous fistulae and AVM5 ,6 ,11 and utilized the HyperForm and HyperGlide balloons (eV3 Neurovascular, Irvine, California, USA) to control the flow of Onyx. These balloons cannot be employed as standalone devices for Onyx embolization as they require the presence of a microwire to close the balloon valve to maintain inflation, thereby blocking the lumen of the catheter for embolisate administration. Consequently, the use of these single lumen balloons requires the placement of an additional catheter, in parallel, to deliver the Onyx embolisate distal to the inflated balloon. Employing this strategy of dual catheters in parallel, there is a risk of Onyx reflux since the balloon is prevented from achieving complete occlusion of the lumen of the parent vessel because of the adjacent microcatheter.7 In addition, the older generation balloon catheters were more difficult to navigate since they utilize a 0.010 inch microwire. Another disadvantage is the requirement to navigate two catheters (microcatheter and separate balloon catheter) in what is often times challenging anatomy.
The dual lumen Scepter C balloon catheter has several advantages for use with Onyx embolization over older devices. Inflating the balloon creates a proximal plug blocking retrograde reflux of embolisate and allowing Onyx to travel forward, avoiding inadvertent embolization of non-target vessels. This technique bypasses the need to form a large Onyx plug in the target vessel which significantly reduces the amount of time spent building a plug and reduces the incidence of reflux and proximal non-target vessel occlusion. The inner working lumen of the balloon permits delivery of Onyx distal to the inflated balloon. This significantly reduces the amount of time spent embolizing lesions and reduces contrast load to the patient and radiation exposure to both the patient and operator. Additionally, we have found that the ability to incorporate a 0.014 inch microwire makes the Scepter C balloon catheter more navigable, permitting distal access within even challenging and highly tortuous vasculature. This allows for more selective embolization of vascular pedicles faster and deeper penetration into the lesion, and avoids compromising the blood supply to non-involved areas of the head and neck. We believe the balloon augmented Onyx embolization technique represents a valuable tool to add to the armamentarium of the neurointerventionalist to address a variety of head and neck lesions.
Footnotes
-
Contributors Each author listed should receive authorship credit based on material contribution to this article, their revision of this article, and their final approval of this article for submission to this journal.
-
Competing interests None.
-
Ethics approval The study was approved by the institutional review board of the Medical University of South Carolina.
-
Provenance and peer review Not commissioned; externally peer reviewed.