Article Text

Abstract
Background The initial experience with the large diameter Penumbra Coil 400 (PC400) system has been positive regarding safety, efficacy, improved packing density and cost effectiveness, but follow-up data are limited.
Methods This is a single-center retrospective review of 76 aneurysms treated with PC400 coils compared with 301 aneurysms treated with a variety of different bare platinum and bioactively coated coils. Atypical and giant aneurysms were excluded as well as those that had undergone previous treatment. Occlusion classification was determined immediately after the procedure and at short-term follow-up.
Results Compared with controls, in the PC400 group fewer coils were used (3.53 vs 5.44, p<0.05), procedure time was decreased (48 vs 64 min, p<0.05) and packing density was increased (31.7% vs 24.8%, p<0.05). There were more grade III aneurysms (71.1% vs 38.2%, p<0.05) and fewer grade I aneurysms (13.2% vs 30.2%, p<0.05) in the PC400 group than in the control group immediately after the procedure. At first follow-up, however, more aneurysms in the PC400 group improved (51.3% vs 28.7%, p<0.05) in angiographic grade leading to similar rates of acceptable outcome (grades I or II) at first follow-up (PC400 79.5% vs control 77.2%). The adverse event rate was similar in the two groups.
Conclusions Large diameter PC400 coils can be used to safely treat cerebral aneurysms with fewer coils, decreased procedure time and increased packing density compared with standard coils. The early angiographic outcome is similar to that achieved with standard coils.
- Aneurysm
- Coil
- Intervention
- Technology
Statistics from Altmetric.com
Introduction
The Penumbra Coil 400 (PC400) is a new generation large diameter (0.0200 inches) platinum coil that has been available for use in the USA since 2011 for the endovascular treatment of both ruptured and unruptured intracranial aneurysms. The initial experience with the PC400 system has been positive, specifically regarding safety, efficacy, improved packing density and cost effectiveness.1–3 These advantages have been attributed to the larger coil diameter/volume and inherent softness of the PC400 system.4 The initial reports, however, have provided only limited follow-up data. We report our extended experience with the PC400 system. We hypothesize that cerebral aneurysms can be treated safely with large diameter PC400 coils, with the use of fewer coils, decreased procedure time, increased packing density and similar early angiographic compared to standard coils.
Methods
This is a single-center retrospective case review of cerebral aneurysms treated with coil embolization. The study group included 75 patients with 76 aneurysms treated with PC400 coils from April 2011 to August 2013 and the control group included 282 patients with 301 aneurysms treated with a variety of bare platinum and coated coils from April 2003 until August 2013. The coils used in the control group included Orbit (Codman), GDC (Stryker), Trufill (Codman), Galaxy (Codman), Matrix (Stryker), Target (Stryker) and Hydrocoil (Microvention). All aneurysm embolizations were performed by three interventionalists using the same endpoint of maximum safe packing of the aneurysm. PC400 coils were delivered using a microcatheter with a 2.6 french distal outer diameter, whereas standard coils were delivered using a microcatheter with a 1.7 french distal outer diameter. PC400 coils all have 0.0200 inch outer diameter, whereas standard coils all have a 0.0150 inch outer diameter or less.
Criteria for inclusion were subjects with saccular cerebral aneurysms treated by coil embolization, including both ruptured and unruptured aneurysms. Exclusion criteria included atypical and giant aneurysms as well as any aneurysms that had undergone previous treatment. Aneurysmal and subject characteristics were determined by review of both the subject's medical chart and angiographic data. Aneurysm size was determined both qualitatively and quantitatively. The qualitative system involved using the maximum dome diameter (small: <10 mm, large: 10–25 mm, giant: >25 mm). Aneurysmal volume, coil volume and packing density were measured using AngioCalc (http://www.angiocalc.com), an open-source web-based calculator endorsed by all of the major coil manufacturers. Procedure time was determined by analysis of the imaging, defined as the time from establishment of the working angiographic view to the end of the procedure.
First follow-up was defined as the first angiographic follow-up at least 3 months after the procedure. All initial and follow-up angiograms were reviewed by either interventionalist (ABP or HM). The Raymond-Roy Occlusion Classification (grade I: no residual aneurysm; grade II: residual neck; grade III: residual aneurysm) was used for aneurysm grading.5 Any contrast seen within the aneurysm at the end of the procedure was defined as grade III even if it was believed to be a result of heparinization or the use of antiplatelet therapy.
Discrete variables, frequency counts and percentage of patients within each category were compared using the Fisher exact test. For continuous variables, the Wilcoxon rank sum test was used for treatment comparisons. Significance levels were reported at the α=0.05 level. For some variables where significance was reached, α=0.01 was reported for additional detail. Subset analysis was performed for different sized aneurysms, assisted coiling, rupture and retreatment status.
Results
The baseline patient and aneurysm demographic characteristics were similar in the two groups and with most aneurysm series in the literature. There was a trend towards fewer ruptured aneurysms in the PC400 group that did not reach statistical significance (PC400 44.7% vs control 57.5%, p=0.054). This finding may be explained by changes in regional referral patterns. There were more anterior communicating aneurysms in the control group (22.6% vs 9.2%, p=0.009) and more posterior communicating aneurysms in the PC400 group (32.9% vs 19.9%, p=0.021). Although there was a greater average dome volume in the control group (224.59 mm3 vs 207.21 mm3, p=0.004), the median dome volume was greater in the PC400 group (110.8 mm3 vs 80.9 mm3), the average diameter was greater in the PC400 group (6.5 mm vs 6.0 mm, p=0.007) and there was a trend towards more large aneurysms in the PC400 group (25.0% vs 18.9%, p=0.264), only the last of which did not reach statistical significance. This paradox may possibly be explained by a small number of large aneurysms in the control group that skewed the average dome volume (table 1).
Baseline patient and aneurysm demographic information
There was no difference in stent assistance between the two groups (PC400 26.3% vs control 27.6%, p=0.886). There was, however, a trend towards less need for balloon assistance in the PC400 group that did not reach statistical significance (5.3% vs 12.0%, p=0.098). All patients in the PC400 group were treated exclusively with PC400 coils except for one patient (1.3%) who was treated with a combination of four PC400 and three Target coils. This patient was included in the PC400 group because the majority of the coil length was PC400. Seventy-one patients (23.6%) in the control group were treated with a combination of standard sized coils. Compared with the control group, the PC400 group was treated on average with fewer coils (3.53 vs 5.44, p=0.002) and decreased procedure time (48 min vs 64 min, p=0.000). Despite this, the PC400 group had increased coil volume (56.15 mm3 vs 40.19 mm3, p<0.001) and increased packing density (31.7% vs 24.8%, p<0.001; table 2).
Procedural information
In the PC400 group, at least one follow-up was available in 51.3% of patients (n=39). It is important to note that many patients were not yet within the time period for their first follow-up (n=17) and some died during their initial hospitalization (n=6). Taking this into account, the yield for first follow-up was 73.6%. In the control group, a single follow-up was available in 71.9% of patients (n=202) (72.9% accounting for the same as above). The average time to first follow-up was 7.01 months in the PC400 group and 8.34 months in the control group (p=0.207).
Compared with controls, there were fewer grade I aneurysms (13.2% vs 30.2%, p=0.002), fewer grade II aneurysms (15.8% vs 31.6%, p=0.006) and more grade III aneurysms (71.1% vs 38.2%, p<0.001) in the PC400 group immediately following the procedure. Many of the grade III aneurysms (n=37) had contrast filling within the interstices of the coils and fewer grade III aneurysms (n=17) had contrast filling along the aneurysm wall. At first follow-up, however, there was no statistical difference in occlusion grade between the two groups (table 3). Using grade I or II as a definition of acceptable outcome, the rates were similar between the two groups (PC400 79.5% vs control 77.2%). In addition, 12 aneurysms in the PC400 group had a second angiographic follow-up at an average of 19.01 months, at which time none had changed in occlusion grade.
Initial and follow-up occlusion class data
More aneurysms in the PC400 group improved in angiographic grade (51.3% vs 28.7%, p=0.009). The recanalization rate was not statistically different between groups (PC400 5.1% vs control 11.4%, p=0.388). Compared with the control group, there was a trend towards fewer retreatments in the PC400 group that did not reach statistical significance (2.6% vs 9.3%, p=0.059; table 4). Subset analysis did not yield different results from the entire group analysis.
First follow-up occlusion class progression and retreatment
The adverse event rate was 6.7% in the PC400 group and 9.5% in the control group. One patient in the PC400 group had extravasation from a wire perforation of a pontine perforator during coiling of an unruptured basilar tip aneurysm and ultimately died secondary to subarachnoid hemorrhage and intractable intracranial hypertension. In both groups, almost all parent or distal vessel compromise, thrombus/platelet plug formation and in-stent stenosis resolved with either intraoperative or postoperative treatment. The rates of permanent disability or death (as a result of the adverse event) in the PC400 and control groups were 1.3% and 2.1%, respectively (table 5).
Adverse events
Discussion
PC400 coils are soft platinum coils of large diameter (0.0200 inch) specifically designed to address aneurysm recanalization by increasing coil volume and packing density. PC400 coils are bare platinum with stretch-resistant Nitinol wire that is marketed as having 400% more volume per unit length than conventional embolic coils, tight breaks during all stages of packing because of an inherently softer larger diameter coil, complete coverage and neck-to-dome stability with multiple shapes, and exceptionally soft curve finishing coils for treatment of the aneurysm neck or for complete treatment of small aneurysms.6 Together, these properties allow for decreased procedural time and improved packing density.7
There have only been two reports to date evaluating the initial experience with the PC400 system. In 2012 we reported 16 aneurysms treated with the PC400 system and compared these with 79 equally matched aneurysms that were embolized with conventional coils. Compared with conventional coils, the PC400 system achieved higher packing density (36.8% vs 28.1%, p<0.005) with fewer coils (3.9 vs 6.1, p<0.05) and significantly less procedural time (45.7 min vs 64.1 min, p<0.05), and the report concluded that the PC400 system is more efficient than the use of conventional coils. However, no follow-up data were available at the time of this report.2
In 2013 Milburn et al reported 18 aneurysms treated with the PC400 system and compared these with 40 aneurysms treated with Orbit/Galaxy coils. They also found higher packing density (33.7% vs 24.4%) and fewer coils per aneurysm volume (0.026 vs 0.114 coils/mm3) in the PC400 group. The initial occlusion classification within the PC400 group was 10 in class I, three in class II and four in class III. Follow-up angiography was available for 11 of the 18 aneurysms in the PC400 group. The average time to angiographic follow-up was 8.6 months (range 2 weeks to 17 months). At follow-up, 10 aneurysms were unchanged and one aneurysm recanalized requiring further intervention. This report performed a cost analysis and showed improved cost effectiveness with the PC400 system.3
In the present study we show that aneurysm embolization with PC400 coils results in the use of fewer coils and decreased procedure time while providing greater coil volume and packing density. Increased procedure time has been shown to be associated with an increased ischemic stroke rate,8 which suggests that the PC400 may have a greater safety profile. This safety benefit, however, has to be weighed against the risk of procedural aneurysm rupture secondary to the large coil diameter. Fortunately, we had a low rate of procedural aneurysm rupture (1.3%, n=1) and do not believe this to be a significant concern. Higher packing density has been associated with improved angiographic outcome,9–12 although the relationship is controversial and it may have less influence for small aneurysms,13 those treated with stent assistance14 and unruptured aneurysms.9 Although the PC400 coils provided increased packing density, because the recanalization rates were not statistically different, it is unclear whether this is an added benefit.
There were a large number of grade III aneurysms immediately following the procedure. This finding could be explained by a large number of aneurysms retaining contrast between coil interstices. The larger diameter/volume of the PC400 coil, although increasing the overall coil volume, results in the coils occupying a less disperse volume of the aneurysm allowing more contrast opacification in the larger unoccupied portions of the aneurysm (figure 1). Many of these aneurysms had contrast opacification only within the coil interstices and had a propensity to improve (figures 2⇓–4). In addition, many patients in this population who underwent ultra-early angiographic follow-up for vasospasm had already progressed to occlusion. Although the argument could be made that a grade III aneurysm is at risk of rupture or re-rupture, we did not observe this in our population and suspect that this subtype of grade III aneurysm behaves similarly to a grade I or II aneurysm.

Cross-sectional exaggerated depiction of PC400 coils (left) and control coils (right). The larger diameter of the PC400 coils allows for greater overall coil volume/packing density; however, less disperse packing accounts for a greater percentage of grade III results in the PC400 group.
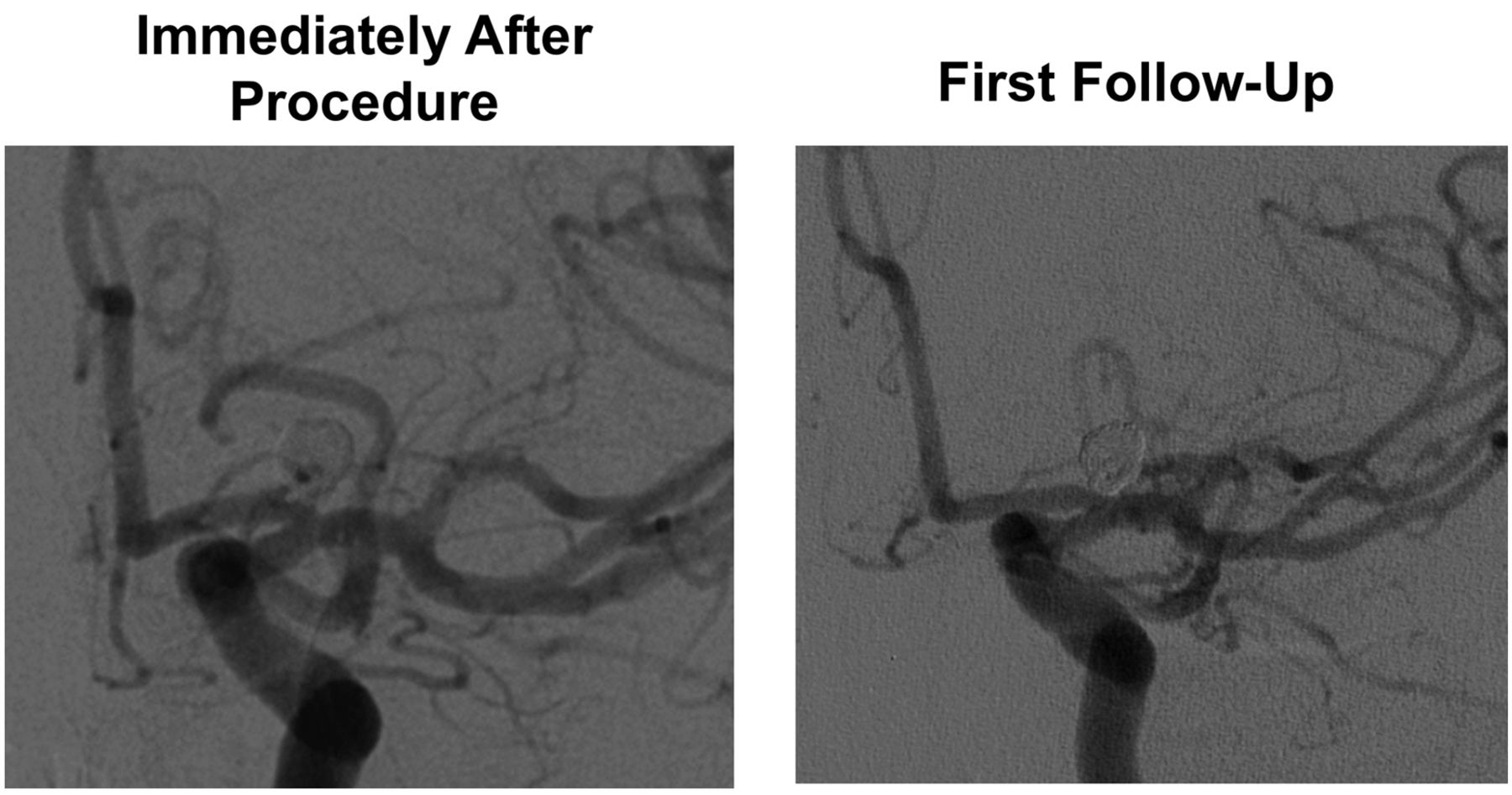
Angiographic images of an elderly patient with an unruptured left internal carotid artery bifurcation aneurysm treated with coil embolization immediately after the procedure (left) and at 5.7 months (right); the grade III aneurysm has progressed to a grade I aneurysm.

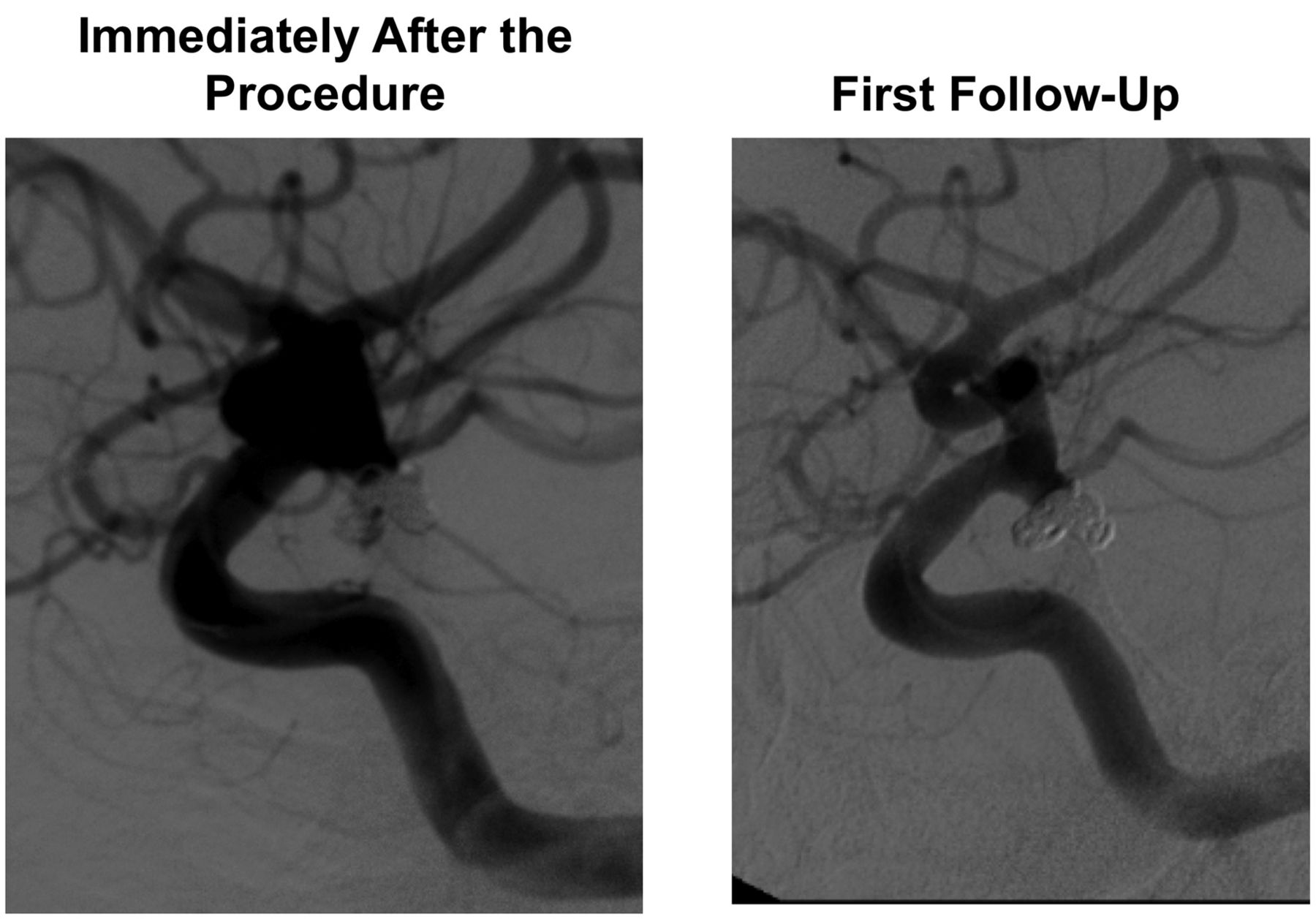
Angiographic images of a middle-aged patient with a ruptured basilar tip aneurysm treated with coil embolization immediately after the procedure (left) and at 6.1 months (right); the grade III aneurysm has progressed to a grade I aneurysm.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Angiographic images of a young patient with a ruptured right posterior communicating artery aneurysm treated with coil embolization immediately after the procedure (left) and at 8.5 months (right); the grade III aneurysm has progressed to a grade I aneurysm.
Aneurysm recanalization is a risk factor for aneurysm re-rupture.15 A meta-analysis in 2009 found the overall recanalization rate of more than 8000 coiled aneurysms to be approximately 20%.16 In this analysis, the authors found similar recanalization and retreatment rates among both bare platinum and newer generation modified coils. An even more recent meta-analysis published in 2013 found similar rates of ‘unfavorable outcome’ (defined as either ‘recanalization’, <90% occlusion or ‘incomplete occlusion’ at follow-up) among bare platinum, Matrix, Hydrocoil and Cerecyte coils at follow-up.17 The initial studies of the PC400 do not adequately address long-term stability and recanalization.
At short-term follow-up we found that many aneurysms in the PC400 group improved in angiographic grade and very few worsened, leading to equivalent overall results to standard coils. The recanalization rate was similar in both groups and lower than the 20% reported in the literature. It is important to note that there was a trend towards fewer ruptured aneurysms in the PC400 group, and this may favorably influence the recanalization rate in that group. The retreatment rate was not statistically different between the groups, and it is probably premature to compare the retreatment rate given the overall shorter follow-up in the PC400 group. All aneurysms that were available for delayed second follow-up remained stable compared with the first follow-up. In addition, the adverse event rate was low and comparable to the control group. Importantly, the procedural rupture rate was low in the PC400 group, which was a potential concern given the large coil diameter.
We understand that the study is limited by its retrospective nature and that it only addresses angiographic outcome rather than clinical outcome. In addition, the two groups were treated during different time periods. The PC400 group was treated more recently and the results may be influenced by increased overall experience. Because the PC400 group was treated more recently, first follow-up was not available for a portion of these patients. With regard to procedural limitations, our experience is that PC400 coils are not ideal for smaller distal aneurysms due to the larger catheter diameter. This may account for the statistically smaller number of anterior communicating artery aneurysms in the PC400 group.
Conclusions
This study represents the largest review of the PC400 system to date for treating cerebral aneurysms. We have shown that the large diameter PC400 system can safely achieve equivalent short-term angiographic results compared to standard coils while offering the benefits of the use of fewer coils, decreased procedure time and increased packing density.
References
Footnotes
-
Contributors All of the authors participated in the research and preparation of the manuscript. JRM, ABP and HM participated in study design and analysis and interpretation of data. JRM, MFP and AAP participated in data collection. All authors participated in manuscript drafting and finalization as well as approval of the final document.
-
Competing interests ABP is a consultant for Penumbra.
-
Ethics approval Ethics approval was obtained from the Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.