Article Text

Abstract
Background and purpose Tandem vascular occlusions are an important cause of acute ischemic stroke (AIS) and present unique treatment challenges. We report our experience of managing a subset of AIS patients with extracranial vascular stenting/angioplasty and intracranial revascularization.
Methods Consecutive patients who presented at three centers with AIS from tandem vascular occlusions confirmed by brain and neck CT imaging were included in the study. We retrospectively analyzed the patient demographics, National Institute of Health Stroke Scale (NIHSS) score and modified Rankin Scale (mRS) score at the time of admission, treatment strategy, angiographic results using the Thrombolysis In Cerebral Infarction (TICI) score, and clinical and imaging follow-up.
Results Twenty-eight patients were included. The mean NIHSS score at admission was 18. Extracranial carotid occlusions with a concomitant middle cerebral artery occlusion were seen in 89.3% of patients (n=25) and vertebral artery combined with basilar artery lesions in 10.7% (n=3). An antegrade approach (ie, treatment of the extracranial lesion first) was used in 24 patients (85.7%). Proximal occlusion recanalization was achieved usually with a stent (n=27; 96.4%). Pursuant to intracranial revascularization techniques, ≥TICI 2A recanalization was seen in 96.4% of patients. An mRS score of ≤2 at 90 days was achieved in 56.5% of patients.
Conclusions Our study shows preliminary data from three centers on recanalization of tandem occlusions in patients presenting with AIS. There was a preference to revascularize the proximal occlusion using a stent followed by distal recanalization with mechanical thrombectomy, intra-arterial thrombolysis or a combination of these. This approach has low periprocedural complications and can achieve an excellent angiographic and clinical outcome.
- Stroke
- Stent
Statistics from Altmetric.com
Introduction
Tandem vascular occlusions include a proximal extracranial occlusion in conjunction with a downstream intracranial occlusion. They complicate the treatment of acute ischemic stroke (AIS) and present a complex treatment challenge to this unique subset of AIS patients. The natural history of these lesions usually leads to high morbidity and mortality.1 ,2 There have been studies using only intravenous tissue plasminogen activator (IV tPA) for these lesions.3 The low rate of recanalization of proximal internal carotid artery (ICA) occlusion with IV tPA alone is also likely to be responsible for poorer clinical outcomes.4–7 Unfavorable recanalization results after the use of either IV2 ,8 or intra-arterial (IA)9 tPA led to the development of an alternative treatment approach in such lesions to achieve adequate reperfusion and to improve patient clinical outcome. IA tPA infusion in middle cerebral artery (MCA) occlusion via an access through the communicating arteries,10 thromboaspiration via the anterior communicating artery has been described11 to address the distal occlusion in case of an occluded proximal ICA. The recent availability of stent retriever-based thrombectomy devices to the field of AIS has enabled interventionalists to attain better recanalization rates.12–14 There are limited case reports and series regarding the use of acute endovascular intervention in tandem vascular occlusions,6 ,15–17 either using antegrade or retrograde revascularization. However, the order in which the affected vessels should be treated to achieve rapid and permanent flow restoration has not been determined.16 This retrospective analysis of consecutive patients presenting with AIS pursuant to tandem lesions at three institutions evaluates the endovascular approach, recanalization rates and patient clinical outcome retrospectively after a staged endovascular approach.
Materials and methods
Consecutive patients presenting with AIS secondary to a tandem lesion and treated endovascularly at the University of Massachusetts Memorial Medical Center, USA (n=19), the Chungnam National University Hospital, South Korea (n=3) and Baptist Cardiac and Vascular Institute, USA (n=6) between June 2006 and April 2013 were identified and their data were reviewed.
We included patients who presented with extracranial ICA occlusion and a concomitant occlusion in either the distal ICA ‘T’ occlusion, MCA or anterior cerebral artery (ACA), as well as patients presenting with lesions in the vertebral artery (VA) and a simultaneous occlusion of the basilar artery (BA). Tandem occlusions were identified prior to intervention with neck and brain CT angiography (CTA). We collected the information of each patient's stroke risk factors, National Institute of Health Stroke Scale (NIHSS) scores and modified Rankin Scale (mRS) scores on admission and at discharge. Data also collected included method of anesthesia during intervention, approach for intracranial revascularization and use of cerebral protection devices. The final recanalization achieved was evaluated using the Thrombolysis In Cerebral Infarction (TICI) score. In addition to the NIHSS score at the time of discharge, the mRS score at 90 days and follow-up imaging data for in-stent stenosis were also collected.
Results
A total of 28 patients were identified to have tandem vascular occlusions (19 men and 9 women, mean age 58.7 years, range 30–83). Patient comorbidities included hypertension (64.3%), dyslipidemia (42.9%), smoking (35.7%), diabetes (32.1%) and alcohol abuse (17.8%).
Mean NIHSS and median mRS scores at admission were 18 and 4, respectively. In 82.1% of cases the intervention was performed under general anesthesia.
The antegrade treatment approach (revascularization of the proximal occlusion followed by the distal occlusion) was used in 24 patients (85.7%) while the reverse/retrograde technique (treatment of the intracranial lesion before revascularization of the proximal lesion) was used in four patients (14.3%). Extracranial carotid occlusions with a concomitant MCA occlusion were seen in 89.3% of all lesions (n=25) and VA combined with BA lesions in 10.7% (n=3). Proximal occlusion recanalization (ICA and VA) was achieved usually with a stent (n=27; 96.4%). The need for angioplasty, whether pre- or post-stent deployment, was decided upon review of the images and was used in 15 patients (60%). In one patient only thrombectomy was used to achieve complete recanalization of the proximal occlusion. IV tPA prior to intervention was administered in 27.3% of patients. In six patients (30%) the distal lesion was treated with IA lysis alone and in 20% with thrombectomy alone. Six patients were treated with IA lysis and thromboaspiration. A combined approach of IA lysis, thrombectomy and angioplasty as well as lysis combined with angioplasty was used in one patient each. The combined approach of lysis with either stenting or thrombectomy was used in two patients each. The treatment strategy and patient outcomes are shown in detail in table 1.
Summary of treatment strategy and patient outcome
The cause of the proximal occlusion was identified as dissection (n=8, 28.6%) or atherosclerosis (n=20, 71.4%). Stents used to treat the proximal lesion were a single Precise stent (Cordis Endovascular, New Brunswick, New Jersey, USA; n=14); two overlapping Precise stents (n=2); a combination of Precise and Enterprise (Codman Neurovascular, Raynham, Massachusetts, USA) stents (n=2); a combination of Precise and Neuroform (Stryker Neurovascular, Fremont, California, USA) stents (n=1); and three Enterprise stents (n=1). Additionally, Wallstent (Boston Scientific, Natick, Massachusetts, USA), Wingspan (Stryker Neurovascular) and Xact stents (Abbott Vascular, Redwood City, California, USA) were used in one patient each. Thrombectomy only was used in one case to revascularize the carotid lesion. The VA reconstructions were achieved with the use of a Wallstent, an ION stent (Boston Scientific) and four overlapping Xact stents. Endovascular protection devices were used in six cases with the antegrade treatment approach and stent placement. Patients were loaded with 650 mg of aspirin via either the nasogastric/orogastric or per rectal route if stenting was anticipated. We generally acquire a cone-beam CT (Allura Biplane FD20/20, Philips Medical, Best, The Netherlands) in our neuroangiography suite immediately after treatment to rule out cerebral hemorrhage; only thereafter is a 600 mg loading dose of clopidogrel administered.
The distal occlusion (MCA, ACA or BA) was treated with a stent, mechanical, pharmaceutical or combination of various modalities. The mode of revascularization was based on operator preference and the available armamentarium of stroke devices at the time of the event. IA lysis alone was used in six cases, IA lysis with thrombectomy was used in five patients and thrombectomy alone was used in seven. Combined approaches consisting of IA lysis, angioplasty and lysis, thrombectomy and angioplasty were used in one patient each. IA lysis with stenting was used in two cases each. One patient was treated with IA lysis, thrombectomy and stenting. The combined approach of IA lysis with thromboaspiration was used in five patients. All proximal lesions in the posterior circulation were stented and all BA occlusions were treated with thrombectomy only (see online supplemental table I).
Complete recanalization graded (TICI 3) and partial recanalization with partial reperfusion (TICI 2A and 2B) was achieved in 13 and 14 cases, respectively. An mRS score of ≤2 at discharge was achieved in 39.3% of patients; the mean patient NIHSS score was 7.6 (available for 24 patients). Symptomatic and asymptomatic intracranial hemorrhage (ICH) was seen in 9.1% and 36.4%, respectively. An mRS score of ≤2 at 90 days was achieved in 56.5% of patients.
In this case series four patients (14%) died, two secondary to stroke and two from symptomatic ICH. In the two cases of cerebral hemorrhage, decompressive craniectomy was required for significant mass effect and midline shift. All of the patients who died were treated with the antegrade approach, received IV and/or IA tPA, had a stent placed without use of an embolic protection device and had ≥TICI 2A recanalization (see online supplemental table II).
Illustrative case 1
A patient aged in his/her early 50 s presented with right facial droop, right hemiparesis and expressive aphasia consistent with a NIHSS score of 10 and a mRS score of 4 at the time of admission. Non-contrast CT was negative for any hemorrhage or any large territory infarction so IV tPA was administered. CTA demonstrated a left MCA (arrow, figure 1A) and a tandem left ICA occlusion (double arrows, figure 1B). The patient was intubated in the neuroangiography suite without letting the blood pressure drop during induction. The time to treatment was 202 min from the last time the patient was seen normal. A diagnostic angiogram of the right ICA showed poor perfusion of the left MCA territory (figure 1C). Angiography of the left common carotid artery confirmed the complete occlusion of the left ICA at its origin (arrow, figure 1D) with minimal filling of the supraclinoid ICA via collaterals from the internal maxillary artery. A microcatheter was navigated to the left ICA, followed by a superselective angiogram to confirm the intravascular position and the left MCA occlusion (arrow, figure 1E). An exchange wire was then used to deploy a 6 mm×30 mm Precise Pro RX (Cordis, Miami Lakes, Florida, USA) carotid stent. This was followed by PTA with 3.5 mm×20 mm and 4.5 mm×20 mm balloons achieving an excellent result (figure 1F). Using the exchange length wire, a Penumbra 3MAX reperfusion catheter (Penumbra, Alameda, California, USA) was used to access the left MCA occlusion followed by thromboaspiration (figure 1G). In addition, 9 mg of IA tPA was infused into the left MCA. The final angiogram demonstrated a TICI 2B recanalization (figure 1H). A loading dose of 650 mg aspirin was given via the nasogastric tube after deploying the carotid stent. In addition, 14 mg eptifibatide was also infused into the proximal cervical ICA for platelet aggregation/thrombus formation. Time from groin puncture to carotid stenting was 33 min and from groin puncture to TICI 2B recanalization using IA tPA and Penumbra thromboaspiration was 108 min. A cone-beam CT was performed in the angiography suite, confirming no ICH but mild contrast staining (figure 1I). MRI with diffusion and gradient echo images showed no evidence of acute ischemic focus or any hemorrhage (figure 1J). The patient was then started on 75 mg clopidogrel and 325 mg aspirin. The patient returned to complete baseline neurological status in 2 days with a NIHSS score of 0 and mRS score of 0 at the time of discharge. Follow-up angiography at 2.5 months for treatment of incidentally discovered cerebral aneurysm showed no in-stent stenosis in the previously placed left carotid stent (figure 1K). The patient continues to be neurologically intact without any sequelae of prior AIS.

CT angiography demonstrates a left middle cerebral artery (MCA) (arrow, (A) axial reformatted MIP image) and a tandem left internal carotid artery (ICA) occlusion (double arrows, (B) coronal reformatted MIP image). The right common carotid angiogram shows a poor perfusion of the left MCA territory (C, frontal projection). Angiogram of the left common carotid artery confirms the complete occlusion of the left ICA at its origin (arrow, D). Superselective angiogram confirms the intravascular location of the microcatheter and the left MCA occlusion (arrow, E). Angiogram following complete revascularization with stent and percutaneous transluminal angioplasty shows good result (F). Penumbra 3MAX reperfusion catheter was used to access the left MCA occlusion followed by thromboaspiration (arrow, G). The final angiogram demonstrates Thrombolysis In Cerebral Infarction 2B flow (H). Cone-beam CT demonstrates no intracranial hemorrhage but mild contrast staining (I). MRI with diffusion and gradient echo images shows no evidence of an acute ischemic focus or hemorrhage (J). Follow-up angiogram at 2.5 months shows no in-stent stenosis of the stented carotid segment (K).
Illustrative case 2
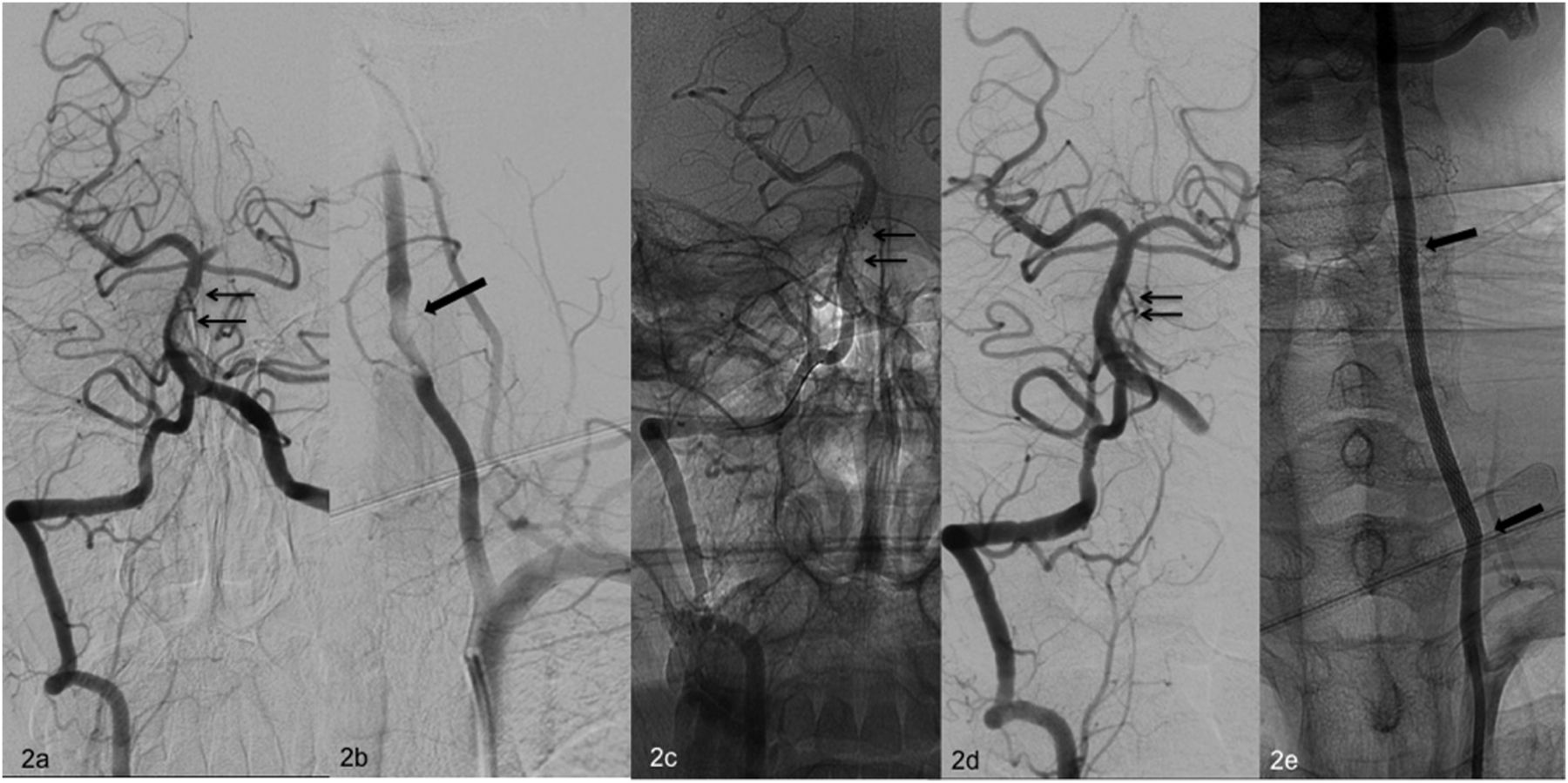
A patient aged in his/her late 20 s was transferred to the emergency room with decreased consciousness. The NIHSS and mRS scores on admission were 15 and 4, respectively. MRI/MRA showed acute ischemic changes on the pons and left cerebellum with severe narrowing/thrombus in the mid basilar trunk and the proximal left VA. IV tPA was not given due to uncertain time of onset of symptoms. After being transferred to the neuroangiography suite, partially occlusive thrombus was seen in the mid-BA (double arrows, Figure 2A). There was near occlusion of the left V2 segment (figure 2B) with an intact right VA. Under conscious sedation, a 4×20 mm Solitaire stent retriever (ev3, Irvine, California, USA) was deployed via the right VA incorporating the thrombus in the BA for 5 min (double arrows, figure 2C). The Solitaire stent was retrieved into the guide catheter. Thrombus was observed on the stent surface. Complete recanalization of the BA was achieved (double arrows, figure 2D). Thereafter, the guide catheter was navigated into the proximal left VA and a 6×22 mm Wallstent (Stryker, Plymouth, Minnesota, USA) was deployed without the use of a distal protection device and covering the dissection-like lesion (figure 2E). IA tirofiban was infused via a microcatheter at the proximal left VA following stenting. Follow-up angiography showed complete TICI 3 recanalization of the VA without distal emboli. Time from groin puncture to TICI 3 intracranial revascularization was 35 min and from groin puncture to VA stenting was 55 min. Follow-up MRI demonstrated no ischemic changes. Thereafter, the patient was started on clopidogrel and aspirin. The NIHSS score at discharge was 3 and the 90-day mRS score was 1. Neck CTA showed patent left VA at 1-month follow-up examination.

{kind=link}
{kind=link}
Right vertebral artery (VA) angiogram demonstrates the partially occlusive thrombus in the mid-basilar artery (double arrows, A). Left subclavian artery angiogram shows near occlusion of the left VA at V2 segment (B). A 4 mm×20 mm Solitaire stent retriever was deployed incorporating the thrombus (double arrows, C). Right VA angiogram after clot removal demonstrates complete recanalization of the basilar artery (double arrows, D). Angiogram demonstrates VA stenting with good reconstruction of the diseased and near occluded segment (E).
Illustrative case 3
Details are shown in the online supplement.
Discussion
In our series of AIS secondary to tandem lesions, technical success (TICI ≥2B) was achieved in 15 cases (68.2%). The clinical outcome in our series was comparable to other studies of patients with tandem lesions.6 ,16 ,18 Given the poor natural history of these lesions or the poor clinical outcome with IV tPA treatment alone,2 these data from multiple case series demonstrate the potential value of endovascular treatment of this complex disease.
Major arterial occlusions are associated with high stroke scales19 ,20 and worse clinical outcomes.21 ,22 The recanalization rates for major vessel occlusions are low with IV tPA alone,23 especially with proximal occlusions,7 compounded with a risk of symptomatic ICH of 1.7–8%.24–28
One of the reasons that tandem lesions have worse outcomes is the possibility of reduced or absent antegrade flow in the ACA. The reduced (in cases of small anterior communicating artery) or absent (in cases of isolated hemisphere) ACA flow is insufficient for a proper leptomeningeal blood supply to the occluded MCA. The small ACA also limits the amount of flow available to the striatal vessels originating from the ACA, such as the recurrent artery of Heubner. There are case reports of attempting to recanalize the intracranial occlusion via the ACA.10 ,11 We choose not to do so, to prevent any risk to the contralateral hemisphere. Luminal compromise of the anterior communicating artery can further decrease the collateral supply to the occluded vasculature. Any catheter-related or thromboembolic event to the contralateral hemisphere has the potential for even worse outcomes.
There is no clear consensus on the sequence of proximal versus distal revascularization. The advantage of proximal recanalization followed by distal revascularization is to provide blood flow to the non-occluded ACA. This prevents a recurrent occlusion of the intracranial vessels from slow or stagnant flow. It also allows accessing the intracranial lesion with bigger guide catheters. With this approach, an exchange length wire can be kept in the distal intracranial vasculature at all time, which allows distal access and certainty of the luminal compartment. The ability to advance the balloon guide catheter for proximal flow arrest during clot removal or intermediate guide catheter past the distal end of the stent is very important while removing clots with stent retrievers. This prevents entanglement of stent struts with meshes of stent retrievers. In six cases we observed that infusing IA tPA through the microcatheter between the tandem occlusion was the only intervention necessary after proximal revascularization. These are some of the reasons why we prefer antegrade recanalization strategy to retrograde recanalization. Possible advantages of the retrograde/reverse treatment approach currently discussed include quicker restoration of cerebral blood flow to the intracranial area by prioritising treatment of the distal lesion and possibly reducing cerebral ischemia.
In our case series both antegrade and retrograde strategies were used. However, in most cases antegrade revascularization was performed. We do not propose the superiority of one strategy over the other as long as each of them can be done safely and in a timely manner, but it is our preference to revascularize using the antegrade approach for the abovementioned reasons. A larger randomised study will help to define the superiority of either method.
In our series TICI 2A, TICI 2B and TICI 3 flow was achieved in 96.4%, 71.4% and 46.4% of patients, respectively. In most cases we were able to pass a 0.014 inch microwire past the ICA or the VA occlusion. We usually pass the wire through a microcatheter. The microcatheter is then placed distal to the occlusion site and is used to inject contrast to confirm the nature of the occlusion. This generally helps to differentiate between a dissection and an atherosclerotic lesion. The microcatheter injection is also helpful in delineating the extent of the lesion and confirming the true lumen prior to mechanical thrombectomy or thrombolysis. We then proceed to rapid carotid stenting with or without angioplasty. The use of distal protection devices (DPD) in these cases is left to operator preference. We used DPD in 21.4% of the treated patients. Nevertheless we had a have a low rate of distal emboli. We did not observe distal emboli in cases with DPD (6 patients) and found distal emboli in three out of 22 patients (13.7%) without DPD. We recommend use of DPD whenever possible.
The study limitations include non-randomization and treatment heterogeneity associated with the retrospective study design. We also think that the longitudinal nature of retrospective data acquisition since 2006 has contributed to the technical and thus clinical outcomes. The stroke thrombectomy devices have evolved rapidly and, with the recent availability of stent retrievers, mechanical thrombectomy has become even more efficient and safe. In addition, we may have missed cases that were aborted due to inability to cross the lesion and thus were not included in our analysis.
Conclusion
We present an efficacious and safe treatment strategy for AIS associated with tandem occlusions of intracranial and extracranial arteries. Acute proximal revascularization followed by distal revascularization showed good clinical outcomes in this subset of otherwise difficult to treat acute stroke patients. We think our study opens the doors for future randomised studies to test the efficacy and safety of antegrade revascularization strategies versus IV thrombolysis versus combined mechanical and pharmaceutical revascularization treatment for tandem occlusions.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online supplement
Footnotes
-
Contributors Study conception and design: ASP, IL, AKW. Data collection: ALK, SYH, HJK, MK, EL. Data analysis and interpretation: ASP, IL, GD, MJG, AKW. Literature research: ALK, HJK, JYC, IMJVDB. Drafting the manuscript: ASP, ALK, SYH, EL. Revision of the manuscript for important intellectual content: HJK, MK, GD, IL, JYC, IMJVDB, MJG, AKW. Approval of final version of manuscript: all authors.
-
Competing interests GD is a consultant for Covidien, Codman and Reverse Medical. IL is a consultant for Covidien, Stryker and Codman. MJG is a consultant for Stryker, Codman and Surpass Medical. AKW is a consultant for Stryker and Boston Biomedical Association and received research grant from Philips Medical.
-
Ethics approval Institutional Review Board waiver for retrospective study analysis was obtained for the University of Massachusetts Memorial Medical Center in Worcester, Massachusetts, the Baptist Cardiac and Vascular Institute in Miami, Florida and the Chungnam National University Hospital in South Korea.
-
Provenance and peer review Not commissioned; externally peer reviewed.