Article Text

Abstract
Objective Acute tandem occlusions of the extracranial internal carotid artery (ICA) and a major intracranial artery respond poorly to intravenous tissue plasminogen activator (tPA) and present an endovascular challenge. We describe our experience with emergency stent-assisted ICA angioplasty and intracranial stent-based thrombectomy of tandem occlusions.
Methods Procedures were performed from March 2010 to December 2013. National Institutes of Health Stroke Score (NIHSS) and Alberta Stroke Program Early CT Score (ASPECTS), occlusion sites, collateral supply, procedural details, and outcomes were retrospectively reviewed with IRB waiver of informed consent.
Results 24 patients, mean age 66 years, mean admission NIHSS 20.4, and mean ASPECTS 9 were included. Occlusion sites were proximal ICA–middle cerebral artery (MCA) trunk in 17 patients, proximal ICA–ICA terminus in six, and ICA–MCA–anterior cerebral artery in one. Stent-assisted cervical ICA recanalization was achieved in all patients, with unprotected pre-angioplasty in 24/24, unprotected stenting in 16/24 (67%), and protected stenting in 8/24 (33%), followed by stent-thrombectomy in 25 intracranial occlusions. There was complete recanalization/complete perfusion in 19/24 (79%), complete recanalization/partial perfusion in 3/24 (13%), and partial recanalization/partial perfusion in 2/24 (8%) with no procedural morbidity/mortality. Mean time to therapy was 3.8 h (range 2–5.5) and mean time to recanalization was 51 min (range 38–69). At 3-month follow-up, among 17/22 surviving patients (77%), 13/17 (76%) were modified Rankin Scale (mRS) 0–2 and 3/17 (18%) were mRS 3.
Conclusions In acute tandem ICA–MCA/distal ICA occlusions, extracranial stenting followed by intracranial stent-based thrombectomy appears feasible, effective, and safe. Further evaluation of this treatment strategy is warranted.
- Artery
- Technique
- Stent
- Stroke
- Thrombectomy
Statistics from Altmetric.com
Introduction
Acute extracranial internal carotid artery (ICA) occlusion with tandem distal occlusion is usually associated with major stroke leading to severe disability or death1 ,2; intravenous thrombolysis and other combined approaches have met with limited success.3–7 A significant clot burden and limited delivery of the thrombolytic drug to the distal occlusion may explain the poor results.8 In selected cases, successful revascularization of carotid occlusion with stent implantation immediately followed by intracranial intra-arterial thrombolysis, balloon angioplasty, or thromboaspiration has been reported.9–13 The recent widespread use of self-expanding stents as a thrombectomy device for major embolic occlusions14–16 has led to a new endovascular approach consisting of extracranial angioplasty and stenting followed by intracranial stent-based thrombectomy.17 ,18 We present our recent experience with this endovascular approach in the management of acute tandem occlusive disease.
Material and methods
Participants included consecutive patients with acute ischemic stroke secondary to tandem occlusion of the ICA and middle cerebral artery (MCA) at a single institution (Hadassah-Hebrew University Medical Center) from March 2010 to December 2013. Among the participants in this study, all proximal occlusions were treated by stent-assisted carotid angioplasty and all distal embolic occlusions were managed with self-expanding microstents used as a thrombectomy device (stent-thrombectomy, Solitaire; ev3/Covidien, Plymouth, Minnesota, USA). Patients managed with alternative endovascular or other techniques and those who presented with major intracranial occlusions associated with underlying atherosclerotic stenosis requiring a permanent stent implant were excluded from the study.
Endovascular procedures were performed within 6 h of symptom onset in patients with National Institutes of Health Stroke Scale (NIHSS) score >10 upon presentation to the emergency department where there was no cerebral hemorrhage and no clear sign of early cerebral infarction involving more than one-third of the endangered territory. Tandem occlusion was demonstrated on admission cranial CT angiography and confirmed by digital subtraction angiography (DSA). MR studies were performed for penumbra evaluation only in selected cases (ie, conflicting clinical-neuroradiological findings, unclear stroke onset time) to determine whether there was indication for endovascular revascularization. Comorbidities and current medications were taken into consideration when the therapeutic options were weighed.
Selected clinical, radiographic, and interventional data are presented in table 1. Clinical data included age, admission NIHSS, time to endovascular therapy (defined as interval from stroke onset to arrival in the angiography suite), and modified Rankin Scale (mRS) at 1–3 month follow-up. Radiological data included Alberta Stroke Program Early CT Score (ASPECTS),19 occlusion site, extent of collateral supply on CT angiogram, MR (when available), and post-procedural head CT evaluation. Interventional data included anesthesia type, medications during endovascular treatment, endovascular techniques, time-to-recanalization (TTR, defined as the interval between introducer sheath placement to first angiographic run showing recanalization), Thrombolysis in Myocardial Infarction flow grade (TIMI) at recanalization, and Thrombolysis in Cerebral Infarction (TICI) grade.17 ,18
Demographic, clinical, and procedural data of 24 patients with tandem occlusions of the anterior circulation
Collateral supply was evaluated as good, fair, or poor based on the ratio of the area of parenchyma supplied by collaterals to the total area that should have been supplied by the thrombosed vessel, as assessed by CT, MRI, and/or DSA; good supply was defined as a ratio >66%, fair as 33–66%, and poor as <33%. This classification may be partially correlated with the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology (ASITN/SIR) collateral flow grading system on pretreatment angiography,17 where a good collateral supply corresponds to grade 3–4, fair corresponds to grade 2–3, and poor to 0–1.
Assessment of hemorrhagic transformation (HT) on follow-up CT was performed by an experienced neuroradiologist (JMG). Following established definitions, HT was diagnosed in patients with petechial or confluent hemorrhage within the ischemic lesion. Parenchymal hemorrhage was defined as blood clot in the infarcted area with at least a slight space-occupying effect. Symptomatic intracerebral hemorrhage was defined as any sign of hemorrhage on follow-up imaging associated with a 4-point NIHSS deterioration within 36 h.
Endovascular technique
Every procedure was performed under general anesthesia. A single dose of 2500 units of intravenous heparin was given immediately after achieving femoral access. Diagnostic angiography was performed to confirm the occlusion pattern and collateral supply. Immediately after angiographic confirmation of ICA occlusion and the need for stent implant, patients who were not on antiplatelet therapy received 300 mg aspirin per nasogastric tube.
A 90 cm 8 F guiding catheter (Guider Softip; Boston Scientific, Natick, Massachusetts, USA) was placed at the distal common carotid artery ipsilateral to the occluded ICA. The ICA occlusion was crossed with a Synchro 0.014 inch microguidewire (Boston Scientific) and a Rebar 18 microcatheter (eV3). Angiography was performed through the microcatheter to assess ICA status. Pre-dilation of the cervical occlusion was performed using 2.5/3.0×30 mm balloons and then, if protection was considered necessary, the balloon was exchanged for a distal filter-type protection device (SpiderFX, eV3) that was temporarily deployed beyond the stenosis at a straight prepetrous segment. A closed-cell carotid stent (Wallstent; Boston Scientific/Target) was placed across the stenosis. In selected cases, conservative post-dilation was performed with a 3.5×20 mm balloon.
Carotid angiography was then performed to assess ICA recanalization and determine the precise location and extent of the distal occlusion. The guiding catheter was advanced through the implanted stent with the aid of single or double guidewires or a coaxial catheter, with its tip placed beyond the distal end of the stent. The guiding catheter thus caused subocclusion of the suboptimally expanded stent (the main rationale for conservative post-dilation), allowing a more effective proximal aspiration despite the fact that the guiding catheter is not balloon-tipped. This prevents stent-retriever entrapment in the implanted stent. The guiding catheter was placed distal to the carotid Wallstent, and stent-based thrombectomy proceeded under proximal ICA subocclusion with vigorous suction, as usual.
A final angiogram was performed to assess revascularization of the ICA and its branches. Heparin was not administered after the procedure. Immediate post-procedural CT was obtained to detect hemorrhagic complications or the need for a further surgical procedure. After negative CT, clopidogrel was added to the antiplatelet regime (loading dose 300 mg). Patients were kept under a double regimen of antiplatelet agents for 2 months (clopidogrel 75 mg/day plus aspirin 100 mg/day), and then clopidogrel was discontinued. Aspirin (100 mg/day) was continued indefinitely. The technique is illustrated in figures 1 and 2.

A patient aged >60 years with a history of controlled vascular risk factors was urgently transferred to our center 2.5 h after stroke onset. Upon arrival the patient was alert, with global dysphasia, gaze deviation, and left hemiplegia (National Institutes of Stroke Score (NIHSS) 18). (A–D) Head CT followed by CT angiogram showed no signs of right hemispheric ischemia (Alberta Stroke Program Early CT Score (ASPECTS) 10), with tandem occlusion of the right internal carotid artery (ICA) and proximal middle cerebral artery (MCA). (E) Under general anesthesia, diagnostic angiography confirmed proximal occlusion of the right ICA. A small angiographic spike marked the ICA ostium. The left ICA occlusion was crossed with a microsystem and the angiogram obtained through the microcatheter confirmed its location at the left cervical ICA. The microcatheter was exchanged for a balloon and angioplasty was performed at the proximal left ICA occlusion, achieving partial revascularization. The balloon was exchanged for a protection device and a closed-cell carotid stent was implanted across the plaque. The guiding catheter was advanced beyond the stented segment. (F) Angiography confirmed proximal right MCA occlusion. A 0.021 microcatheter was navigated across the intracranial occlusion. (G,H) Stent-assisted thrombectomy allowed complete recanalization of the MCA after a single pass (Thrombolysis in Myocardial Infarction grade (TIMI) 3, Thrombolysis in Cerebral Infarction grade (TICI) 3). The patient's condition improved, with neurological assessment reaching NIHSS 0 after 1 week.

{kind=link}
{kind=link}
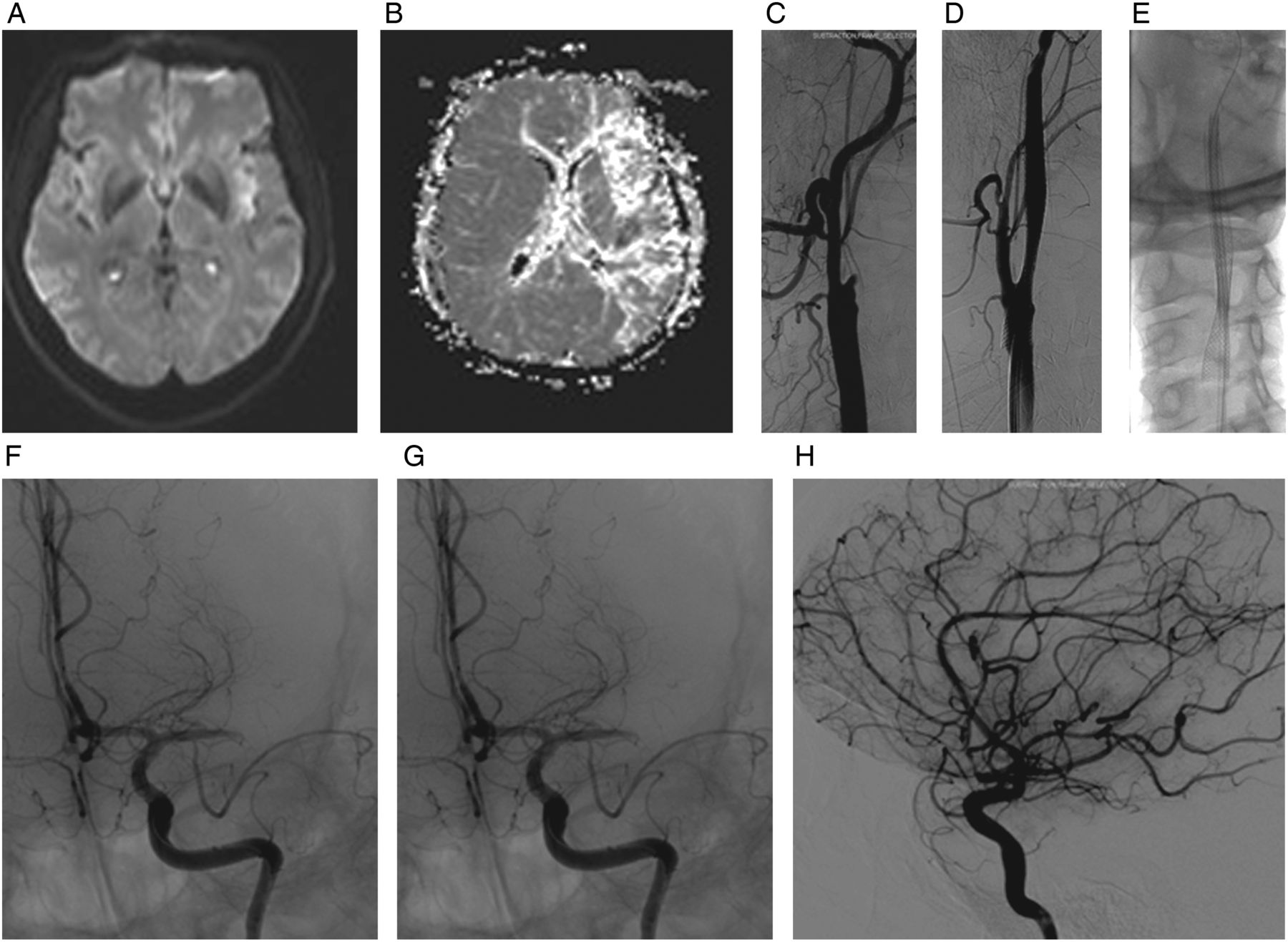
(A,B) A middle-aged patient with a history of multiple poorly controlled vascular risk factors was transferred to our center with a wake-up stroke of unclear onset time. The patient had last been seen well 7 h earlier and was found unconscious on the bedroom floor. Upon arrival the patient was drowsy with global dysphasia and gaze deviation, and presented with right dense hemiplegia NIHSS 24. Head CT followed by CT angiography showed unclear signs of left hemispheric ischemia (ASPECTS 10), with tandem occlusion of the left ICA and proximal MCA Emergency MRI stroke protocol confirmed the presence of a significant diffusion-perfusion mismatch. (C) Under general anesthesia, diagnostic angiography confirmed proximal occlusion of the left ICA. A small angiographic spike marked the ICA ostium. The left ICA occlusion was crossed with a microsystem. Angiogram obtained through the microcatheter confirmed its location at the cervical left ICA. The microcatheter was exchanged for a balloon and angioplasty was performed at the proximal left ICA occlusion. The balloon was exchanged for a protection device and a closed-cell carotid stent was implanted across the plaque. (D) Angiography demonstrates recanalization of the left ICA. (E) The guiding catheter was advanced beyond the stented segment. (F) Angiography confirmed proximal left MCA occlusion. A 0.021 microcatheter was navigated across the intracranial occlusion and stent-assisted thrombectomy was performed. (G,H) In 47 min, after one pass, the left MCA was completely recanalized and reperfused (Thrombolysis in Myocardial Infarction grade 3, Thrombolysis in Cerebral Infarction grade 3). The patient's condition improved, with neurological assessment reaching NIHSS 3 after 1 week.
Results
Overall, 24 patients met the inclusion criteria (4 women and 20 men, mean age 66 years, range 51–77 years). Mean admission NIHSS was 20.4 (median 18, range 14–28) and mean ASPECTS was 9 (range 7–10). Intravenous tissue plasminogen activator (tPA) was administered on admission to 10 patients; two presented further neurological deterioration after thrombolysis. In all other patients the effect of intravenous tPA was considered modest.
Occlusion sites were tandem proximal left ICA and left MCA trunk in 11 patients, tandem right ICA and MCA trunk in six, tandem proximal left ICA and ICA terminus (‘T’) in four, tandem proximal right ICA and ICA ‘T’ in two, and tandem left ICA, MCA, and anterior cerebral artery (triple occlusion) in one case. In all 24 cases the collateral supply was graded as poor (ASITN/SIR collateral flow grading system grade 1–2).
Cervical stenting
Successful stent-assisted cervical ICA recanalization was achieved in all cases. Unprotected pre-angioplasty was routinely performed, with unprotected stenting in 16 patients (67%) and protected stenting in eight (33%). Conservative post-angioplasty was performed in 14 patients (58%) to cross the clot with the guiding catheter. No new embolic event occurred during carotid angioplasty in any patient.
Intracranial thrombectomy
In all patients there was successful intracranial stent deployment across the clot with Solitaire stents (eV3) used as a thrombectomy device for distal clot removal. Complete recanalization was achieved with a single stent pass in 17 patients (71%). A mean of 1.6 thrombectomy attempts was needed to achieve removal of the distal clot (range 1–5). Complete recanalization with complete perfusion (TIMI 3, TICI 3/2b) was achieved in 19 patients (79%), complete recanalization with partial perfusion (TIMI 3, TICI 2A) was achieved in three (13%), and partial recanalization with partial perfusion (TIMI 2, TICI 2A) was obtained in two (8%). The mean time to therapy was 3.8 h (range 2–5.5). The mean TTR was 51 min (range 38–69 min). No intracranial self-expanding stent was permanently implanted. No arterial dissection, arterial rupture or accidental stent detachment occurred.
CT findings
Routine CT scans performed after recanalization in 18/24 patients (75%) demonstrated cortical sparing (>80% of cortex at risk). This is particularly remarkable considering that patients in this series presented with very limited collateral flow at admission angiography. Lenticulostriate/subinsular residual infarct (volume 0.8–9 cm3) was noted in 19/24 patients (79.2%). No patient required decompressive craniectomy for mass effect or infarction. Six patients had petechial hemorrhages; none presented with intracerebral or intraventricular hemorrhage. The sample size and low rates of hemorrhage precluded analysis of the effect of intravenous tPA or antiplatelet loading dose administration.
Sonographic findings
None of the 20 patients with follow-up Doppler examination had stent occlusion. Four patients with known post-angioplasty residual stenosis (>30%) were followed more closely and remain asymptomatic; one patient with stenosis progression on sonographic and angiographic follow-up sustained uneventful re-angioplasty 4 months after primary treatment.
Clinical outcome
Rapid neurological recovery (NIHSS <6 on day 7) was achieved in 14/24 patients (58%). Two patients died (8%); one elderly patient died during hospitalization due to infectious complications and a second elderly patient died from suspected cardiovascular causes 9 weeks after endovascular treatment during inpatient rehabilitation. Among the 22 surviving patients, 17 (77%) were examined at 3-month follow-up. Of these, 13/17 (76%) had good neurological evolution reaching mRS 0–2 and 4/17 (24%) achieved mRS 3. At 6-month follow-up, mRS was obtained for 20 patients at a scheduled hospital visit or by telephone follow-up; 14/20 (70%) had mRS 0–2 and 6/20 (30%) had mRS 3. Two patients have not reached 6-month follow-up. There were readmissions for a new cerebrovascular (n=2) or cardiovascular event (n=2) in 4/24 patients (17%). Neither of the two new strokes occurred on the treated territory and stents from the primary procedure were found patent in all four patients.
Discussion
Mechanical thrombectomy aims to achieve rapid clot removal by means of different devices instead of the slow pharmacological disintegration of the embolic material after intra-arterial injection. The recent introduction of stent-based thrombectomy has revolutionized the endovascular revascularization of acute large vessel occlusion, with marked improvement in both time and rate of recanalization.15 ,19–22 Until stent-retrievers were introduced into common practice, endovascular management of tandem occlusions was complex, only partially effective, hazardous, and time-consuming.10–13
In this report, we present a case series of 24 patients with acute anterior circulation tandem occlusions treated exclusively with proximal stent-assisted angioplasty immediately followed by stent-based thrombectomy. Our preliminary data on this group of 24 patients suggest that angioplasty and stenting of the proximal occlusion followed by intracranial intervention may be feasible, efficacious, and safe, and may likely be associated with higher rates of recanalization and better rates of good functional outcome compared with intravenous thrombolysis or even other endovascular approaches.2 ,10–13 ,23
Recently, Mpotsaris et al18 also concluded that the extracranial Wallstent/intracranial stent-retriever approach was safe and led to improved neurological outcome in patients with a poor prognosis under intravenous tPA treatment alone.
In our series, angioplasty and stenting of the acute ICA origin occlusion was performed with high technical success. One of the most challenging technical steps when dealing with tandem occlusion is catheterization of the true lumen of the occluded ICA.24 Small subtle angiographic signs may indicate the optimal point of entry to the true arterial lumen, as shown in figures 1E and 2C. We agree with Malik et al12 that the feasibility of passing a microguidewire across this occlusive lesion in a high proportion of cases reflects a similar situation to that demonstrated in acute coronary syndromes, where vessel occlusion often represents thrombus formation associated with rupture of a pre-existing plaque of underlying non-critical stenosis.25 In our experience, most acutely occlusive lesions of the ICA represent focal atherosclerotic lesions with superimposed fresh soft thrombus, resulting in relatively easy passage of a microguidewire through the lesion, limited resistance to pre-angioplasty, and the need for a tight-meshed stent in order to adequately jail the friable plaque/clot. This is also the main argument favoring extracranial stenting followed by stent thrombectomy (antegrade approach) instead of thrombectomy followed by extracranial stenting (reverse approach).17
This novel approach, although more demanding than the regular procedure performed for a single occlusion, has proved to be reasonably fast, with a mean time to recanalization of 51 min (range 38–69 min). Extracranial carotid recanalization was achieved in every case, and complete recanalization with perfusion (TIMI 3, TICI 3/2b) was achieved in four out of five patients, with partial recanalization achieved in the remaining 20%. These rates are comparable to the recanalization rates achieved in patients with isolated proximal MCA occlusions treated by stent-retrievers.24 ,26 ,27 Good clinical prognosis and low rates of hemorrhagic complications are also comparable among patients with tandem and single occlusions, supporting the fact that, with this approach, both groups have a similar prognosis.
Recently, Stampfl et al28 presented a series of 24 patients who sustained cervical ICA stenting after stenosis or occlusion, followed by intracranial thrombectomy. Their endovascular approach was similar (not identical) to ours, but they reported substantially higher rates of cerebral hemorrhagic complications. Symptomatic intracranial hemorrhage occurred in 4/24 patients (16.6%); three of them had received tirofiban and one had received a loading dose of aspirin and clopidogrel. Hemorrhage was fatal in one patient. Although the reasons are unclear, this may be related to the use of intravenous thrombolysis before thrombectomy in most of their patients (22/24) and the concomitant use of glycoprotein IIb/IIIa receptor antagonist (started before stent implant and maintained for 24–48 h) instead of our more conservative scheme.
This report provides pilot data for a subsequent study on tandem ICA–MCA occlusions treated with stent-based techniques. Our encouraging preliminary results await confirmation from further experience and prospective randomized studies.
Acknowledgments
The authors wish to thank Shifra Fraifeld, Senior Medical Writer and Head of Research Support in the Departments of Neurosurgery and Radiology at the Hadassah-University Medical Center, for her editorial assistance in the preparation of this manuscript.
References
Footnotes
-
Contributors All authors made a significant contribution to the study and to manuscript preparation. JEC, JMG, RRL and EI contributed to study conception and design, JEC, JMG, GR and RE contributed to data acquisition, and JEC and RRL contributed to data interpretation and analysis. JEC and JMG drafted the manuscript, JEC, RRL, RE and GR critically revised the paper, and EI contributed significantly to the intellectual content. JEC, JMG, GR, EI, RE and RRL approved the final version of the manuscript.
-
Competing interests None.
-
Ethics approval This retrospective analysis was conducted with approval of the Hadassah-Hebrew University Institutional Review Board (0003-12-HMO).
-
Patient consent Informed consent for the study was waived; however, patients or a family member gave informed consent for the endovascular procedure.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Questions regarding details not seen in the manuscript should be addressed to Professor Jose E Cohen, the corresponding author, who maintains the clinical research files for neuroendovascular procedures.