Article Text

Abstract
Introduction Reports of the limitations and feasibility of balloon remodeling for treatment of complex anterior communicating artery (ACoA) aneurysms are scarce.
Methods Ninety-nine patients were treated with balloon-assisted coil embolization for ACoA aneurysms between August 2004 and October 2012. Records were reviewed for aneurysm characteristics, balloon trajectory (vessel and side), bilateral access, treatment-related complications, and aneurysm recurrence determined by magnetic resonance angiography (MRA). Morphological outcomes following treatment were categorized into Raymond class I, II, or III.
Results Fifty-three aneurysms (53.5%) were unruptured and 46 (46.4%) were ruptured. Aneurysmal occlusion (Raymond I or II) was achieved in 89 patients (89.9%); three (3.0%) were incompletely embolized and treatment was aborted in six (6.1%). Balloon trajectories were from the A1 to either the ipsilateral or contralateral A2. In 17 cases (17.2%), bilateral A1 access was used to achieve balloon protection of the contralateral A2. In four cases (4.0%), balloon remodeling was aborted due to technical difficulty. There were 15 (15.2%) treatment-related complications; five (5.1%) were intraoperative ruptures, one of which resulted in a neurological deficit and another in death. All other complications were clinically silent, producing a permanent complication rate of 2.0%. Mean radiographic follow-up was 2.5 years, and six patients (6.1%) were retreated for recurrence or known remnant.
Conclusions Balloon remodeling should be considered for broad-based complex ACoA aneurysms. This technique provides a high rate of aneurysm occlusion with an acceptable complication profile, and avoids the need for dual antiplatelet therapy. The balloon trajectory will depend on aneurysm morphology and bilateral access may be useful in selected cases.
- Aneurysm
- Flow Diverter
- Cranial nerve
- Coil
- Angiography
Statistics from Altmetric.com
Introduction
Anterior communicating artery (ACoA) aneurysms are the most common intracranial aneurysms and are responsible for nearly 40% of cases of aneurysmal subarachnoid hemorrhage (SAH).1–3 The complexities of these lesions often include wide necks, involvement of perforators and the A2 segment of the anterior cerebral artery (ACA), variable dome projection, and anatomic anomalies or variants. As a result of these characteristics, treatment of these lesions by microsurgical clipping or endovascular coil embolization is often difficult and can carry a higher risk of treatment-related morbidity.
Balloon remodeling for the endovascular treatment of complex wide-necked aneurysms has evolved over the past two decades. With recent trials demonstrating equipoise in reported intraprocedural complication rates when compared with primary coil embolization, its indications have expanded to more anatomically complex lesions including bifurcation aneurysms.4 ,5 However, remodeling has traditionally been employed less frequently in ACA and ACoA aneurysms, partially due to difficulty of navigation with first-generation balloons. As a result, few series exist reporting the use of this adjunctive technique for these lesions.
To further delineate patient subsets that may benefit most from this technique, we report our experience with balloon remodeling in the treatment of complex ACoA aneurysms. In doing so, we set out to describe technical nuances unique to remodeling in this region, as well as to report complication rates from our institutional experience.
Methods and materials
We reviewed a prospectively maintained endovascular database at the Barrow Neurological Institute for patients who have undergone balloon-assisted coil embolization from August of 2004 to October of 2012 after obtaining Institutional Review Board approval. General anesthesia with neurophysiologic monitoring was used in all cases. Records were reviewed for balloon trajectory (vessel and side), bilateral access, treatment-related complications, and aneurysm recurrence determined by magnetic resonance angiography (MRA). Aneurysm characteristics recorded included size, rupture status, and time to recurrence. Endovascular treatment was categorized as ‘complete’ or ‘near-complete’ in cases with a small neck remnant (Raymond class I or II) and ‘incomplete’ if significant post-treatment residual contrast filling was observed (Raymond class III). All patients with asymptomatic coil herniation into the parent vessel were maintained on a 6-week course of aspirin after the procedure.
All patients with non-ruptured aneurysms were systemically heparinized to maintain activated clotting time >200 s throughout the procedure. For ruptured aneurysms, heparinization was instituted either prior to catheter exchange or following placement of the first coil. The decision to use balloon-assisted coil embolization was made by the primary endovascular surgeon at the time of treatment, depending on morphological characteristics. Aneurysms with a favorable neck-to-dome ratio and/or difficult balloon catheter access were treated with primary coil embolization. All others were treated with a balloon in place. All patients harboring a ruptured or unruptured ACoA aneurysm were given the option of treatment by either of the modalities. Patients included in this study consented to endovascular treatment only after a comprehensive discussion of the risks and benefits of each. All procedures were performed using a HyperForm or HyperGlide balloon (ev3, Irvine, California, USA) measuring 4 mm in widest diameter and 7–20 mm in length.
Radiographic follow-up was performed using MRI/MRA at 3, 6, 12, and 24 months. The development of a new significant neck residual greater than 3 mm or any contrast filling within the aneurysm dome were indications for retreatment. In addition, an increase in size of any previously stable residual dome or neck prompted retreatment.
Results
There were 99 patients with ACoA aneurysms where balloon remodeling was attempted and/or used during the study period (49 men and 50 women). The mean age of the patient subset was 61.2 years (range 24–84). Average aneurysm size treated was 6.5 mm. Fifty-three lesions (53.3%) were unruptured and 46 (46.4%) were ruptured. Of the 99 patients, balloon remodeling was aborted in nine (table 1); three underwent primary coil embolization (3.0%), five were referred for microsurgical clipping (5.1%), and one underwent stent-assisted coil embolization (1.0%). Of the remaining 90 patients, complete or near-complete occlusion (Raymond class I or II) was achieved in 87 lesions (96.7%). Residual aneurysms (Raymond class III) were observed in three cases (3.3%).
Outcomes of balloon remodeling for treatment of anterior communicating artery aneurysms at Barrow Neurological Institute
A variety of catheter trajectories were used, depending on the morphology of the aneurysm and parent vessel complex. Of the cases in which balloon access and remodeling were successful, 58 cases (64.4%) used a contralateral balloon trajectory from an A1 to a contralateral A2 segment vessel for coverage of the aneurysm neck. In 31 cases (34.4%), an ipsilateral trajectory was used. In one case, two balloons were used to achieve bilateral protection of the lesion and parent vessels (see illustrative case). Of the entire series, 13 cases (13.1%) required bilateral femoral artery access. This enabled both simultaneous bilateral carotid injections, allowing for full visualization of the ACA and ACoA complex, and bilateral microcatheter access to the ACoA.
Treatment-related complications were observed in 15 cases (15.2%, table 2). Thirteen were clinically silent and two resulted in permanent morbidity or mortality. Of the latter, one resulted in an ACA distribution stroke and the other resulted in death; both were secondary to intraprocedural rupture of a parent artery and subsequent glue embolization and sacrifice of an A2 vessel. Follow-up was performed using MRA imaging exclusively, with average follow-up time of 20.4 months (range 2–72 months). During the study period, eight patients (8.1%) underwent retreatment, six for recurrence (6.1%) and two for a known residual that was observed to grow (2.1%). The mean time to recurrence was 21.2 months (range 2–72 months).
Treatment-related complications
Illustrative cases
Case 1
A 52-year-old man was found unresponsive and brought to the Barrow Neurological Institute where he was clinically noted to be Hunt–Hess grade 5 with a Fisher grade 4 SAH. Imaging revealed a ruptured superiorly-projecting ACoA aneurysm measuring 7×6 mm, with an anomalous A2 complex demonstrating two A2 branches originating from the base of the aneurysm from the left, along with a normal right A2 (figure 1). Digital subtraction angiography demonstrated filling of the aneurysm and the anomalous left A2 branches only from the left internal carotid artery (LICA) and therefore bilateral groin access was obtained for full visualization of the ACA and ACoA complex (figure 2). The neck of the aneurysm was measured to be 4.3 mm. Given the anomalous A2 branches originating from the base of the lesion along with the size of the neck, two 4×7 mm HyperForm balloons were used for protection of the parent vessel, one in each anomalous A2 on the left (figures 3 and 4). Coil embolization was carried out without complication. Post-embolization angiography demonstrated obliteration of the lesion and patency of the anomalous left A2 branches (figure 5).
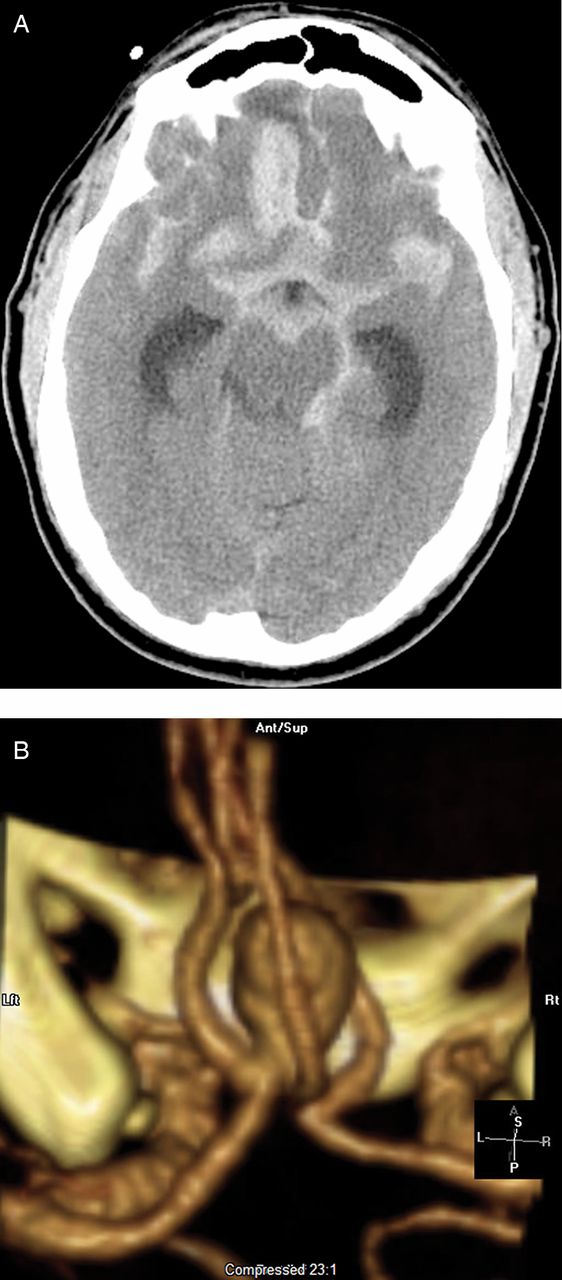
CT and CT angiography (CTA) of the head. (A) Axial CT without contrast demonstrating Fisher grade 4 subarachnoid hemorrhage. (B) CTA three-dimensional reconstruction of a ruptured anterior communicating artery aneurysm with anomalous dual-origin A2 segment vessels originating from the left and a normal A2 on the right. Reproduced with permission from Barrow Neurological Institute.

Three-dimensional digital subtraction angiography of a left internal carotid artery injection demonstrating filling of a complex anterior communicating artery aneurysm measuring 7×6 mm, with two left-sided A2 segments. Reproduced with permission from Barrow Neurological Institute.

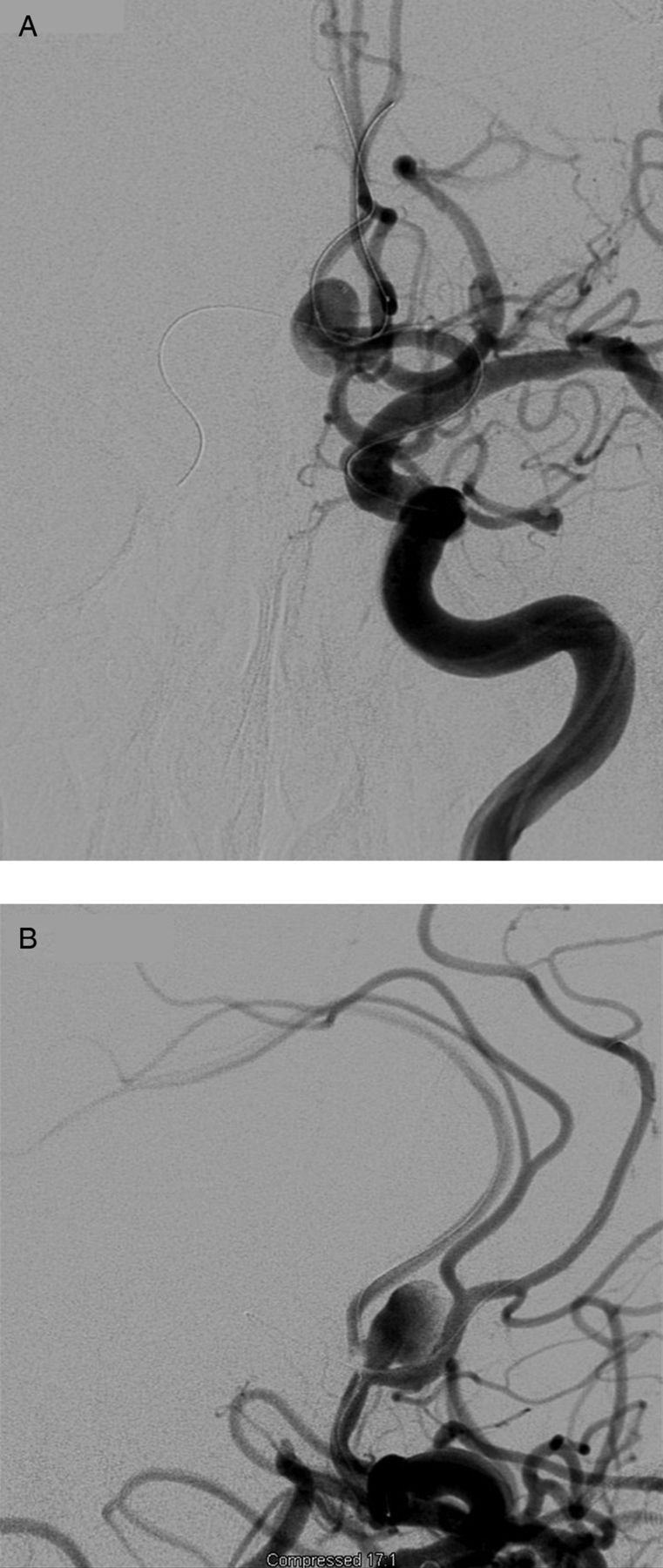
Unsubtracted angiography and digital subtraction angiography. (A) Working angle projection in A-plane, left internal carotid artery (LICA) injection, demonstrating bilateral balloon catheter distal purchase in both anomalous left A2 segments. (B) Working angle projection in B-plane, LICA injection, demonstrating bilateral balloon catheter distal purchase in both anomalous left A2 segments. Reproduced with permission from Barrow Neurological Institute.

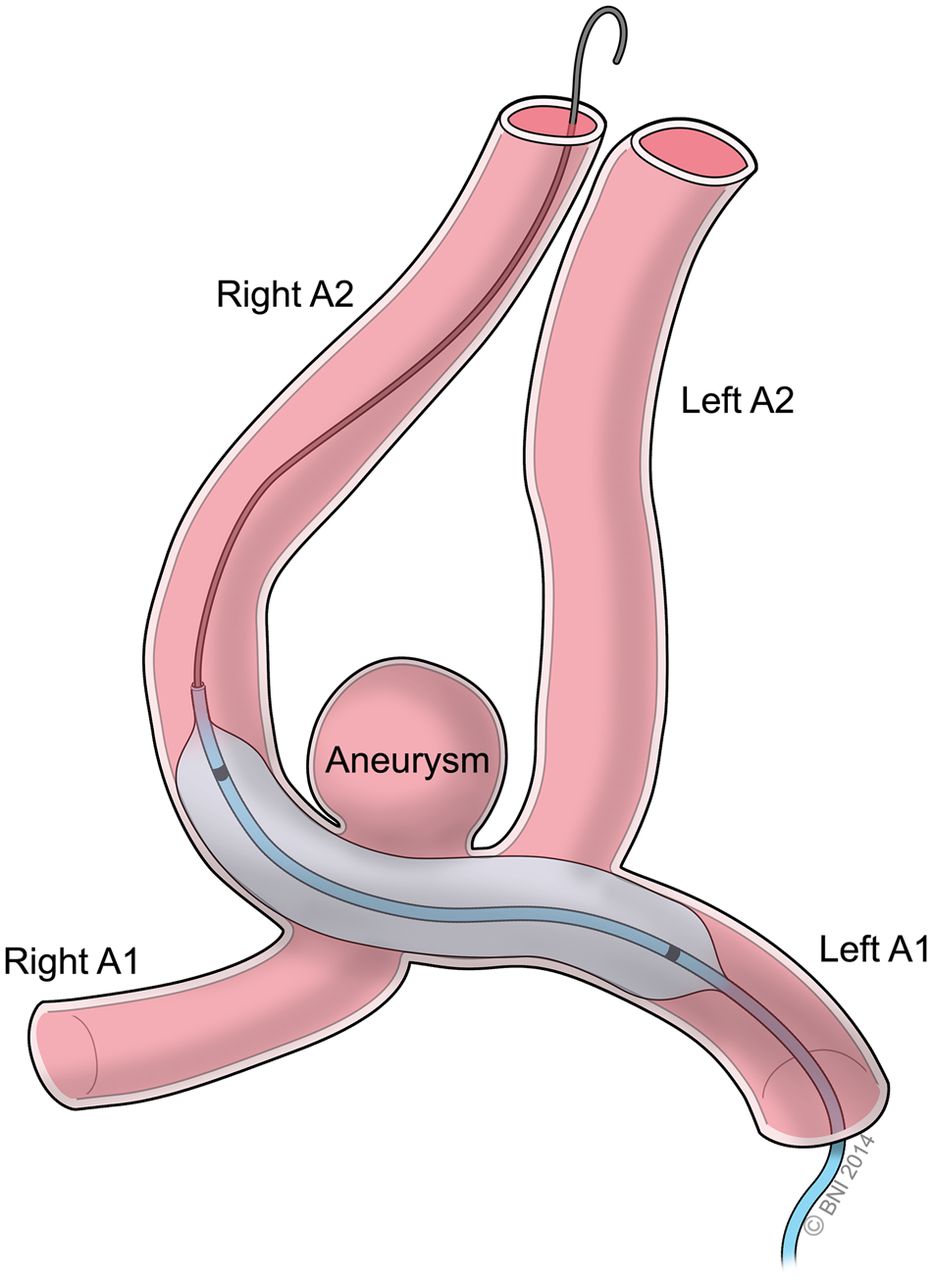
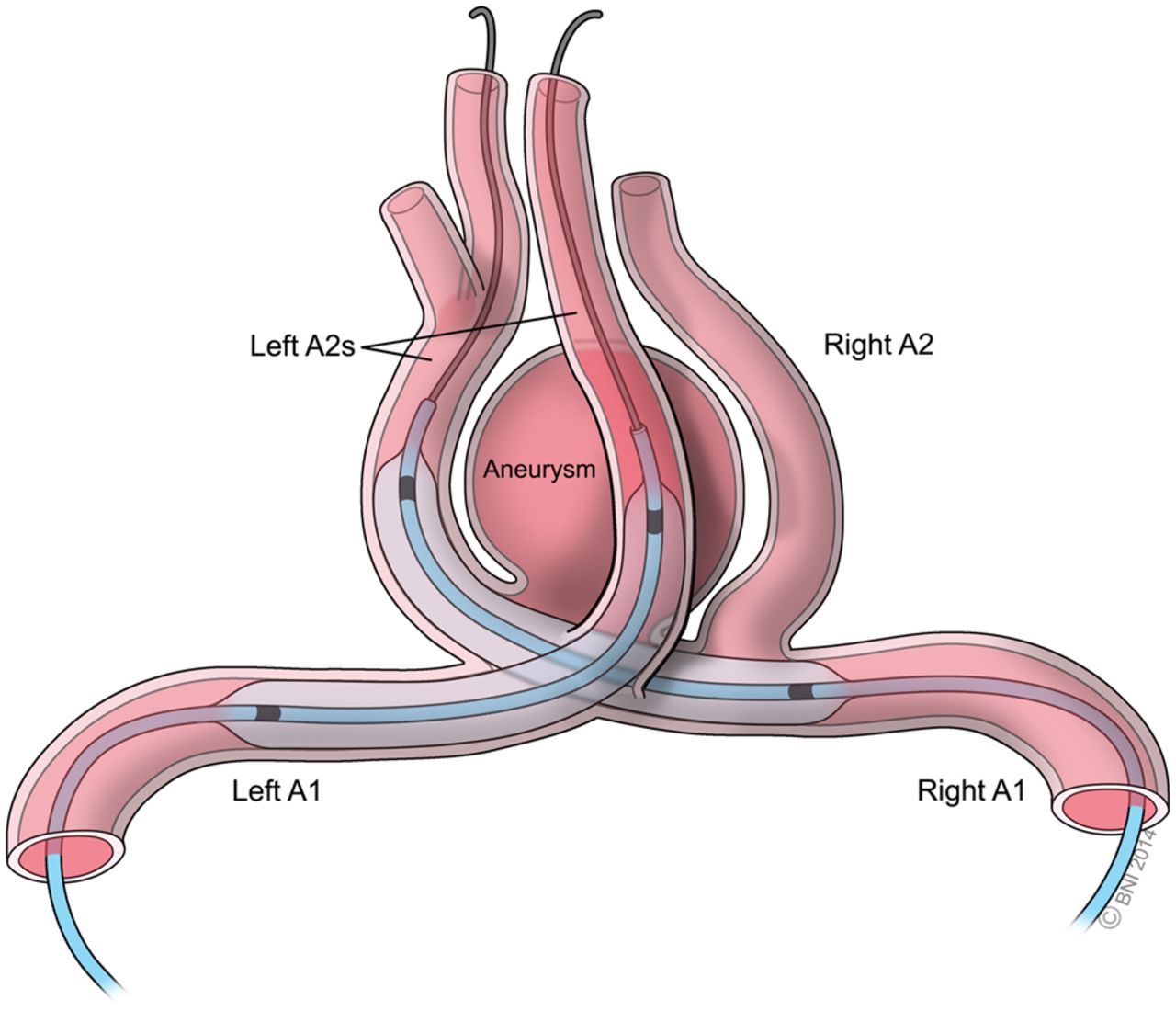
Balloon remodeling technique using two crossing balloons from bilateral A1 branches to an anomalous left A2 complex. Reproduced with permission from Barrow Neurological Institute.

Digital subtraction angiography. Working angle projection in A-plane, left internal carotid artery injection, demonstrating obliteration of the aneurysm after treatment. Reproduced with permission from Barrow Neurological Institute.
Case 2
A 69-year-old man was incidentally found to have an inferiorly-projecting ACoA aneurysm measuring 6×6 mm (figure 6). He was initially evaluated for microsurgical clipping but referred for endovascular treatment after being found to be a poor surgical candidate secondary to medical comorbidities. Digital subtraction angiography demonstrated filling of the lesion and bilateral A2 branches from a right internal carotid artery (RICA) injection. A 4×15 mm HyperGlide balloon was used for protection of the parent vessel with an ipsilateral trajectory from the right A1 to the right A2 (figures 7 and 8). Coil embolization was carried out and post-embolization angiography demonstrated obliteration of the lesion with patency of all branch vessels (figure 9). A small coil loop herniation into the parent vessel was noted and the patient was maintained on a 6-week course of aspirin 325 mg daily without complication.

Three-dimensional digital subtraction angiography of a right internal carotid artery injection demonstrating filling of an inferiorly-projecting anterior communicating artery aneurysm measuring 6×6 mm. Reproduced with permission from Barrow Neurological Institute.

Unsubtracted angiography and digital subtraction angiography. Working angle projection in A-plane, right internal carotid artery injection, demonstrating balloon catheter trajectory from the right A1 to the ipsilateral A2. Reproduced with permission from Barrow Neurological Institute.

Balloon remodeling technique using an ipsilateral trajectory from the right A1 to the right A2. Reproduced with permission from Barrow Neurological Institute.

Digital subtraction angiography. Working angle projection in A-plane, right internal carotid artery injection, demonstrating obliteration of the aneurysm post-treatment. Reproduced with permission from Barrow Neurological Institute.
Case 3
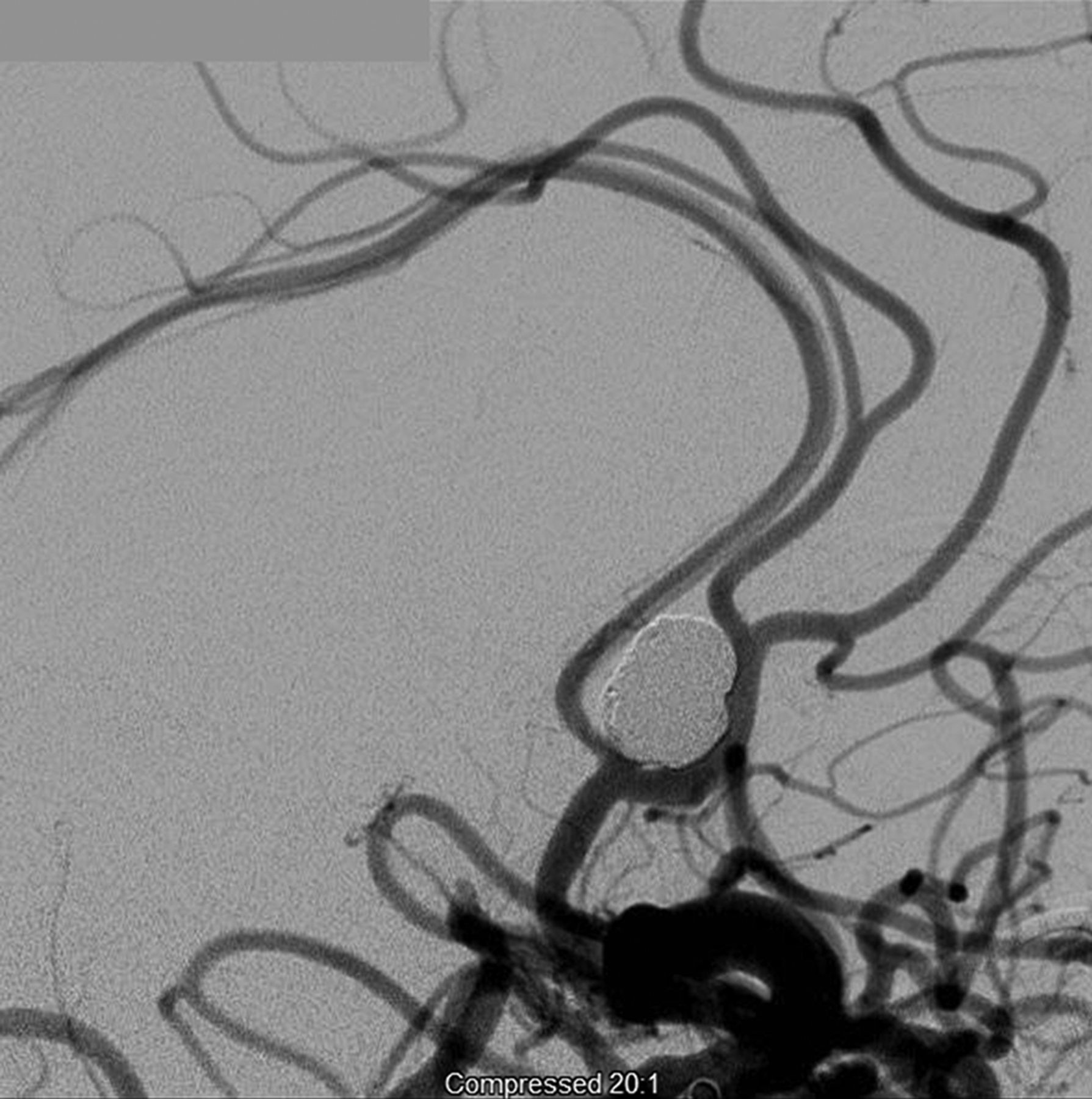
A 59-year-old man was found to have a 4×5 mm superiorly-projecting ACoA aneurysm on investigation for vertigo (figure 10). A 4×7 mm HyperForm balloon was used with a contralateral trajectory from the left A1 to the right A2 (figure 11). Coil embolization was carried out and post-embolization angiography demonstrated obliteration of the aneurysm dome (figure 12).

Three-dimensional digital subtraction angiography of a left internal carotid artery injection demonstrating filling of a superiorly-projecting anterior communicating artery aneurysm measuring 4×5 mm. Reproduced with permission from Barrow Neurological Institute.
Balloon remodeling technique using a contralateral trajectory from the left A1 to the right A2. Reproduced with permission from Barrow Neurological Institute.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Digital subtraction angiography. (A) Working angle projection in A-plane, left internal carotid artery (LICA) injection, demonstrating balloon catheter trajectory from the left A1 to the contralateral A2. (B) Working angle projection in A-plane, LICA injection, demonstrating obliteration of the aneurysm post-treatment. Reproduced with permission from Barrow Neurological Institute.
Discussion
ACoA aneurysms are often complex and difficult lesions to treat because of their morphology, including wide necks, variable dome projection, the presence of critical perforators in the region of the aneurysm neck, and associated vascular anomalies or variants. The impact of morphological characteristics of ACoA aneurysms on treatment outcomes has been studied. Neck location on the ACoA and posterior dome projection were among several anatomic factors associated with aneurysm recanalization in a recent model.6 Vessel occlusion was seen to be significantly higher for superiorly or posteriorly projecting lesions in microsurgically treated patients when compared with other orientations in both clipped and coiled patients.7
Balloon remodeling for wide-necked aneurysms was first described by Moret et al8 in 1994. There are few data for balloon remodeling for coil embolization of ACA and ACoA aneurysms, primarily because the remodeling technique has historically been used less frequently in these locations compared with other lesions. While navigation of the ACA and ACoA complex was relatively difficult with the first generations of balloon catheters, advances in technology and technique have made it easier and safer. Additionally, obliteration rates for balloon-assisted coiling have varied, depending on the location of the lesion. Results have varied from institution to institution, probably as a result of differing treatment paradigms for complex lesions and study methodology. The results of this series demonstrate a high obliteration rate for these lesions when assisted by balloon remodeling.
Our experience has helped delineate some of the technical nuances of balloon remodeling for aneurysms of this complex region. As with primary coil embolization, bilateral access is often helpful and sometimes required for full visualization of the ACA and ACoA complex, including bilateral A2 arteries, and for navigation of the balloon catheter. Ipsilateral and contralateral trajectories for the balloon catheter can be used; in our series, both trajectories were used almost equally. While sidewall aneurysms can traditionally be remodeled without difficulty by inflating the balloon in the parent vessel directly across the aneurysm neck, the morphology of ACoA lesions in conjunction with variable A2 take-offs can make balloon catheter navigation and placement much more complex. As with balloon remodeling of bifurcation aneurysms, two balloons can also safely be used, as we demonstrated in one case of a wide-necked lesion with complex A2 anatomy. In many cases these techniques have made possible the endovascular treatment of complex ACoA aneurysms where primary coil embolization may not have previously been possible.
Finally, inflation of the balloon can also help with stabilization of the coiling microcatheter during coil deployment. This, in turn, can aid in achieving a more dense packing, thereby minimizing the risk of coil compaction in wide-necked aneurysms. While it is likely that this has a significant impact on the durability of treatment, predictors of retreatment are difficult to ascertain from institutional series due to variability in classification of coil density and residual filling. In addition, the complexity of lesions requiring remodeling may diminish the added benefit of balloon remodeling. Likewise, some series suggest higher rates of retreatment in lesions treated with balloon remodeling, despite the knowledge that there is a relationship between coil mass attenuation and rates of recanalization.9–12 While the current study does not include a comparison group of lesions treated with primarily coil embolization, we have demonstrated that, with judicious use of balloons for lesions in this location, only 6.1% required retreatment at a mean follow-up of 2.5 years. This remains lower than the rates of retreatment following primary coil embolization and balloon remodeling in the literature, which range from 9% to 17%.6 ,10
While we used exclusively single-lumen balloons navigated over a 0.010 wire, more recently designed double-lumen balloons such as Scepter C (MicroVention, Tustin, California, USA) and Ascent (Micrus, San Jose, California, USA) that are navigated over a 0.014 wire may facilitate balloon navigation to the ACA and across the ACoA complex. Our decision to use a HyperGlide versus HyperForm balloon was primarily dependent on the morphology of the aneurysm neck, as well as its relationship to the parent vessel. For approaches to the ipsilateral A1–A2 junction, a HyperGlide balloon will often suffice for protection of the parent vessel with an ipsilateral trajectory. When additional compliance is necessary, most notably in cases of a contralateral trajectory, a HyperForm balloon is often preferable due to its ability to herniate into the neck of the aneurysm while protecting the contralateral A1–A2 junction. As an alternative to balloon remodeling, stent-assisted coiling can be used for complex lesions. However, a significant disadvantage of stent use is the need for antiplatelet therapy. While the treatment of unruptured aneurysms carries a lower risk of intracranial and extracranial hemorrhagic complications with antiplatelet therapy and anticoagulation than ruptured lesions, avoidance of antiplatelet therapy remains preferable, especially in light of patient compliance issues.
While some anterior circulation aneurysms, such as middle cerebral artery lesions, have traditionally been more amenable to microsurgical clip occlusion, ACoA aneurysms often represent equipoise. As with all intracranial aneurysms, all patients in this cohort were given the option of microsurgical clip occlusion and informed of risks and benefits of both modalities. In general, aneurysm morphology may dictate treatment paradigm. Posteriorly projecting lesions may complicate microsurgical approaches and increase the risk of perforator injury.7 Additionally, advanced age, poor SAH grade, extensive parenchymal edema, and risk of cerebral vasospasm with vessel manipulation in mid-to-late SAH presentation may all be factors that favor endovascular therapy.
Our results suggest that the complication profile for balloon remodeling of lesions in this location is comparable to or lower than most series of balloon remodeling for all aneurysms. While earlier data suggested that the use of the balloon remodeling technique for all intracranial aneurysms was associated with higher intraprocedural complication rates, recent prospective trials have demonstrated similar rates of complications between balloon remodeling and primary coil embolization.4 ,5 Reported rates of thromboembolic events, including those that remained clinically silent, range from 5.4% to 14% in the literature for both ruptured and unruptured lesions.4 ,5 ,9 ,10 ,13 ,14 Additionally, the rates of intraoperative rupture range from 1.7% to 4.4% in the literature for both ruptured and unruptured lesions.4 ,5 ,9 ,10 ,14 Given that inflation of the positioned balloon can be helpful in the event of intraprocedural rupture, a recent series found fewer patients with neurological worsening following a rupture when balloon assistance was used.15 In addition, coil herniation into the parent vessel, while often clinically silent, can precipitate thromboembolic events. Balloon protection of the parent vessel can often mitigate this risk during coil deployment.
Conclusion
Balloon remodeling is a valuable adjunctive technique in the endovascular treatment of complex and wide-necked ACoA aneurysms. It is technically feasible with a high rate of obliteration and is safe, with a complication profile comparable to that of primary coil embolization. Technical nuances vary depending on the morphology of the aneurysm and parent vessel.
Acknowledgments
The authors wish to thank Clare Prendergast for providing technical support for this manuscript.
References
Footnotes
-
Funding No external funding was received or used for this study.
-
Contributors KM, FCA, AFD, RWC, and CGMcD are responsible for the conception and design of this work. KM and AFD were the primary data gatherers. Data interpretation and analysis was performed by KM and AFD. The article was drafted by KM and AFD. FCA, AFD, and CGMcD critically revised the article; all authors approve the final version of the manuscript. The study was supervised by FCA and CGMcD. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.