Article Text

Abstract
Background Artificial stroke models can be used for testing various thrombectomy devices.
Objective To determine the value of combined stentriever–aspiration thrombectomy compared with the stentriever-alone approach.
Methods We designed an in vitro model of the intracranial circulation with a focus on the middle cerebral artery (MCA) that closely resembles the human intracranial circulation. After introducing fresh clot in the MCA, we used conventional biplane angiography and microangiographic fluoroscopy to compare recanalization rates and occurrence of emboli in new, unaffected territory for thrombectomy approaches in which a stentriever (Solitaire flow restoration stentriever, Covidien) was used alone or in combination with continuous manual aspiration through a Navien catheter (Covidien).
Results In a total of 22 experiments (11 for each approach), successful clot delivery to the MCA was achieved in all cases. Successful angiographic recanalization (thrombolysis in cerebral infarction score of 2b–3) was achieved more frequently with the combined stentriever–aspiration approach than with the stentriever-alone approach (in 10 vs 4 experiments, p=0.023). Emboli in new territory occurred in three experiments with the stentriever-alone approach, and none were seen with the combined approach (p=0.21).
Conclusions The combined stentriever–aspiration approach to thrombectomy leads to better angiographic recanalization rates than use of the stentriever alone. Further experiments are needed to test the value of balloon-guide catheters and aspiration performed using other types of catheters and modes of aspiration.
- Stroke
- Thrombectomy
- Technique
Statistics from Altmetric.com
Introduction
Stentrievers are the most recent class of stroke thrombectomy devices approved by the Food and Drug Administration (FDA) for recanalization of occluded cerebral vessels in patients with acute ischemic stroke. Post-FDA approval experience shows that stentrievers are often used in clinical practice in conjunction with other endovascular approaches, of which combined aspiration plus stentriever thrombectomy is used most commonly.1–4 Stentriever thrombectomy under continuous aspiration is believed to prevent distal embolization and improve recanalization rates; however, direct evidence to support this presumption is lacking.
Previous investigators have shown the effectiveness of artificial stroke models in testing various thrombectomy devices.5–8 Here, we present a new stroke model that closely resembles the intracranial circulation with a robust collateral supply and demonstrate its usefulness in evaluating primary stentriever versus combined stentriever–aspiration thrombectomy approaches to stroke, particularly in relationship to recanalization rates as measured by the Thrombolysis in Cerebral Infarction (TICI) revascularization scale, and detecting embolization in unaffected territories.9
Methods
Model anatomy
The collection of clinical data for this study was approved by our local institutional review board. Using intracranial CT angiograms of subjects with normal anatomy from an anonymized patient library, a three-dimensional (3D) model of the intracranial circulation was generated in STereoLithography (STL) file format using a 3D workstation (Vitrea, Vital Images, Minneapolis, Minnesota, USA). Free mesh-manipulation software (MeshMixer, Autodesk, Inc10) was used to create a segmented geometric model of the intracranial circulation, with a focus on the middle cerebral artery (MCA).
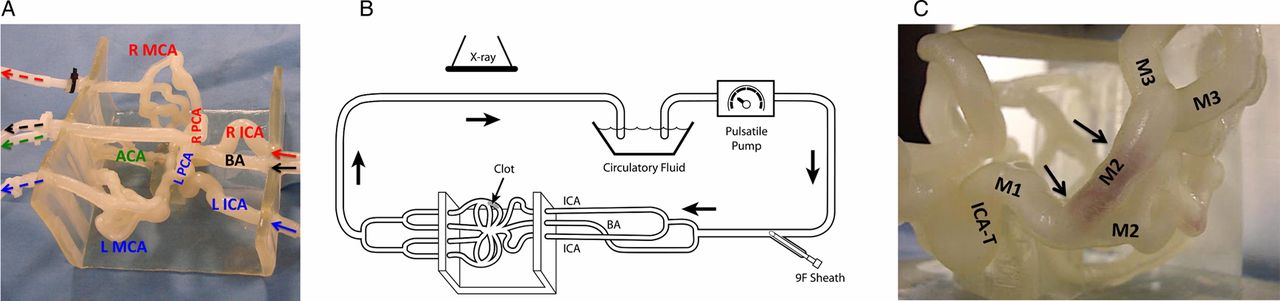
The MCA was chosen as the primary focus of the model (figure 1A) because it is the most common anatomical target for intra-arterial thrombectomy. The model was manipulated by trimming smaller branches to simplify the geometry. The model consisted of three separate inflow channels mimicking the basilar artery and the two intracranial internal carotid artery (ICA) branches. The right and left MCA branches included M1–M4 segments with smallest vessels of 1 mm in diameter (figure 2). The design included bilateral A1 anterior cerebral artery segments connected to a single anterior cerebral artery and a single posterior communicating artery (right side), allowing near-complete circle of Willis circulation. To maintain stability of the model and preserve the venous outflow, vessels representing the distal intracranial anterior circulation were merged into closed loops with separate outflow channels. Each MCA, the anterior cerebral artery, and the basilar artery had a separate venous outflow channel.

Intracranial circulation stroke model. (A) The model consists of three separate inflow channels (arrows) for the left internal carotid artery (L ICA), right internal carotid artery (R ICA), and the basilar artery (BA). The right and left middle cerebral artery (MCA) branches (R MCA, L MCA), the anterior cerebral artery (ACA), and the left and right posterior cerebral artery (L PCA, R PCA) P1 segments have separate outflow channels (dashed arrows). (B) Schematic representation of the clot model. The model contains separate inflow and outflow channels and is connected to a pulsatile pump via a closed circuit. Arrows indicate direction of flow. A 9 F sheath allows the introduction of guide catheters and thrombectomy devices. Biplane angiography and microangiographic fluoroscopy is used during thrombectomy experiments. (C) Higher magnification of the model with a clot located within the M2 segment of the MCA (arrows). ICA-T, internal carotid artery terminus; M1, M1 MCA segment; M3, M3 MCA segment.

Angiographic appearance of intracranial vessels in the model, Anteroposterior (AP) and lateral views of simultaneous injection of left and right internal carotid arteries (L ICA; R ICA) and the basilar artery (BA), simulating an ‘arch run’. Numbers in white font indicate diameters of corresponding vessel segments in millimeters. ACA, anterior cerebral artery; ICA, internal carotid artery; M1, M1 segment of the middle cerebral artery (MCA); M2, M2 MCA segment; M3, M3 MCA segment; M4, M4 MCA segment; PCA, posterior cerebral artery.
Model preparation
Once the 3D design was finalized, the model was fabricated using a 3D printer (Object Model 260 V, Object-Stratasys, Inc, Eden Prairie, Minnesota, USA) and TangoPlus material (Object-Stratasys, Inc, catalog no. OBJ-03224). After printing the model, the support material was removed manually from large-diameter vessels using a power-washer connected to tubing. For small-diameter distal vessels, the model was soaked in sodium hydroxide solution for 24 h, and the distal vessels were then flushed using catheters of various diameters. The model was next connected to a pulsatile pump, (Masterflex, Cole-Parmer, Vernon Hills, Illinois, USA) to simulate cardiac output (figure 1B). Circulating fluid was maintained at 37°C.
Fresh clots were prepared by mixing 4 mL of fresh swine blood (no anticoagulant), 32 mg of fibrinogen from bovine plasma (Sigma-Aldrich, St Louis, Missouri, USA; catalog no. F8630), and 1 unit of thrombin from bovine plasma (Sigma-Aldrich, catalog no. T4648) in a 5 mL syringe for at least 3 min, based on our laboratory protocol, which was adapted from earlier studies.11 ,12 The mixture was placed into plastic tubing (4 mm diameter) and incubated at room temperature for at least 60 min. Clots were then cut into 10 mm length pieces and introduced into the MCA M1 and M2 segments of the model (figure 1C). Pressure measurements of the intracranial vessels before and after clot introduction are shown in online supplementary figure S1.
Contrast material (Visipaque, 320 mgI/mL, GE Healthcare, Waukesha, Wisconsin, USA) was injected manually using a 10 mL syringe via a guide catheter positioned in the vessel territory of interest. Digital subtraction angiography was performed using a biplane angiographic suite with 8 inch×8 inch flat-panel detectors; 70 kVp, 17 mA, and 2.7 ms for frontal view; and 70 kVp, 12 mA, and 2.2 ms for lateral panels (Toshiba Infinix-i, Toshiba, Tochigi, Japan). A high-resolution region-of-interest imaging detector, the microangiographic fluoroscope-charge coupled device (MAF-CCD), was applied during deployment and retrieval of the Solitaire flow restoration. The MAF-CCD and its physical features13 and clinical application14 have been described in detail elsewhere.
Thrombectomy
After introduction of the clot into the MCA, a 6 F Cook shuttle (Cook Medical, Bloomington, Indiana, USA) was placed into the segment corresponding to the cervical ICA. Once the location of the occlusive clot was confirmed by angiography under roadmapping guidance and direct fluoroscopic injection, a 0.021 inch Orion microcatheter (Covidien, Mansfield, Massachusetts, USA) was delivered over a 0.014 inch microwire to cross the occlusion. A microinjection through the microcatheter was performed to visualize the extent of occlusion distally and create a roadmap for delivery of the stentriever. For experiments testing primary stentriever thrombectomy alone, a Solitaire flow restoration stentriever (Covidien), either 6 mm×20 mm for M1 occlusion or 4 mm×20 mm for M2 occlusion, was deployed, left for 5 min, and then retrieved into the Cook shuttle.
For experiments testing the combined stentriever–aspiration approach, we used a Navien 0.072 inch catheter (Covidien). The catheter was parked in the paraclinoid or ICA terminus segments, and continuous manual aspiration using a 20 mL syringe was applied while the stentriever was withdrawn until it was jammed into the Navien catheter tip and both were then pulled back as a single unit into the Cook shuttle.
A single thrombectomy attempt was allowed in each experiment. While performing thrombectomy, continuous visualization and video camera recording of the clot and the stentriever were performed to capture and document the location of any clot breakdown. Primary outcomes included the degree of recanalization (based on the TICI grading scale) and the occurrence of emboli in unaffected territory. Successful recanalization was defined as TICI score of 2b–3.
Statistical analysis
Analysis of variables was performed using Fisher's exact test. p<0.05 was considered statistically significant.
Results
Angiography simulating an ‘arch run’ with simultaneous injection of both ICAs and the basilar artery is seen in figure 2. There is a close anatomical resemblance to the human intracranial anterior circulation, demonstrating practicality and feasibility of the model to study various devices and approaches to stroke thrombectomy. The model allows easy and reliable delivery of the clot to the target site by intermittent occlusion of parallel inflow (arterial) tubing channels and preferential direction of flow.
A total of 22 experiments were conducted: 11 with stentriever thrombectomy alone and 11 with the combined stentriever–aspiration thrombectomy approach. Successful clot delivery to the MCA was achieved in all cases. Location of the occlusion within the MCA and final post-thrombectomy radiographic outcomes are summarized in table 1.
Stentriever alone versus combined stentriever plus aspiration thrombectomy
The clot was successfully captured after initial withdrawal of the stentriever from the MCA in all but one trial (see online supplementary video 1). In stentriever thrombectomy-alone experiments, visual inspection of the model showed clot disengagement and fragmentation in six of 11 trials during passage of the stentriever through the intracranial portions of the ICA—the two places were the clinoid segment and petrocavernous junction (figure 3; see online supplementary video 2). As a result, the clot traveled distally with anterograde flow back into the MCA, which caused recurrent occlusion of the MCA branches. With the combined stentriever–aspiration thrombectomy experiments, the clot was successfully captured in 10 of 11 retrieval attempts (figure 4; see online supplementary videos 3–8).
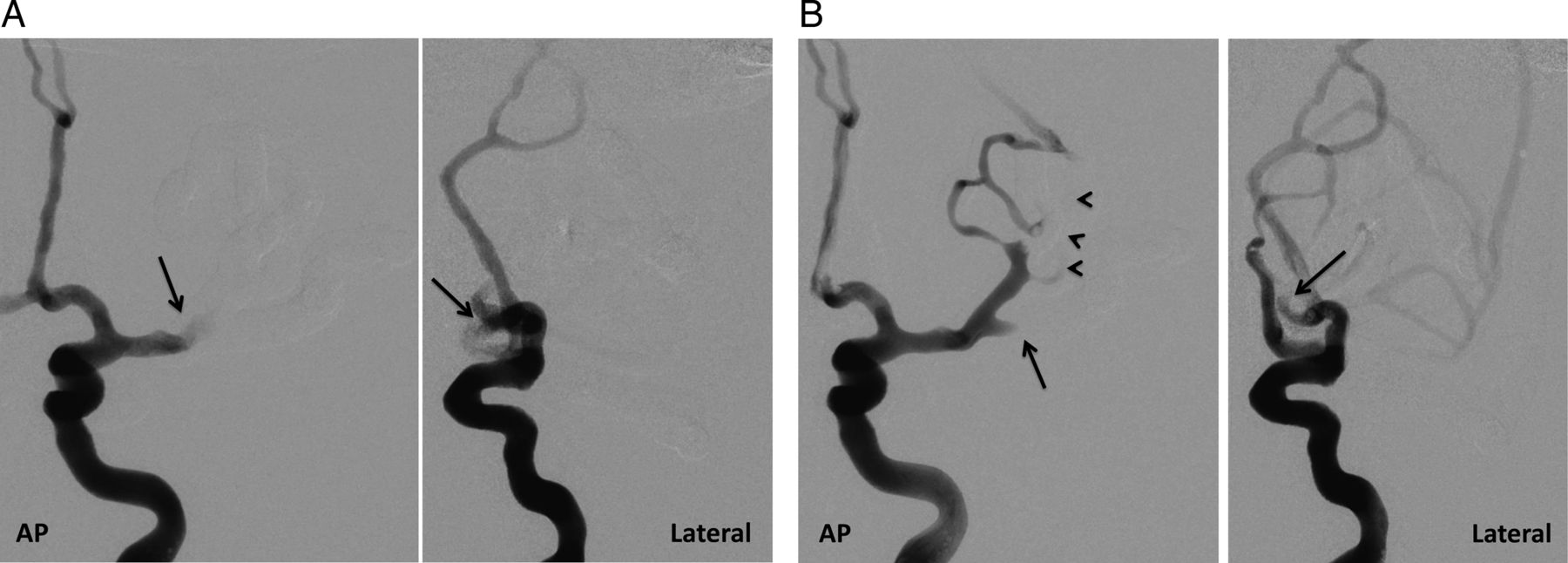
Stentriever alone approach to thrombectomy. (A) Baseline angiogram, anteroposterior (AP) (left) and lateral (right) views, left internal carotid artery injection showing occlusion at the level of the middle cerebral artery (MCA) bifurcation (arrow). (B) After a thrombectomy attempt, persistent occlusion of the inferior trunk of the MCA is seen. There is good filling of the proximal portion of the superior trunk of the MCA (arrows) but persistent occlusion of the distal MCA branches (arrowheads), corresponding to thrombolysis in cerebral infarction 2a recanalization.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
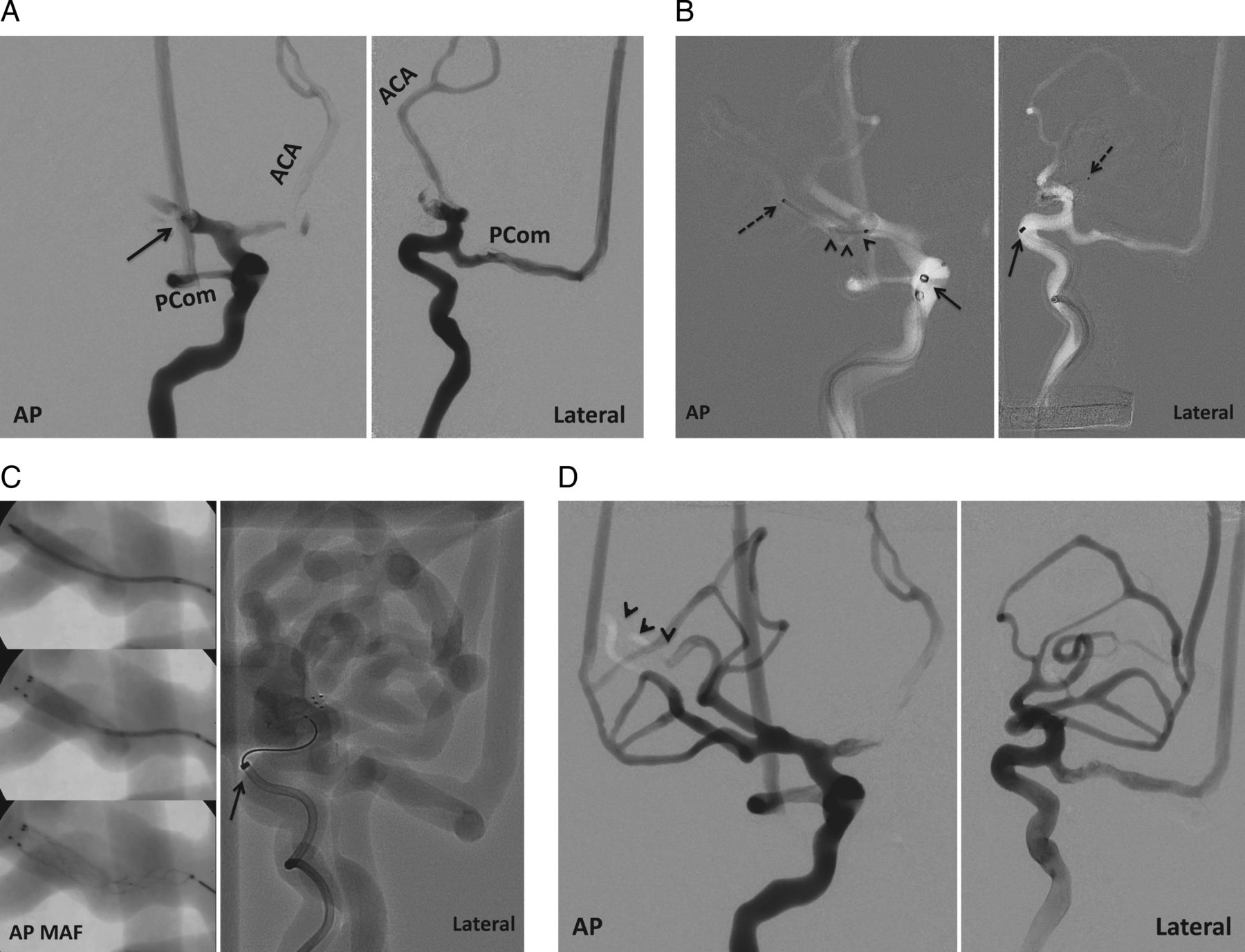
Combined stentriever plus aspiration approach to thrombectomy. (A) Baseline angiogram, anteroposterior (AP) (left) and lateral (right) views, right internal carotid artery injection, demonstrating occlusion at the middle cerebral artery (MCA) bifurcation (arrow). ACA, anterior cerebral artery; PCom, posterior communicating artery. (B) Angiogram with roadmapping assistance, AP (left) and lateral (right) views, showing delivery of the microcatheter across the clot. Dashed arrow marks the location of the microcatheter's distal marker. Arrowheads indicate the location of the clot. Arrow points to the location of the aspiration catheter. (C) AP views (left) of microangiographic fluoroscopy (MAF) showing gradual deployment of the Solitaire flow restoration stentriever. Lateral view (right) is a conventional angiogram demonstrating the fully deployed stentriever. Notice higher resolution provided by MAF in comparison with conventional angiography. Arrow points to the location of the aspiration catheter. (D) Final angiogram after successful thrombectomy, AP (left) and lateral (right) views, showing robust filling of the right MCA. There is a small distal area with delayed filing (arrowheads); therefore, the final recanalization grade is thrombolysis in cerebral infarction (TICI) 2b rather than TICI 3.
After a single pass, successful recanalization (TICI 2b–3) was achieved more often with combined stentriever–aspiration than the stentriever alone (in 10 vs 4 experiments; p=0.023). Emboli in new territory were seen in three of 11 retrieval attempts with the stentriever-alone approach, and none were seen with the combined approach, but the difference did not reach statistical significance (p=0.21). In all three cases, emboli in new territory involved previously unaffected M2 MCA territories.
Discussion
The usefulness of in vitro models in testing stroke thrombectomy devices has been demonstrated.5–8 Thrombectomy success can be measured by testing changes in flow pressure proximally and distally to the occlusion site or by analyzing the number and size of clot fragments. The advantage of such models includes the ability to replicate multiple experiments in a standardized fashion and thus accurately compare different types of thrombectomy devices, which is not feasible in clinical trials owing to multiple confounding factors, such as differences in patient anatomy and comorbid status or clot location and composition.
In clinical practice, thrombectomy success in stroke interventions is tested using angiographic recanalization grading scales, of which the TICI score is now used most commonly.9 Available in vitro stroke models lack the complexity to resemble the intracranial circulation, which is required for application of the TICI grading scale. In vitro models with more simplified anatomical design, which typically consist of a single inflow and outflow channel, measure changes in pressure and flow gradients. In our model, because of the extensive network of collaterals within the circle of Willis and MCA branches, we measured reperfusion with the TICI score rather than recording changes in pressure and flow gradients. Although recanalization scales can be applied to thrombectomy experiments conducted in animal models, high costs associated with such experiments and differences in anatomy are potential limiting factors.15 ,16
In vitro models with more complex intracranial anatomy have been successfully used as a training tool for embolization of aneurysms17; however, their use as stroke models thus far is very limited. Suzuki et al18 noted that their silicone stroke model failed to provide the feeling of realistic manipulation. This might be due to the much higher (approximately three- to fivefold) tensile strength of the silicone material in comparison with the tensile strength of the human arterial wall.19 ,20 The tensile strength of the TangoPlus material used in our model is within the 0.8–1.5 MPa range, which is similar to that of the human arterial wall.19 ,20
The combined stentriever–aspiration thrombectomy approach is now widely used in clinical practice, yet its advantage over the use of stentrievers alone has not been demonstrated.3 ,21 ,22 Our data suggest that withdrawal of the stentriever under continuous aspiration results in more effective capture and withdrawal of the clot, with higher recanalization and lower distal embolization rates.
The following points should be considered when interpreting our data and extrapolating it to a clinical setting. First, we used only the 0.072 inch Navien catheter for aspiration in our experiments. In clinical practice, the combined aspiration approach is performed using a variety of other aspiration catheters, such as the 5 MAX ACE (0.068 inch inner diameter catheter with a 0.060 inch distal tapered tip) or 5 MAX (0.064 inch inner diameter catheter with a 0.054 inch distal tapered tip) reperfusion catheters (Penumbra, Inc, Alameda, California, USA), or the 0.058 inch Navien catheter, which were not tested in our model.23 ,24 Second, in our experiments, only manual aspiration with a syringe was performed; continuous aspiration with the Penumbra pump was not tested. Data suggest that manual aspiration generates a higher dynamic pressure than the Penumbra aspiration pump.8 Also, using an aspiration catheter with a larger inner diameter can further increase dynamic pressure.8 Third, in clinical practice, some neurointerventionalists deliver the reperfusion catheter directly into the M1 MCA segment, whereas in our experiments, the aspiration catheter tip was positioned more proximally within the clinoid-terminus segments of the ICA. Although occlusion within the posterior circulation was not tested, on the basis of our experience with this model, we expect that intracranial vertebrobasilar and posterior cerebral arteries can also be successfully reconstructed and fabricated. Finally, we did not test the value of a balloon-guide catheter in our experiments, and the use of such a catheter can decrease the incidence of distal embolization, according to recent publications.4 ,5 All the above points will be addressed in our future experiments.
Conclusions
We have demonstrated the practicality and feasibility of using this in vitro intracranial circulation model for testing thrombectomy devices. Our experiments show that the combined stentriever–aspiration approach to thrombectomy leads to better angiographic recanalization rates than use of the stentriever alone. Further experiments are needed to test the value of balloon-guide catheters and aspiration performed using other types of catheters and modes of aspiration.
Acknowledgments
The authors thank Liza Pope BS for preparation of the clots, Paul H Dressel BFA for assistance with preparation of the illustrations, and Debra J Zimmer for editorial assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure
- Data supplement 2 - Online video 1
- Data supplement 3 - Online video 2
- Data supplement 4 - Online video 3
- Data supplement 5 - Online video 4
- Data supplement 6 - Online video 5
- Data supplement 7 - Online video 6
- Data supplement 8 - Online video 7
- Data supplement 9 - Online video 8
Footnotes
Contributors Conception and design: all authors. Acquisition of data: MM, SVSN, AHS, and CNI. Analysis and interpretation of data: all authors. Drafting the manuscript: MM and CNI. Critically revising the manuscript: all authors. Final approval of the manuscript: all authors.
Funding Thrombectomy devices were provided by Covidien. All data collection, analysis, and interpretation were performed by the authors, independent of the company's input or interpretation. National Institutes of Health (2RO1EB002873; for partial support of student and faculty). Toshiba (equipment).
Competing interests CNI received grants from the National Institutes of Health (2RO1EB002873; for partial support of student and faculty) and Toshiba (equipment) for this study. EIL has shareholder/ownership interests in Intratech Medical Ltd. and Mynx/Access Closure, and Blockade Medical LLC. MM has received an educational grant from Toshiba. SR received grants from the National Institutes of Health (2RO1EB002873; for partial support of student and faculty) and Toshiba (research and equipment) for this study. He receives financial support from Erie County Medical Center for services paid to the University at Buffalo Foundation. In addition, SR holds US patent no. 6,285,739 for region-of-interest microangiography. AHS has received research grants from the National Institutes of Health (co-investigator: NINDS 1R01NS064592-01A1, Hemodynamic induction of pathologic remodeling leading to intracranial aneurysms and NIBIB 5RO1EB002873-07, Micro-radiographic image for neurovascular interventions) and the University at Buffalo (Research Development Award); holds financial interests in Hotspur, Intratech Medical, StimSox, Valor Medical, Blockade Medical, and Lazarus Effect; serves as a consultant to Codman & Shurtleff, Inc, Concentric Medical, ev3/Covidien Vascular Therapies, GuidePoint Global Consulting, Penumbra, Stryker Pulsar Vascular, MicroVention, Lazarus Effect, and Blockade Medical; belongs to the Codman & Shurtleff, Inc speakers’ bureau; serves on National Steering Committees for Penumbra Inc's 3D Separator Trial, Covidien's SWIFT PRIME trial, and MicroVention's FRED trial; serves on advisory boards for Codman & Shurtleff and Covidien Neurovascular; and has received honoraria from Abbott Vascular and Codman & Shurtleff, Inc for training other neurointerventionalists in carotid stenting and for training physicians in endovascular stenting for aneurysms and from Penumbra, Inc All consulting is per project and/or per hour.
Ethics approval This study was approved by the University at Buffalo Health Sciences institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data may be made available as requested.