Article Text

Abstract
Objective We have previously developed three logistic regression models for discriminating intracranial aneurysm rupture status from 119 aneurysms based on hemodynamic–morphological parameters. In this study we exploit their use as a tool for predicting the risk of rupture of aneurysms with a defined Rupture Resemblance Score (RRS).
Methods We collected three-dimensional images of 85 consecutive aneurysms, applied the three regression models and compared model performance at predicting rupture status against anecdotal metrics (aneurysm size and aspect ratio). We then reinterpreted the model-predicted probability as RRS, where the higher the score the closer the resemblance to previously known rupture components, and applied the RRS prospectively to four unruptured aneurysms with borderline treatment decisions.
Results All three models yielded excellent sensitivity (0.78–0.83) and specificity (0.78–0.84) at a cutoff score of 50%, whereas aneurysm size and aspect ratio showed poor sensitivities (0.28 and 0.33, respectively). Lowering the cutoff score to 30% improved sensitivity to 0.90. The RRS identified most of the ruptured aneurysms and also some unruptured ones that closely resembled ruptured aneurysms hemodynamically and/or morphologically. The prospective application of the RRS to unruptured aneurysms shows that it could provide additional insights for treatment decisions.
Conclusions Previous regression models based on hemodynamic–morphological parameters are able to discriminate rupture in a new cohort in the same population. A higher probability of rupture is associated with larger size ratio, lower normalized wall shear stress and higher oscillatory shear index. The RRS could potentially stratify rupture risk and assist in treatment decision-making for unruptured aneurysms.
- Aneurysm
- Blood Flow
- Hemorrhage
- Stroke
Statistics from Altmetric.com
Introduction
Intracranial aneurysms (IAs) affect as much as 5–8% of the entire population.1 Aneurysm rupture leads to subarachnoid hemorrhage (SAH), a devastating event with high mortality (45% within the first year) and morbidity (50% of survivors with major disability).2 ,3 The estimated annual cost for hospitalized patients with unruptured IAs (UIAs) in the USA is $522 500 000, and $1 755 600 000 for patients with SAH.3 Recent advancements in neurovascular imaging have increased the detection of asymptomatic UIAs, placing more pressure on clinicians to decide which UIAs to treat and which ones to observe, since treatments are fraught with risk of complications and high costs.
Currently, aneurysm size is the main quantitative metric in evaluating the rupture risk of UIAs.4 ,5 However, small aneurysms still account for a large portion of ruptured cases that present clinically.6 Subsequently, shape-based morphological parameters have been explored and correlated with rupture.6–8 On the other hand, the hemodynamics of IAs have been widely studied and are believed to play a fundamental role in the mechanisms involved in aneurysm growth and rupture.9–13 A practical goal of IA research is to develop objective models to identify and treat only those UIAs at high risk of rupture.
Rupture risk prediction models should theoretically be built from longitudinal aneurysm data. However, most diagnosed UIAs are defensively treated, leaving only a small number for conservative observation and periodical imaging. These cases tend to involve aneurysms that are small in size with low assumed rupture risks, or aneurysms having no clear or safe surgical options, or patients who refuse treatment. Models built from longitudinal data therefore tend to be severely skewed and do not represent all high-risk aneurysm features.
However, it is possible to derive rupture status classification models from cross-sectional aneurysm datasets. In a retrospective study of 119 aneurysms we identified morphology and hemodynamics that discriminate ruptured from UIAs.9 Through multivariate logistic regression analysis, we built three distinct aneurysm rupture classification models based on morphological, hemodynamic, and combined metrics. A higher probability of rupture status was found to be associated with larger size ratio (SR) in the morphological model, lower normalized wall shear stress (WSS) and higher oscillatory shear index (OSI) in the hemodynamic model, and all three parameters in the combined model.9
The objectives of the current study were to validate the rupture status prediction in a new cohort of IAs by the previously built regression models and to explore the potential of these models in risk stratification of UIAs.
Methods
Study population
We prospectively collected 85 new aneurysms (18 ruptured, 67 unruptured) in 74 consecutive patients imaged at Millard Fillmore Gates Hospital in Buffalo between 2009 and 2010. This cross-sectional dataset was consecutive with the 119 aneurysms in our previous study in which we developed regression models.9
Morphological and hemodynamic parameter extraction
Morphological and hemodynamic parameters for each aneurysm were calculated as previously described.8 ,9 Briefly, three-dimensional (3D) images were segmented at the region of interest (aneurysm lumen and adjacent vessels) using the Vascular Modeling Toolkit (http://www.vmtk.org).14 An in-house MATLAB code was used to calculate the three morphological parameters used in the current study8: aneurysm size, SR, and aspect ratio (AR). For computational fluid dynamics (CFD) simulations, finite volume meshes of 0.5–1 million elements generated from ICEM CFD (ANSYS, Canonsburg, Pennsylvania, USA) were imported into the CFD solver Star-CD (CD Adapco, Melville, New York, USA) to calculate time-resolved 3D velocity and pressure fields. Three pulsatile cycles were simulated, with the last cycle being taken as the output to ensure that numerical stability had been reached. From the flow solutions we calculated the two most critical hemodynamic parameters9—namely, WSS and OSI.
Performance evaluation of the regression models
We applied the three regression models from our previous study9 to each of the 85 IAs in the new cohort and calculated their probability of being ruptured. Adopting a 50% probability cutoff, the statistical models classified each aneurysm from the current study as either ruptured (>50%) or unruptured (<50%). The sensitivity (rate of correct prediction of ruptured IAs) and specificity (rate of correct prediction of UIAs) for classifying these 85 new aneurysms were calculated by comparing their probability with the actual rupture status at the time of imaging. Classifications were also made from clinically used metrics: aneurysm size (>7 mm classified as high risk of rupture)5 and AR (>1.6 as high risk of rupture).6 To examine whether these common classifications can pick out the ruptured IAs in the cohort, we evaluated their sensitivity and specificity. Furthermore, for the three regression models we varied the probability threshold and plotted the resulting sensitivities and specificities to examine its influence on prediction performance in these 85 IAs.
Exploring the potential of the regression models in risk stratification of UIAs
We further examined the false-positive cases in the 85 new IAs—that is, UIAs classified as ruptured IAs by the regression models. We take an alternative view of the prediction by these regression models, which were originally intended to evaluate the probability of an aneurysm being ruptured. When applied to a given UIA, the regression models measure how much the aneurysm in question resembles the ruptured IAs in the original (training) database hemodynamically and/or morphologically. Hence, we reinterpret this probability as the Rupture Resemblance Score (RRS), where the higher the score the closer the resemblance to previously known rupture components. The RRS can identify UIAs that closely resemble ruptured aneurysms and thus may merit treatment recommendation. This allows us to explore the potential of these regression models for risk stratification in UIAs in general. In order to illustrate how the RRS could assist in clinical treatment decisions, we then prospectively applied these regression models to four additional UIAs encountered in our clinical practice.
Results
Validation of the regression models
At a 50% probability cutoff, the three hemodynamic–morphological classification models predicted aneurysm rupture status in the new cohort with high sensitivity (0.78, 0.83, and 0.79 for morphological, hemodynamic, and combined models, respectively) and specificity (0.81, 0.84, and 0.78 for the three models) (figure 1). In contrast, if used to discriminate ruptured IAs from UIAs, size and AR showed poor sensitivities (0.28 and 0.33, respectively) and high specificities (both 0.81) (figure 1).

Sensitivity and specificity of predictions by the three regression models (M1: morphological model, M2: hemodynamic model, M3: combined model; 50% probability cutoff) and by clinical metrics: size and aspect ratio (threshold at 7 mm and 1.6, respectively) for 85 aneurysms.
Exploration of the models in risk stratification of UIAs
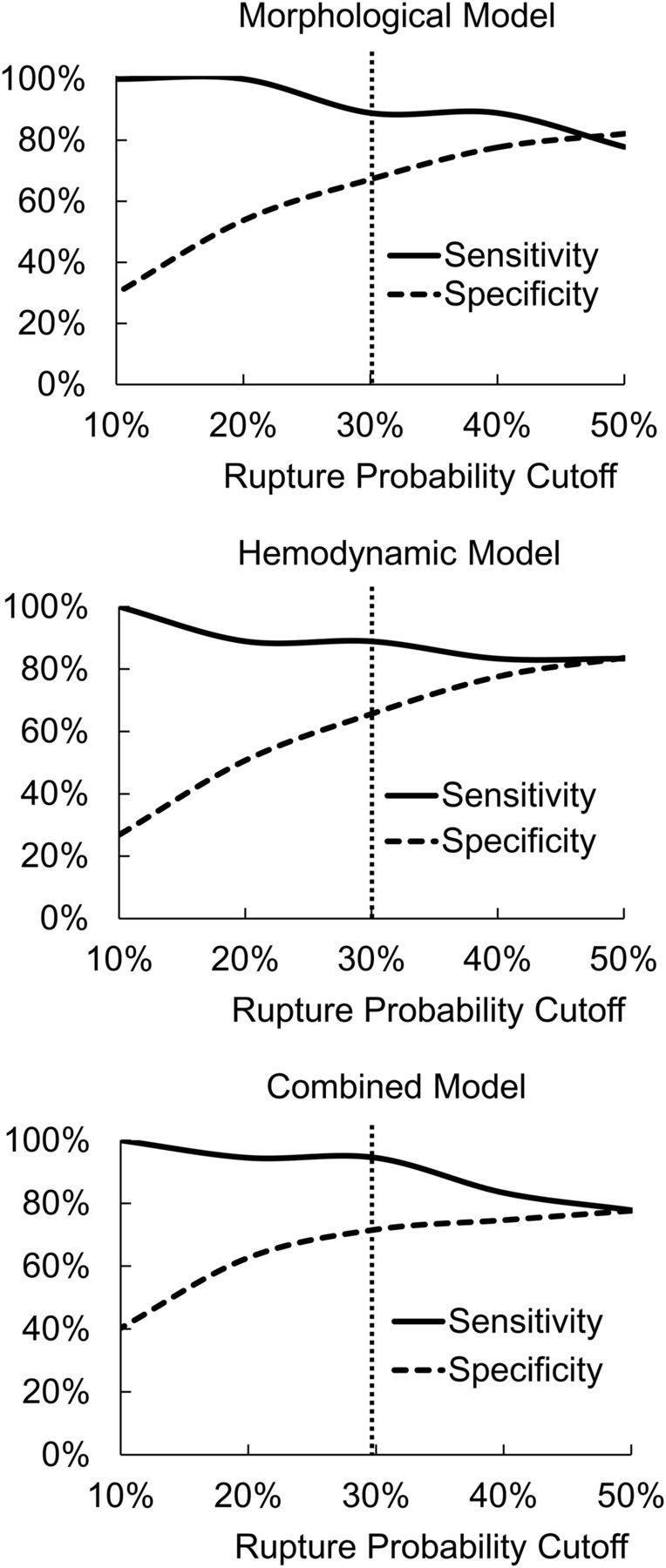
Figure 2 shows how the sensitivity and specificity of the three classification models varied with the probability cutoff. Lowering the cutoff threshold increased the sensitivity of rupture classification but reduced the specificity; 50% gave sensitivity and specificity values of around 0.8, but the catastrophic nature of SAH necessitated a high sensitivity for identifying ruptured IAs. From figure 3, a lower threshold of 30% delivered higher sensitivity values (0.89, 0.89, and 0.94 for morphological, hemodynamic, and combined predictive models, respectively) and acceptable specificity values (0.67, 0.67, and 0.72). At 30% probability cutoff, the combined model produced higher sensitivity and specificity than the hemodynamic and morphological models.

Sensitivity and specificity of predictions versus probability cutoffs for the three regression models. 30% cutoff delivers a higher sensitivity than 50%, and the combined model gives the best performance at this cutoff.

Examples of false-positive prediction cases where unruptured intracranial aneurysms (IAs) were classified as ruptured IAs. These aneurysms highly resembled ruptured IAs. In reality, they were treated right away (unrelated to the calculation). OSI, oscillatory shear index; WSS, wall shear stress.
At 30% probability cutoff, we encountered 22, 22, and 19 cases of false-positive prediction out of the 67 cases of UIA using the morphological, hemodynamic, and combined models, respectively. As shown in figure 3, these UIAs bore a high resemblance to ruptured IAs in morphology (complex geometry, high SR) and hemodynamics (complex flow pattern, low WSS, high OSI). Clinical records showed that all these aneurysms were treated immediately. This suggests that the RRS could be valuable for identifying potentially dangerous UIAs that closely resemble ruptured IAs hemodynamically and/or morphologically.
Illustrative cases
The four additional prospective UIA cases anecdotally support the notion that the RRS could assist treatment decision-making for various types of aneurysms, especially borderline cases. The angiographic images, flow field, WSS, and OSI of these aneurysms are shown in figure 4. We used a conservative criterion that, if one or more of the three regression models gave an RRS >30%, the aneurysm probably should be treated. The final treatment decisions for these aneurysms were made based on our surgeon’s clinical judgment.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Four prospective cases of unruptured aneurysm to demonstrate how the three models could help treatment decision-making. The first case was a posterior inferior cerebellar artery aneurysm with large size ratio (SR) and Rupture Resemblance Score (RRS) confirming the decision to treat. The second and third cases were from a patient with three aneurysms; a large RRS favored treatment of the basilar tip aneurysm in addition to the symptomatic internal carotid artery aneurysm. The fourth case was a 5 mm middle cerebral artery aneurysm with a large RRS favoring a decision to treat. OSI, oscillatory shear index; WSS, wall shear stress.
Case 1: RRS could confirm decision to treat
Patient 1 was admitted with symptoms of dizziness and nausea for a few months. Digital subtraction angiography (DSA) showed an 8 mm right posterior inferior cerebellar artery (PICA) aneurysm located immediately adjacent to the take-off of the right PICA (figure 4). Our clinical team intended to treat this aneurysm based on its high two-dimensional SR measured from the angiogram,15 ,16 despite its size being slightly larger than the conventional threshold of 7 mm. We calculated its 3D morphological and hemodynamic parameters. Its high SR (9.6), low normalized WSS (0.1), and high OSI (0.0179) (figure 4) gave a rather high RRS (100%, 93.7%, and 100% from morphological, hemodynamic, and combined models, respectively). Our models could confirm the decision to treat. In reality this patient was treated by clipping without any complication.
Cases 2 and 3: RRS could inform which aneurysms to treat among multiple aneurysms
Patient 2 presented with right hand and foot numbness. Diagnostic DSA showed three aneurysms located at the left internal carotid artery (ICA, 10 mm), left middle cerebral artery (MCA, 3 mm), and basilar tip (7 mm). The left ICA and MCA aneurysms are shown as Case 2 and the basilar tip aneurysm is shown as Case 3 in figure 4. Our clinical team initially decided to treat the left ICA aneurysm due to the symptoms. We calculated the SR, WSS, and OSI for all three aneurysms and inserted the values into the hemodynamic–morphological models to evaluate their RRS. The RRS of the left ICA aneurysm were 52.7% (morphological), 27.5% (hemodynamic), and 38.6% (combined); the RRS of the left MCA aneurysm was <20% from all three models; and the basilar tip aneurysm had RRS of 82.1%, 55%, and 79.5% despite its smaller size (7 mm compared to 10 mm of the ICA aneurysm). This additional information provided by the RRS could help us to decide to treat the basilar tip aneurysm in addition to the left ICA aneurysm. In reality, both the left ICA and basilar tip aneurysms were treated by coiling without recurrence.
Case 4: RRS could guide decision to treat
Patient 3 with a family history of IAs was found to harbor an unruptured 5 mm right MCA aneurysm during screening. Based on the traditional metrics of size, this small aneurysm should possess a low risk and could be left to be monitored. We calculated the morphological (SR=2.15) and hemodynamic metrics (WSS=0.18, OSI=0.0115). Despite its small size, the RRS was calculated to be 30.8%, 78.5%, and 63.3% from morphological, hemodynamic, and combined models, respectively. This RRS is considered high (>30%). Based on this information, we could have decided to treat the aneurysm. In reality, this MCA aneurysm was treated by stent-assisted coiling without recurrence.
Discussion
While large trials like the International Study of Unruptured Intracranial Aneurysms (ISUIA)4 ,5 and Japanese studies17 ,18 have investigated rather simplistic predictors of rupture such as size, more comprehensive models involving both hemodynamic and morphological features are required for predicting rupture risk. The recently released new American Heart and Stroke Association guidelines for IA management19 recommends consideration of morphological and hemodynamic characteristics of the aneurysm in determining rupture risk assessment and optimal treatment, in addition to the size, location, and patient demographics. To this end, we previously built three hemodynamic–morphological discrimination models from 119 cross-sectional aneurysm samples (the training set) to classify rupture status.9 The current study shows that these regression models are able to predict aneurysm rupture status with high sensitivity and specificity in a testing set of a new IA cohort. This successful validation further supports our original conclusion that morphology and hemodynamics can be used to discriminate ruptured from unruptured aneurysms.9
The study validates the three previously developed rupture classification models in predicting aneurysm rupture status in a new cohort from the same center and, more importantly, it proposes and demonstrates the potential clinical utility of the RRS in risk stratification for UIAs. Using the RRS to stratify risk in UIAs incorporates an implicit hypothesis: the more similar an aneurysm in question is to ruptured IAs (hemodynamically and/or morphologically), the more likely this aneurysm is to experience rupture in the future. This hypothesis is difficult to test because longitudinal data of UIAs (including those going on to rupture) is rare and not easy to obtain. The available longitudinal samples are small and tend to be skewed, but they may become increasingly available. For example, routine screening for IAs has recently been introduced into clinical practice in Japan and could make longitudinal validation possible.20 ,21
In this study we demonstrated the trend of sensitivity and specificity by varying the RRS cutoff. We favor an RRS cutoff of 30% over 50% for clinical use since it gives higher sensitivities (around 0.9) and acceptable specificities (around 0.7), and high sensitivity is required for a metric that aims at identifying dangerous IAs given the high morbidity and mortality of aneurysmal SAH. However, treatment decisions are complicated and multifactorial. Choosing a RRS cutoff value for informing the decision to treat in reality depends on the preferences and judgments of different surgeons and should be considered with other factors such as the patient's medical condition, age, and surgical risks. After all, the RRS only provides an additional piece of information to consider which is quantitative and related to IA pathophysiology,22 and in some difficult borderline cases may provide the needed insight and direction. The three predictive models do not compete with each other since the morphological and hemodynamic models calculate the RRS from different perspectives while the combined model consolidates the two.
Our results indicate low WSS and high OSI as hemodynamic discriminators of rupture status. This is in contrast to studies by Cebral et al10 which found that high WSS was associated with ruptured aneurysms. WSS can drive vascular remodeling and, as we have recently proposed, both low WSS and high WSS may independently facilitate IA growth and rupture, albeit via different biological mechanisms.22 ,23 It seems that our studies (current and Xiang et al9) and the study by Cebral et al10 deal with different patient populations that might be skewed towards different types of IAs —that is, those dominated by low WSS versus high WSS. Our rupture discrimination models are accurate for our single-center patient population but not necessarily for other populations, although many recent publications have also identified low WSS as the rupture indicator.11 ,12 ,24 ,25 Thus, these classification models and the derived RRS may be useful at centers where low WSS has been associated with ruptured aneurysms in their patient populations.
The RRS could be of great interest to the neurosurgical community as many of them struggle to select UIAs for treatment. However, we should not overstate the clinical utility of this score, and currently the clinical application of the RRS is limited. First, further investigation is needed to elucidate the role of low and high WSS in aneurysm rupture mechanisms. Second, we should perform a true prospective evaluation of the predictive ability of the RRS in a large-scale multicenter follow-up trial. This study could potentially be used as the foundation for conducting a prospective trial. Third, the current RRS does not take into account patient demography, medical condition and surgical risks, which may dominate the ultimate treatment decision. The rupture risk of an aneurysm from morphology and hemodynamics is one of many factors to consider in the treatment of a given aneurysm. Thus, currently, the surgeon’s clinical judgment must ultimately prevail in decision-making.
There are several limitations in this study. First, the number of new cases is small and come from the same hospital as our previous study.9 Even with the increased sample size in the current study, there may still be a selection bias and our conclusion may not be valid for different patient populations. In the future, multicenter studies with a larger multi-population are needed to validate these models or even build new models.26 Second, aneurysm geometries may have been affected by the rupture event, although increasing evidence indicates that aneurysms do not shrink when they rupture.8 ,27 Third, the RRS cannot be used to predict the time span in which a given aneurysm may rupture. The RRS is different from rupture rates in patients with prospective aneurysms such as the ISUIA data.4 ,5 However, the RRS measures how much a UIA hemodynamically and morphologically resembles the ruptured IAs in our database, which is helpful for UIA treatment decision-making.
Conclusions
The previously developed statistical rupture classification models based on morphometrics and hemodynamics have been validated by a new cohort of aneurysms. The RRS calculated from these models has the potential for risk assessment of UIAs in clinical practice. Clinical application of the RRS needs further investigation.
References
Footnotes
Contributors Conception and design: JX, AHS, HM. Acquisition of data: all authors. Analysis and interpretation of data: JX, JY, AHS, HM. Drafting the manuscript: JX, HC, HM. Critical revision of the manuscript and final approval of the manuscript: all authors.
Funding This work was supported by NIH grant R01NS064592, the American Society for Quality Biomedical Division Dr Richard J Schlesinger grant and the Toshiba Medical Systems grant.
Competing interests HM: principal investigator of NIH grant R01NS064592. JX: awardee for the American Society for Quality Biomedical Division Dr Richard J Schlesinger grant. EIL: research grant, devices, honoraria from Boston Scientific; research support from Codman and Shurtleff, ev3/Covidien Vascular Therapies; ownership interests in Intratech Medical, Mynx/Access Closure; consultant to Codman and Shurtleff, ev3/Covidien Vascular Therapies, TheraSyn Sensors; fees for carotid stent training from Abbott Vascular, ev3/Covidien Vascular Therapies. AHS: co-investigator of NIH grant R01NS064592, University at Buffalo; financial interests in Hotspur, Intratech Medical, StimSox, Valor Medical; consultant to Codman and Shurtleff, Concentric Medical, ev3/Covidien Vascular Therapies, GuidePoint Global Consulting, Penumbra; speakers’ bureaus for Codman and Shurtleff, Genentech; advisory board of Codman and Shurtleff; honoraria from Abbott Vascular, Codman and Shurtleff, Genentech and Neocure Group. KVS: research and consultant support for Boston Scientific, Cordis, EndoTex, EPI, Guidant, Medtronic, Micrus, Kerberos, Zimmer, Abbott Vascular,ev3 and Toshiba; financial interests in EndoTex, Micrus, BSC EPI, Access Closure, Primus and Cordis; stockholder in Boston Scientific and Access Closure. Grant from Toshiba Medical Systems.
Ethics approval Ethics approval was obtained from the Institutional Review Board of the University at Buffalo.
Provenance and peer review Not commissioned; externally peer reviewed.