Article Text

Abstract
Aims Recent recommendations on the designation of target artery lesions in acute ischemic stroke include the anatomical differentiation between a proximal and a distal occlusion site of the M1 segment of the middle cerebral artery (MCA). The aim of this study was to evaluate whether these occlusion types differ in terms of a disability-free (modified Rankin Scale (mRS) 0 or 1) clinical outcome at 90 days.
Methods A retrospective analysis was performed of all patients with MCA M1 occlusions who had a successful revascularization result after mechanical thrombectomy between October 2009 and September 2013 and for whom follow-up at 90 days was available. Imaging data were regraded and re-evaluated according to the modified Thrombolysis In Cerebral Infarction (mTICI) scale and the respective vessel occlusion site definitions. Outcome measures included National Institutes of Health Stroke Scale (NIHSS), mRS, Alberta Stroke Program Early CT Score (ASPECTS) scoring and procedural timings.
Results 62 patients were successfully recanalized; follow-up at 90 days was available for 42/62 patients (68%). There were proximal MCA occlusions in 24/42 patients (57%) and distal occlusions in 18/42 (43%). Baseline NIHSS, ASPECTS, procedural timings and final mTICI scores did not differ significantly between proximal and distal M1 occlusions. There was a statistically significant difference between proximal and distal M1 occlusions regarding a disability-free early outcome (mRS 0 or 1) at discharge (p=0.03) and at 90 days (p=0.04).
Conclusions Proximal occlusions of the M1 segment of the MCA incorporating the lenticulostriate perforators are associated with a poorer clinical outcome than distal M1 occlusions that spare these perforators. Involvement of these perforators might become an additional predictor of clinical outcome after mechanical thrombectomy in ischemic stroke.
- Artery
- Stroke
- Angiography
- CT
- Thrombectomy
Statistics from Altmetric.com
Introduction
The clinical outcome after severe acute ischemic stroke treated by endovascular means or intravenous thrombolysis (IVT) is considered to depend mainly on the time interval from symptom onset to recanalization and on the quality of the recanalization result. Other important factors influencing the clinical outcome are age, comorbidities, and the localization of the vessel occlusion as well as the quality and quantity of collateral flow.1–6 Brainstem ischemia with an underlying occlusion of the basilar artery is associated with a poorer prognosis than occlusions of proximal large vessels within the anterior circulation.7 ,8 Other circumstances such as so-called tandem-occlusion, comprising an occlusion of the extracranial internal carotid artery followed by an additional vessel occlusion within the anterior circulation, might also be associated with a poorer clinical outcome than single large vessel occlusions. To date, only case series have been published, yielding ambiguous results.9 ,10
Several approaches have been made to predict the outcome of patients with acute ischemic stroke. The reliability and clinical value of the Alberta Stroke Program Early CT Score (ASPECTS) for grading baseline cranial CT in order to predict the outcome after ischemic stroke has been proven in the setting of IVT as well as mechanical thrombectomy (MT).11 ,12 Its applicability to perfusion CT has been demonstrated recently, broadening the spectrum of pre-interventional imaging interpretation.13 Advances have also been made on the anatomical definition of vessel occlusion sites and their respective target downstream territories in the setting of MT. Recent recommendations in the consensus statement of the Cerebral Angiographic Revascularization Grading (CARG) Collaborators, Stroke Imaging Repository (STIR) Revascularization Working Group, and STIR Thrombolysis in Cerebral Infarction (TICI) Task Force on the exact anatomical definition of an occluded arterial segment in acute ischemic stroke and its respective target downstream territory include an anatomical differentiation between the proximal and distal portions of the M1 segment of the middle cerebral artery (MCA). Such a distinct designation is a prerequisite for determining the novel mTICI score.14 Whether the differentiation of MCA M1 occlusions into proximal and distal occlusions has an impact on the clinical outcome after MT has not yet been investigated. The originally published definition of M1 occlusions allows for two alternative approaches: an occlusion should be classified as a proximal M1 (pM1) occlusion when it involves the proximal half of the M1 segment or when no lenticulostriate vessels are visualized, or it should be classified as a distal M1 (dM1) occlusion when it involves the distal half of the M1 segment or when it spares the lenticulostriate perforators.14 We think that only the definition based on the lenticulostriate perforators as a definite categorizing imaging feature is clear enough to justify an analysis of the resulting imaging and clinical outcome in M1 occlusions. Taking into consideration the fact that ischemic stroke comprising the basal ganglia—and especially internal capsule stroke—leads to a progressive impairment of motor function, the role of clot localization with regard to the lenticulostriate perforators within the M1 segment of the MCA might be crucial for the clinical outcome after MT.15–17 Consequently, the aim of this study was to evaluate whether this anatomical distinction between a pM1 and a dM1 MCA occlusion based on the lenticulostriate perforators as a categorizing factor can serve as a predictive factor of the disability-free survival after 90 days of MT.
Material and methods
We screened our prospectively kept neurointerventional database for all patients who received MT with or without additional IVT for the treatment of an acute ischemic stroke with underlying MCA M1 occlusion from October 2009 to September 2013. We excluded from further analysis all patients with a revascularization result mTICI <2a and all patients with underlying high-grade M1 stenosis. Additionally, we excluded all patients from further analysis if no 90-day follow-up was available. No other criteria for patient selection were applied. Clinical data were taken from the electronic patient records. A specialist in neurology performed National Institutes of Health Stroke Scale (NIHSS) and modified Rankin Scale (mRS) scoring of the patients. mRS at 90 days was either conducted by a standardized telephone interview performed by a neurologist or during a follow-up visit in the outpatient clinic. All angiographic and CT images were analyzed by an experienced, fully certified interventional neuroradiologist (AM) who was blinded to all clinical and demographic data. The baseline ASPECTS score was calculated before analyzing the angiographic data. A dM1 occlusion was defined as occlusion of the MCA M1 segment beyond the most lateral branch of the lenticulostriate arteries in the initial digital subtraction angiography (DSA) run, allowing normal angiographic visualization of the perforators. A pM1 occlusion was defined as any occlusion of the MCA M1 that compromised visualization of the lenticulostriate arteries as a whole or in part (figure 1A, B). Whenever necessary, pre-interventional standardized multiplanar stroke CT imaging reconstructions in Maximum Intensity Projections were analyzed in addition to the DSA runs. MT was deemed to be successful if a final revascularization result of mTICI ≥2a was achieved. MT was carried out using either a coaxial stent retriever-based approach with proximal aspiration through the guide catheter (2009–2011) or using a triaxial approach with the Penumbra Separator 3D (Penumbra, Alameda, California, USA) in concert with lesional aspiration through the intermediate catheter (since 2012). All 24 h control CT scans were analyzed for potential infarctions, taking into account the respective target downstream territories of the initial clot location (figure 2A, B). A disability-free survival on discharge and at 90 days was defined as mRS≤1.
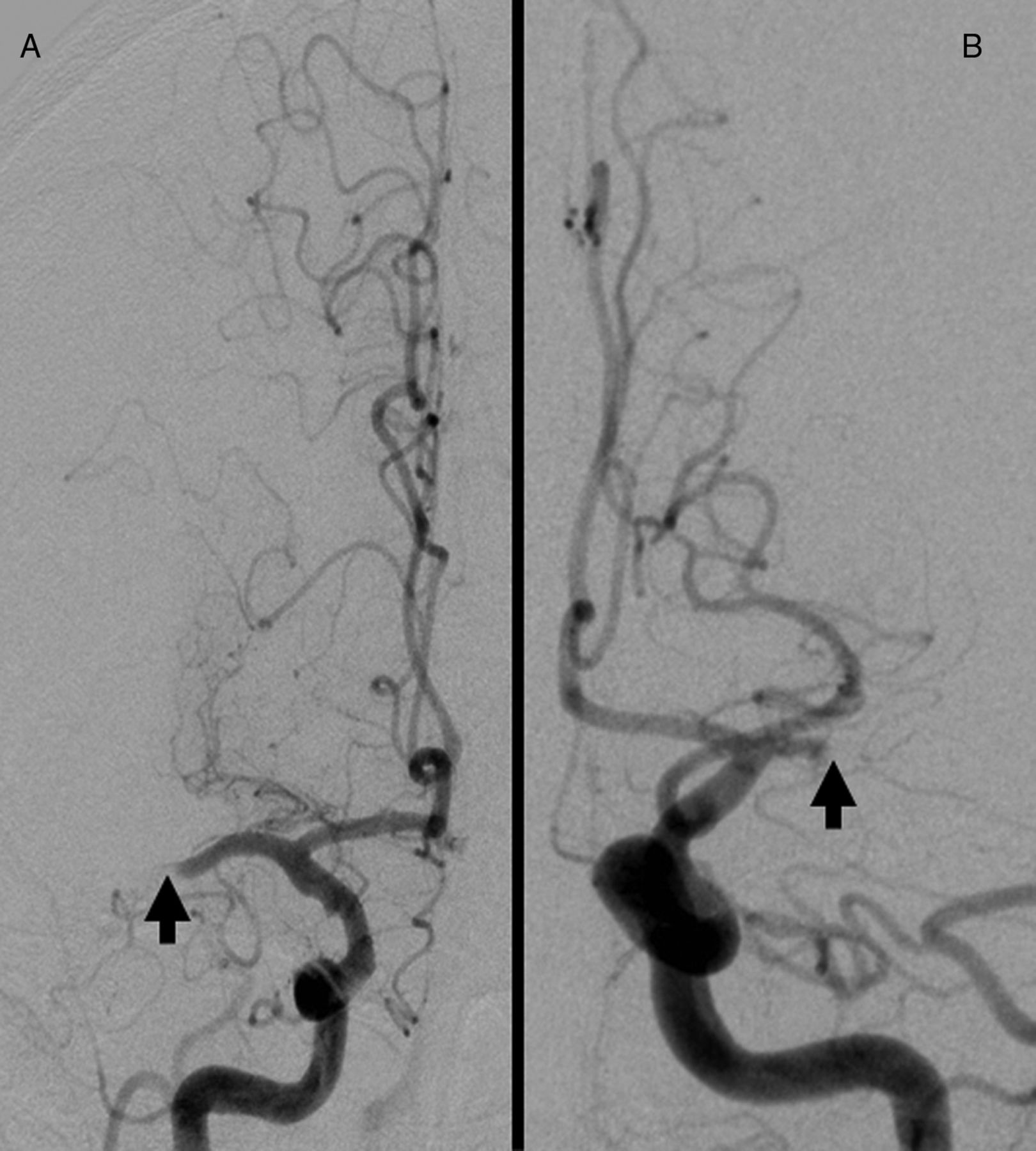
(A) Example of a distal M1 occlusion sparing the lenticulostriate perforators (arrow). (B) Example of a proximal M1 occlusion involving the lenticulostriate perforators (arrow).

{kind=link}
{kind=link}
(A) Small infarct within the lentiform nucleus after successful mechanical thrombectomy of a distal M1 occlusion (arrow). (B) Typical infarct localization after successful mechanical thrombectomy of a proximal M1 occlusion comprising the internal capsule (arrow).
Statistical analysis
Continuous study parameters were compared between patients with a pM1 occlusion and those with a dM1 occlusion by either the Welch t test in case of a normal distribution or by the Mann–Whitney U test in case of non-normal or ordinal distribution. Categorical variables were compared using the Fisher exact test. All statistical analyses were performed using Graph Pad Prism V.6.1 (Graphpad Software, La Jolla, California, USA). The significance level for all tests was set at α=0.05.
Results
We identified 62 patients who received successful MT for the treatment of MCA M1 occlusions. Follow-up at 90 days was available for 42/62 patients (68%). Demographic data and the outcome variables are summarized in table 1. The pM1 and dM1 subgroups did not differ significantly in their demographics or in terms of stroke severity on admission (NIHSS); the relevant procedural time intervals were also comparable. The baseline ASPECTS score did not differ significantly between the pM1 and dM1 groups. A revascularization result of mTICI 2b or 3 was achieved in 38/42 cases (90%), with no significant difference between the groups. Thirty-seven of the 42 patients (88%) received IVT; the IVT rate was higher in the dM1 group (100%). However, there was no statistically significant difference between the groups regarding the IVT rate, although there was a trend towards a higher rate of IVT in the dM1 group. An infarct comprising the internal capsule was seen in 22/42 patients (52%) (24 h CT control scan). Subgroup analysis showed that the vast majority (20/24) of these infarctions occurred in the pM1 occlusion group; this result was statistically highly significant (p<0.0001). Disability-free survival at discharge was achieved in 7/18 patients (38%) in the dM1 group and 2/24 patients (8%) with a pM1 occlusion (p=0.03, table 2). Of these two patients, only one had received IVT prior to MT. At 90 days, disability-free survival was achieved by 13/42 patients (31%), nine of whom presented with a dM1 occlusion. The difference between the groups was statistically significant (p=0.04). In view of these results, a pM1 occlusion in the initial run of the DSA has a sensitivity of 69% (95% CI 49% to 85%) and a specificity of 69% (95% CI 39% to 91%) as a predictor of a persistent disability at 90 days; the corresponding positive predictive value was 83% (95% CI 63% to 95%) and the negative predictive value was 50% (95% CI 26% to 74%). The presence of an infarct comprising the internal capsule was seen in 20/29 patients (69%) with a persistent disability at 90 days, with only 2/13 patients (15%) with disability-free survival having had such an infarct; this difference was highly significant (p=0.002).
Characteristics of all patients with 90 days follow-up (pM1 and dM1 groups)
Patient characteristics according to the clinical outcome at 90 days
Discussion
Time from symptom onset to revascularization and revascularization results are known to be strong predictors of outcome after the treatment of acute ischemic stroke; age and baseline ASPECTS score also play a role.1–5 ,10–12 The question whether the localization of a MCA M1 occlusion might predict an unfavorable outcome or, in other words, whether a dM1 occlusion might be associated with a better clinical outcome after MT has not yet been investigated in detail. In the present cohort we were able to demonstrate that there is a significant association between a pM1 occlusion that involves the lenticulostriate perforators as a whole or in part and a persistent disability after successful recanalization in MT. These findings clearly correspond to the anatomy of the blood supply within the basal ganglia and the internal capsule, which is mainly dependent on the ascending perforators arising from the M1 in the vast majority of cases.18 Interestingly, these findings did not go along with significant differences in baseline NIHSS, age, or time from symptom onset to revascularization. It was the exact anatomical location of the clot in the M1 in relation to the perforators that played a key role for the outcome. The majority of patients with pM1 occlusions had a cerebral infarct which affected the internal capsule; this type of infarct was associated with a poorer outcome in our cohort. A cerebral infarct comprising the internal capsule is more likely to be caused by a pM1 occlusion, and this type of infarct has been reported to be associated with a progressive disability 1 year after the stroke.18 We therefore investigated whether a pM1 occlusion could act as a predictor of a persistent disability at 90 days. In our series, a pM1 occlusion was found to have a sensitivity of 69% and specificity of 69% whereas the positive predictive value for the prediction of a persistent disability was 83%. These preliminary values might be too low to justify routine integration into clinical practice. A reason for this might be the relatively small number of cases limited by the study design as a retrospective single-center evaluation. Nevertheless, we think that our results justify further investigation in larger cohorts.
The retrospective design and the small number of cases are limitations of the study which affect the validity of our results. Whether the exact anatomical clot location in M1 occlusions can definitely act as a predictor of an unfavorable outcome at 90 days and its impact on the long-term follow-up has to be investigated in detail in future trials.
Conclusion
An anatomical distinction between a pM1 and a dM1 MCA occlusion based on the lenticulostriate perforators as the categorizing element can serve as a predictive factor of the disability-free outcome at 90 days. Compared with a dM1 occlusion, which spares the perforators, a pM1 occlusion leads to a significantly higher number of infarctions in the internal capsule after MT and is significantly associated with a higher rate of persistent disability at 90 days.
References
Footnotes
Contributors All authors made a substantial contribution to the conception or design of the work; the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content and final approval of the version to be published, and al authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None.
Ethics approval According to the guidelines of the local ethics committee, no approval was necessary.
Provenance and peer review Not commissioned; externally peer reviewed.