Article Text

Abstract
Background Flow diverters have been used predominantly for large anterior circulation aneurysms. Data on the safety and efficacy of this treatment for posterior circulation aneurysms are limited.
Objective To present our posterior circulation flow diverter experience, outcomes and morbidity in comparison with recent studies.
Methods A retrospective chart and imaging review of six patients with seven aneurysms in posterior circulation vessels, treated with flow diverter technology was carried out. A literature review was performed using standard online search tools.
Results We included five saccular and two fusiform posterior circulation aneurysms. An average of two flow diverters was placed for each patient. Adjunctive coiling was used in three cases. Follow-up at an average of 14.5 months showed complete angiographic occlusion in 4 (57.1%) cases, including one patient with in-stent thrombosis and major brainstem stroke at 4.5 months, a week after self-discontinuing dual antiplatelet therapy. Two other patients developed small periprocedural strokes but had excellent recovery. One death occurred 18 months after the initial procedure. No aneurysm rupture or parenchymal hemorrhage was seen. Overall, 5 (71%) cases, all with saccular aneurysms, had good clinical outcome (modified Rankin score (mRS) 0–1). Fusiform basilar aneurysms had markedly worse outcomes (mRS 5 and 6). Our literature review yielded six other studies with 100 additional patients. Overall, good outcome was seen in 74.3%, with a 12.3% average mortality and 11% permanent neurologic deficit rate. Complete occlusion varied from 43% to 100%.
Conclusions Flow diversion may be a possible treatment in carefully selected patients with high-risk atypical posterior circulation aneurysms, with poor natural history and no optimal treatment strategy. Symptomatic and fusiform large aneurysms appear to carry the highest risk. Further studies are necessary to assess the role of flow diversion in the posterior circulation.
- Aneurysm
- Blood Flow
- Flow Diverter
- Posterior fossa
Statistics from Altmetric.com
Introduction
Flow diverters (FDs) have been increasingly used in the treatment of intracranial aneurysms, predominantly in the anterior circulation.1–6 The framework of these devices has higher surface coverage and lower porosity than conventional intracranial stents, and may provide scaffolding for endothelialization and vessel wall healing. The porosity is thought to allow flow preservation to small covered perforators due to demand.
Although several devices are in development, the Pipeline device (eV3/Codman, Irvine, California, USA) is the only Food and Drug Administration-approved device in the USA since 2011. It is constructed from a 25% platinum and 75% nickel–cobalt–chromium alloy with about 30–35% surface area coverage, depending on the degree of spread during deployment. The Silk device (SFD, Balt Extrusion, Montmorency, France) has been used in Europe since 2007. It is a 48-strand nickel–titanium (nitinol) alloy with platinum microfilaments, and has a 35–55% surface metal coverage and a pore size 110–250 µm. Among others, the Surpass (Stryker, Kalamazoo, Michigan, USA) and FRED (Microvention, Tustin, California, USA) devices are currently in clinical trials.
Flow diversion is usually considered to carry lower risks for large, wide-necked, dysplastic aneurysms in the proximal anterior circulation without significant perforator vessels in their vicinity. These devices emerged as a potential option for previously untreatable or ‘treatment-failure’ aneurysms. One of their main advantages is that they represent a reconstructive technique that preserves the parent vessel, and may result in the involution/regression of the aneurysm sack and consequently decrease the mass effect.3 ,4 The Pipeline device showed promising initial results, with high angiographic occlusion rates at the 1-year follow-up.1 Accumulating, but still limited, data are available for the application of these devices in the posterior circulation.5–10 Other than the well-known potential complications in the anterior circulation,11 ,12 including delayed rupture, delayed parenchymal hemorrhage, and mass effect, in-stent thrombosis and perforator ischemia are a particular challenge in the use of FDs in fusiform posterior circulation aneurysms.7 ,13
We present our experience in a case series of seven aneurysms in six patients with FD placement in posterior circulation vessels and compare our results with previous reports.
Methods
In accordance with the local institutional review board, retrospective review of material and case logs for use of flow diversion in posterior circulation aneurysms was performed. A total of seven aneurysms in six consecutive patients were treated in our institution between November 2011 and November 2013. Before implantation, written informed consent was obtained from the patients. Significant therapeutic and clinical uncertainties and off-label device use were discussed explicitly with the patients and their families. Patients were selected with aneurysms deemed to have a high risk of failure with conventional endovascular or surgical methods, with previous treatment failures, recurrences, and fusiform and large aneurysms with mass effect.
All patients were treated with clopidogrel 75 mg/day and aspirin 325 mg/day for 5 days before the procedure. We conducted standardized laboratory-based light transmission aggregometry from whole blood to assess the medication effect and platelet inhibition. Adequate platelet response was verified by arachnoid acid and ADP aggregation assays. In accordance with the institutional standard, aspirin and clopidogrel response were considered adequate if the arachnoid acid-induced aggregation was <20% (ie, inhibition was >80%) and ADP-induced aggregation reached <40% (ie, inhibition was >60%). When the response was inadequate, patients were given an additional medication dose, and aggregometry was rechecked. No cases of aspirin non-responders were seen. In one patient, clopidogrel was switched to prasugrel 10 mg/day, because of consistent failure to achieve adequate platelet inhibition despite an increased clopidogrel dose and repeat medication loading. All patients also received an intravenous heparin bolus at the beginning of the procedure with additional boluses as needed for a target activated thromboplastin time of 250. Activated thromboplastin times were followed and adjusted consistently during the procedure.
General endotracheal anesthesia was used in all cases. After obtaining femoral access and initial diagnostic angiographic images, a six or seven French shuttle sheath was advanced into the target parent vessel. Working projection for FD deployment was determined from a 3D rotational angiogram. Selection of the FD device size was based on the proximal and distal parent vessel diameters. A triaxial catheter system, consisting of a shuttle sheath, intermediate catheter and microcatheter, was used to reach the aneurysm. If adjunctive coiling was deemed necessary, a standard microcatheter was advanced (‘jailed’) into the aneurysm lumen before FD placement. The FD was deployed through a Marksman microcatheter (eV3/Covidien, Irvine, California, USA). A Pipeline device (eV3/Covidien) was used in all patients. The number of devices used was at the discretion of the operator. Multiple devices were usually deemed necessary in cases of fusiform or very wide neck aneurysms for better FD effect, or to span the aneurysm neck or lumen. Follow-up angiography and/or MRI was carried out in all patients.
Patient demographics and aneurysm characteristics were obtained from medical charts. Technical success, complications, clinical outcome and imaging follow-up were determined. Aneurysm occlusion rates were graded on the O’Kelly-Marotta scale,14 grade D1 representing complete occlusion. All complications possibly related to the device or procedure were investigated. We reviewed the literature by searching the PubMed database with ‘posterior circulation/basilar flow diverter’, ‘posterior circulation/basilar flow diversion’ keywords. Case series with more than five posterior circulation aneurysms were included.
Results
Seven aneurysms in six patients were treated in our institution between November 2011 and November 2013 (table 1).
Our seven posterior circulation aneurysm cases in six patients
Five aneurysms were saccular, and two were fusiform. Patients comprised four men and two women, between the ages of early 30s and mid-60s (mean age 51.4 years). The average aneurysm maximal diameter was 18.1 mm (ranging from 7 to 29 mm), and maximum aneurysm length was up to 52 mm (in a fusiform aneurysm). None of the aneurysms were acutely ruptured, but one patient had a history of questionable subarachnoid hemorrhage years previously, with no records available. This latter patient had two aneurysms, one on each distal intracranial vertebral artery, which were treated separately, 3 months apart (therefore cases No 2 and No 3 are the same patient, treated at different times). All but one patient was symptomatic, with symptoms ranging from worsening headaches to cranial neuropathies, transient ischemic attack, and ischemic stroke. The remaining patient had aneurysm recurrence on follow-up imaging after multiple coiling procedures for an incidentally found posterior cerebral artery (PCA) aneurysm. No patients had previous intracranial stent treatment.
Locations included three basilar arteries, three distal vertebral arteries, and one PCA aneurysm. FDs were placed successfully in all patients. Additional coiling was used in three (42.9%) cases. We used an average of two pipelines for each patient (range 1–5 per patient). Imaging and clinical follow-up was available in all cases, ranging from 3.5 to 28 months (mean 14.5 months). Complete angiographic occlusion was seen in four out of seven cases (57.1%), but one of these cases was due to thrombosis of the entire Pipeline construct secondary to medication non-compliance (case No 6). The latter patient had no clinical complications initially after surgery, but developed in-stent thrombosis with a large brainstem stroke at 4.5 months, a week after the patient self-discontinued dual antiplatelet therapy without notifying the treating physician. There were no other cases of medication non-compliance. The remaining three patients (42.9%) had decreased residual filling on follow-up.
Other clinical events included one patient with a periprocedural stroke with moderate residual deficits and subsequent death (14.3% mortality) from ‘medical complications’ 18 months after the procedure (case No 1), and two other patients with a small periprocedural stroke with excellent recovery (case Nos 3 and 7). One of the latter two patients developed acute intraprocedural in-stent thrombosis, which was rapidly treated (case No 7), and had no significant long-term clinical consequences other than minimal unilateral arm ataxia. The other patient with periprocedural stroke (case No 3) had no obvious angiographic abnormality during FD deployment, but postoperative examination and imaging demonstrated an ischemic stroke; clinical follow-up 2 years later showed no significant residual deficits. No intracranial hemorrhages or delayed ruptures were seen. Overall, four out of our six patients (66.7%), or five of seven cases (71%), had very good clinical outcomes (modified Rankin score (mRS) 0–1).
Illustrative cases
Case No 1
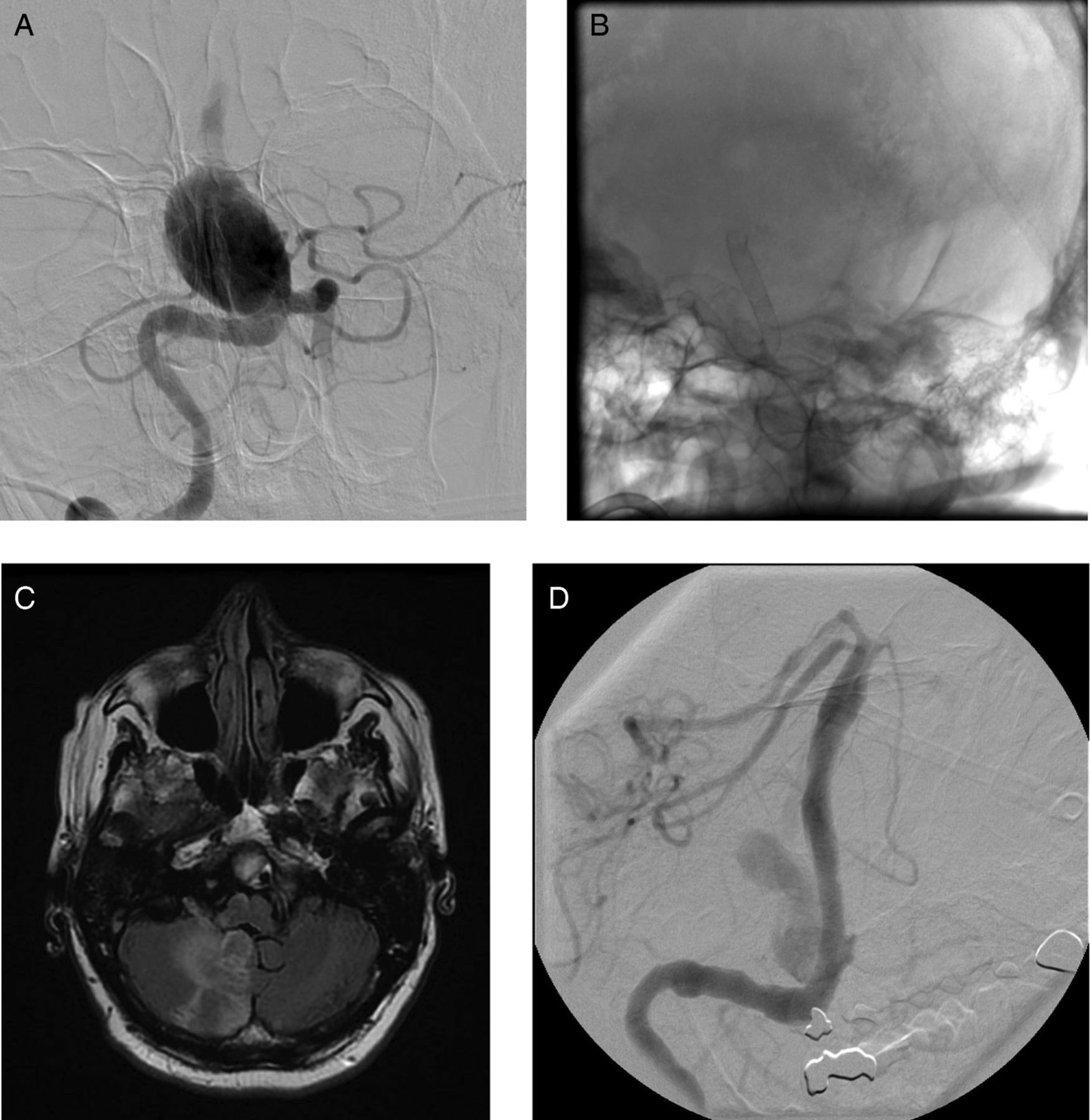
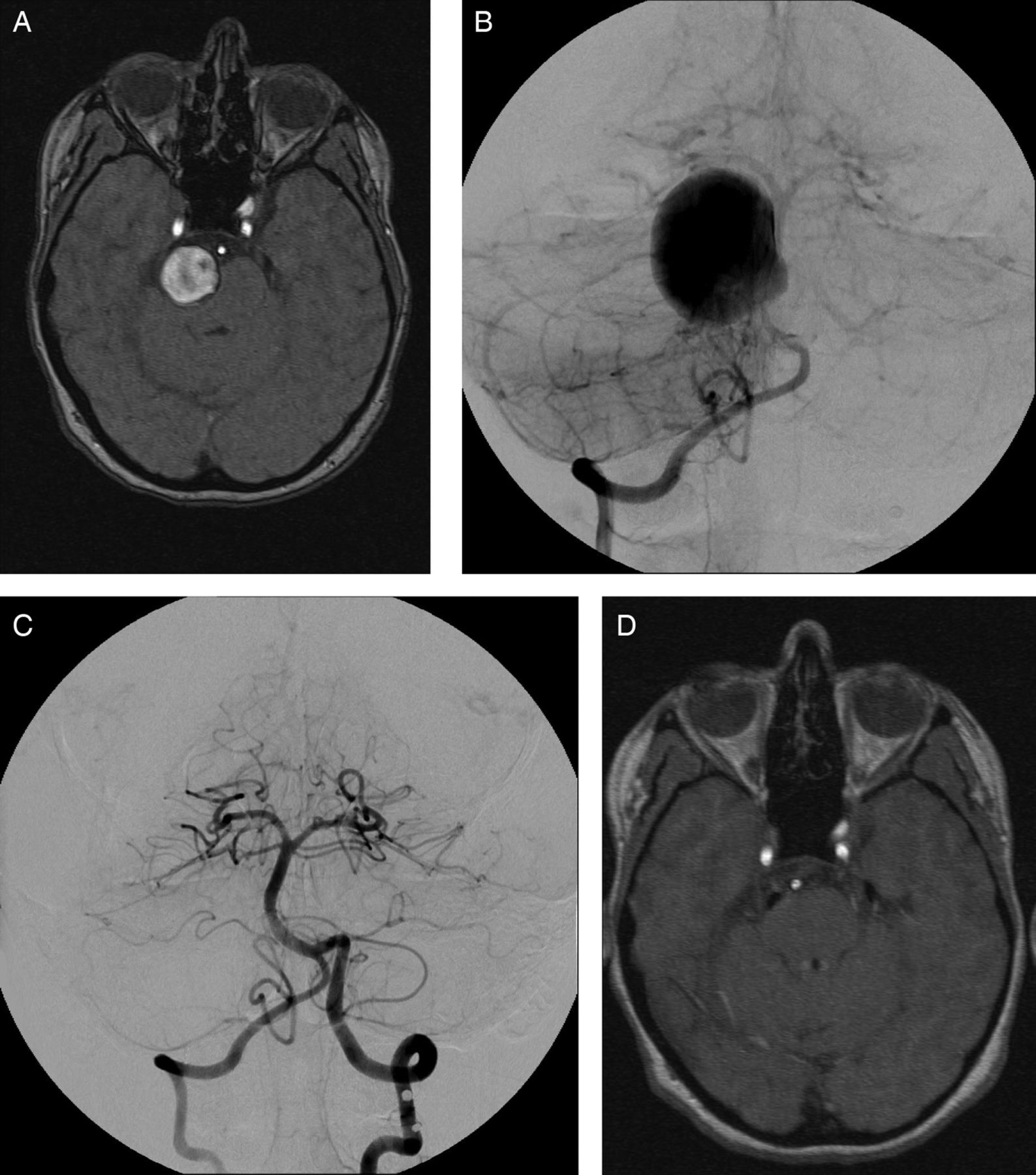
A patient in his/her 60s presented with left-sided weakness and slurred speech, and was diagnosed with a stroke and a large fusiform basilar aneurysm 10 months before treatment (figure 1A) with two overlapping Pipeline devices (figure 1B). The patient developed a sizeable right anterior inferior cerebellar arteries–posterior inferior cerebellar artery (AICA–PICA) distribution stroke (figure 1C) after the procedure, with cranial nerve palsies, dysarthria, and dysphagia, requiring feeding tube placement. The patient was discharged to acute rehabilitation in a different state. A 1-month follow-up MRI and angiogram (figure 1D) showed no new strokes, and markedly decreased aneurysmal filling. The mRS at that time was 4, but then the patient was lost to follow-up, having requested an out-of-state transfer to a rehabilitation facility close to home. Recently, a family member disclosed that the patient had died (mRS 6) about 18 months after his FD placement owing to ‘medical problems’, but no further details were available.
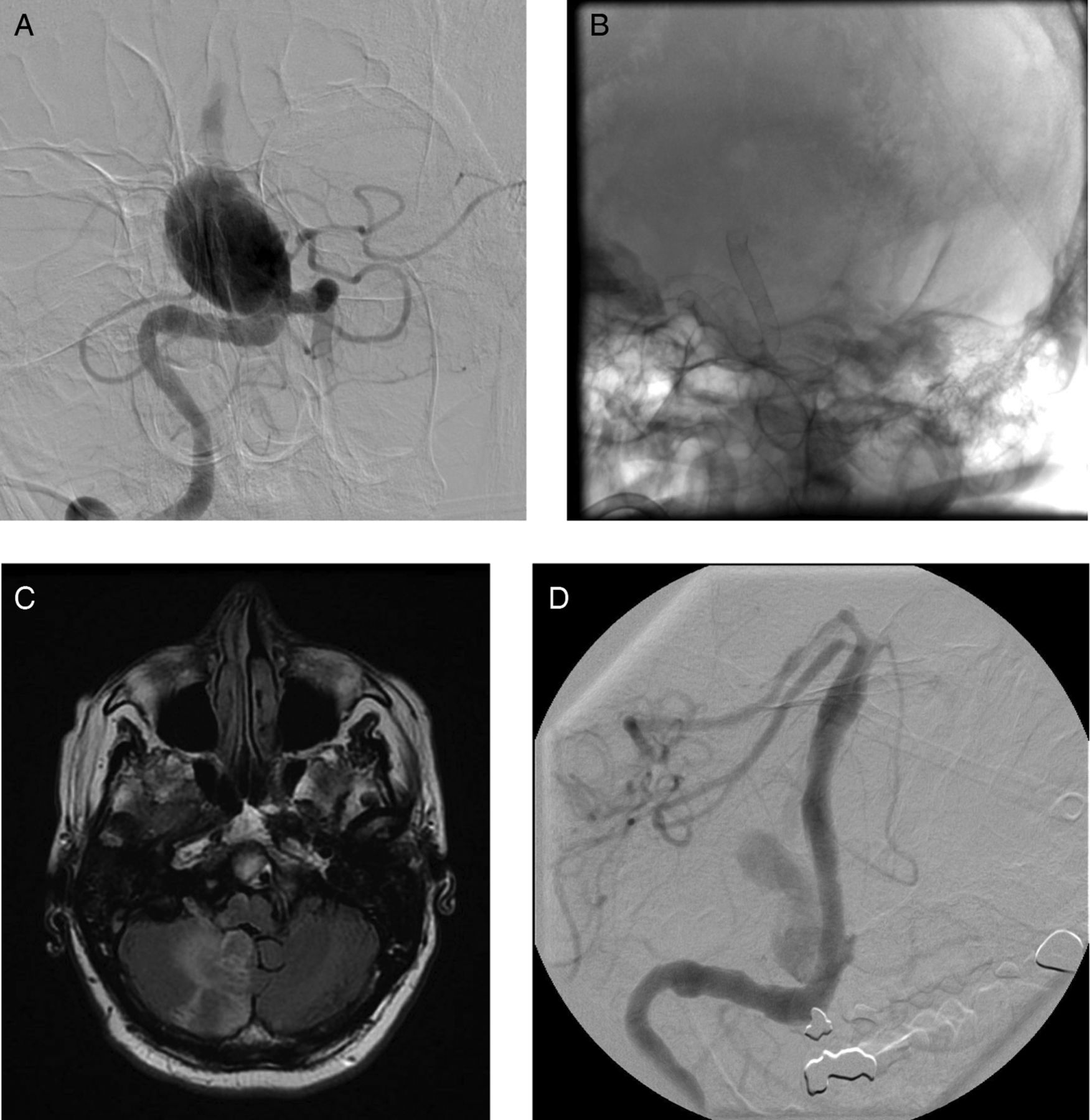
Giant fusiform basilar aneurysm (case No 1). (A) Angiogram before treatment showing limited filling of the basilar apex owing to significant stagnation of contrast in the aneurysm lumen. (B) Native angiogram showing the long pipeline construct (two devices) after treatment. (C) Right anterior inferior cerebellar arteries–posterior inferior cerebellar artery (AICA–PICA) stroke after device placement on MRI. (D) One-month follow-up angiogram showing markedly decreased, but persistent, filling of the original aneurysm with better opacification of the basilar apex.
Case No 4
A patient in their 30s with a history of five cigarettes/week smoking, and no other past medical history presented with worsening right retro-orbital headache and new-onset right trigeminal nerve distribution paresthesias over 2 months, followed by 2 weeks of new diplopia with right abducens nerve paresis. There was no family history of aneurysms, subarachnoid hemorrhage, or collagen vascular disease. Investigation showed a giant basilar sidewall aneurysm with mass effect and significant compression of the pons and midbrain structures (figure 2A). No associated hydrocephalus was seen. Angiographic images showed delayed, limited filling of the basilar apex and distal posterior circulation vessels (figure 2B), and small bilateral posterior communicating arteries. The AICA were difficult to identify, but were suspected to originate at the base of the giant aneurysm. FD treatment was performed with two Pipeline stents in an overlapping fashion. Immediate stagnation was noted in the aneurysm. The patient had transient dysarthria, dysphagia, and generalized weakness immediately after the procedure, which rapidly improved. Post-procedural head CT showed progressive thrombosis of the aneurysm with minimal filling of the aneurysm sac at 5 days. Steroid treatment was maintained for 3 weeks after the procedure for presumed mass effect. The patient was discharged home on day 7. A follow-up angiogram at 7 months showed complete aneurysm occlusion with patency of the AICA (figure 2C). MRI at 12 months showed no significant residual aneurysm filling and marked regression of the large aneurysm sack (figure 2D). The patient had only mild, improved residual facial and body sensory deficit (numbness) at 1 year. Intermittent diplopia (pre-existing symptom) had resolved. The patient was able to go back to work full time, take yoga classes, and travel (mRS 1).
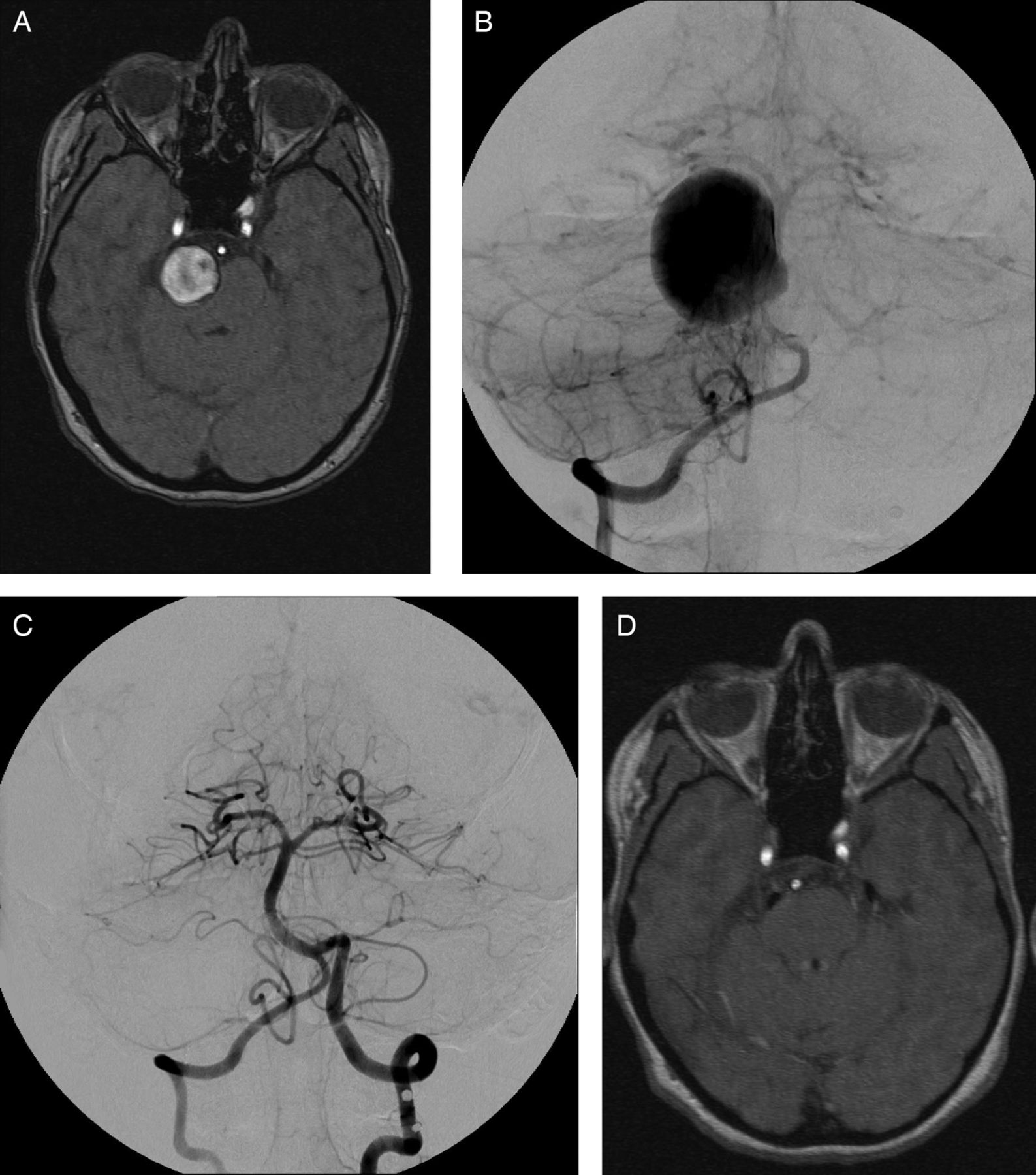
Giant sidewall basilar aneurysm (case No 4). (A) Preoperative T2 MRI sequence demonstrating brainstem compression. (B) Anteroposterior (AP) angiogram before treatment showing the aneurysm with limited basilar apex filling due to contrast stagnation in the aneurysm lumen. (C) A 7-month follow-up AP view angiogram showing no residual aneurysm filling and patency of bilateral anterior inferior cerebellar arteries. (D) A 1-year follow-up MRI showing resolved mass effect and brainstem compression.
Case No 5
A quinquagenarian with a history of hypertension, obesity, and previous head injury presented with worsening headaches. Imaging demonstrated a large dissecting aneurysm of the dominant right vertebral artery adjacent to the PICA origin (figure 3A,B). The patient showed suboptimal response to clopidogrel on multiple reloading and increased (150 mg) daily dosage, and was eventually switched to prasugrel 10 mg/day, while continuing aspirin 325 mg/day. Uneventful Pipeline placement with adjuvant coiling of the aneurysm lumen was performed. A 6-month follow-up angiogram showed no residual aneurysm (figure 3C). The patient's post-procedure clinical status was mRS 0 and National Institutes of Health Stroke Scale 0. The patient's headaches resolved.

Dissecting right vertebral aneurysm adjacent to posterior inferior cerebellar artery origin (case No 5). (A) Lateral magnified angiographic view before treatment. (B) Anteroposterior (AP) angiographic view before treatment. (C) A 6-month follow-up AP angiogram showing no residual aneurysm.
Case No 6
Another quinquagenarian with uncontrolled hypertension and heavy smoking, who initially presented 2 years before endovascular treatment with small patchy posterior circulation strokes, was found to have a giant partially thrombosed vertebrobasilar aneurysm (figure 4A,B). No intervention was offered at that time owing to the risks, but treatment was started with antiplatelet and blood pressure medications. The patient presented with new symptoms of weakness and dysarthria 16 months after the initial event, and underwent ventriculoperitoneal shunt placement for hydrocephalus, with good clinical recovery. The patient re-presented with recurrent ataxia, vertigo, slurred speech, and left-sided weakness 8 months later. Imaging demonstrated further growth of the known fusiform vertebrobasilar aneurysm with significant mass effect and brainstem compression (figure 4C). After multiple considerations, FD treatment was offered. The importance of compliance with the medication was discussed on numerous occasions with the patient and family. A total of five Pipeline stents were deployed in a telescoping fashion from the distal basilar artery to the distal right vertebral segment, just distal to the right PICA origin (figure 4D). The left vertebral artery was sacrificed with endovascular coiling. Angiographic follow-up at 6 days showed significant residual filling of the aneurysm lumen. The patient was able to return home after a short rehabilitation stay, but afterwards had several missed clinic appointments and a 3-month missed MRI/angiography follow-up due to non-compliance and social problems. However, the patient was doing well clinically until 4.5 months after the procedure, but then re-presented with a loss of consciousness and coma. The patient's spouse reported that the patient had self-discontinued both aspirin and clopidogrel without consulting our team, because she/he was ‘feeling a lot better’. Imaging showed complete occlusion of the vertebrobasilar construct and basilar artery (figure 4E) with significant ischemia of the brainstem and occipital lobes (figure 4F). Although there was no residual filling of the aneurysm (occlusion grade D1), this was due to thrombosis of the entire Pipeline construct secondary to medication non-compliance. The family requested maximal medical management despite poor prognosis. The patient left the hospital for a long-term care facility with an mRS of 5. Although the last angiographic follow-up was at 4.5 months, a recent review of medical records showed that the patient was still alive 9 months after the procedure, with no clinical improvements.

Giant partially thrombosed vertebrobasilar fusiform aneurysm (case No 6). (A) Pretreatment angiogram, anteroposterior view. (B) Aneurysm size and brainstem compression in 2011 on FLAIR MRI sequence. (C) Marked aneurysm growth in 2013 compared with 2011 (MRI FLAIR). (D) Long 5-device construct from the distal basilar to the mid right V4 segment. Left vertebral artery was coil sacrificed. (E) In-stent thrombosis of the Pipeline construct at 4.5 months, after medication non-compliance. (F) MRI (FLAIR) demonstrating major posterior circulation ischemic changes after stent thrombosis. FLAIR, fluid attenuated inversion recovery.
Case No 7
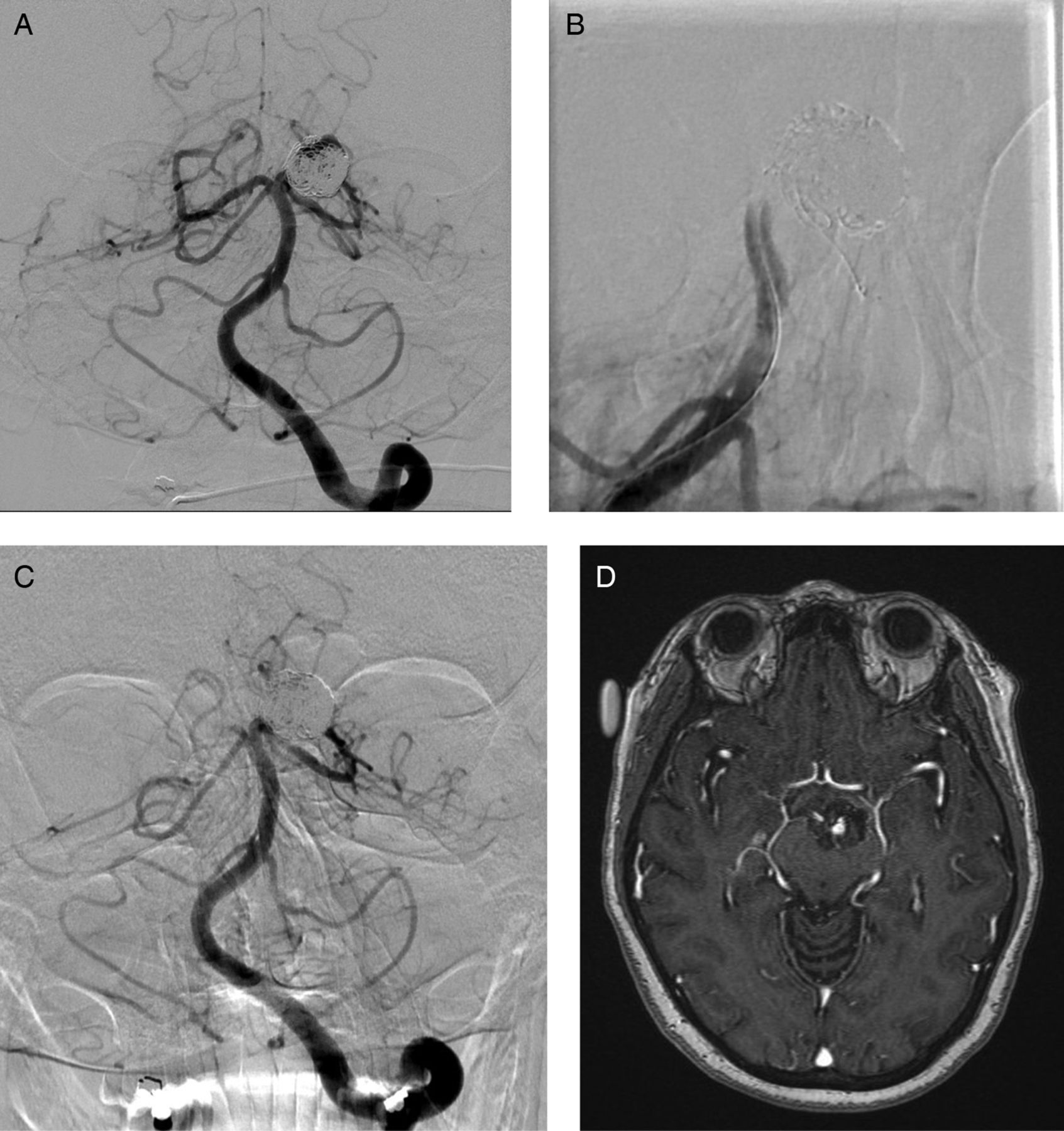
A sexagenarian presented for evaluation of a recurrent left proximal P1 segment aneurysm, which had been incidentally found during an investigation for deviated nasal septum surgery 5 years previously. The patient had undergone recoiling without stent placement four times previously, with significant recurrence on the last follow-up (figure 5A). A single FD device was placed extending from the left P1 to the distal basilar artery, with subsequent acute in-stent thrombosis (figure 5B). Intra-arterial abciximab was administered locally via microcatheter, followed by gentle balloon angioplasty of the stent, resulting in successful recanalization. The patient had transient right facial droop and right-sided weakness after the procedure. An angiogram next day showed patent vessels and reduced flow to the aneurysm lumen (figure 5C). A 3.5-month follow-up showed slight residual right upper extremity ataxia and occasional mild imbalance (mRS 1) with mild residual filling of the aneurysm on MRI imaging (figure 5D). The patient has not yet had 6-month angiography, but we believe that there is a reasonable chance of further occlusion of the aneurysm by the next follow-up.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Left P1 posterior cerebral artery (PCA) recurrent aneurysm. (A) Anteroposterior angiogram before treatment with flow diverters showing significant filling at the coil mass. (B) Intraprocedural transient in-stent thrombosis with lack of filling at the basilar apex. (C) Angiogram 1 day after treatment showing decreased aneurysm filling and patent vessels. Right PCA is washed out from the anterior circulation via posterior communicating artery. (D) A 3-month follow-up contrast MRI showing small residual filling of the aneurysm.
Discussion
Posterior circulation aneurysms are a heterogeneous disease group including sidewall, bifurcation, dissecting, saccular, and fusiform aneurysms. The natural history of the different aneurysm types is not well known. In the International Study of Unruptured Intracranial Aneurysms (ISUIA), the rupture rate for posterior circulation aneurysms >7 mm was 3–10% a year, although no fusiform or atypical aneurysms were included.15 ,16 Fusiform, large or giant partially thrombosed, expanding aneurysms appear to present a particularly high risk owing to the added risks of mass effect, brainstem compression, and thromboembolic events from perforator vessels.7 ,12 ,13 A recent study reported deaths occurring in three patients with atypical posterior circulation aneurysms who were waiting for treatment.7 Rapidly changing or expanding posterior circulation aneurysms have also been described.17
Different aneurysm types and locations in the posterior circulation are also thought to represent variable treatment risks. In a large series, overall poor outcome or death was seen in 40% of patients treated for fusiform posterior circulation aneurysms.18 Not surprisingly, poorer surgical (RR=1.9, p=0.025) and endovascular (RR=2.25, p=0.02) outcome was seen in ISUIA for posterior circulation aneurysms than for anterior circulation.16 A similar trend has been described in a recent meta-analysis of intracranial FDs, which included 29 reports, 1451, patients and 1654 aneurysms. Ischemic strokes and perforator infarctions were significantly higher in the posterior circulation, although there was no difference in subarachnoid hemorrhage and intracranial hemorrhage rates.19
There is usually significant dilemma about treatment indications for these challenging aneurysms, which clearly have an unfavorable natural history, and also, an increased risk of treatment. In most large tertiary care centers, intervention is usually considered necessary if new symptoms develop, and/or there is evidence of change in morphology over time, prior hemorrhage, expansion, or progressive posterior circulation mass effect.
Flow diversion emerged a few years ago as a potential option for intracranial aneurysms. Available studies reporting on the use of FDs in the posterior circulation, however, show highly variable results and complication rates. A retrospective review of seven symptomatic (stroke, ataxia, numbness, headache) patients between the ages of 42 and 75 years with unruptured large (8.5–35 mm) fusiform basilar aneurysms, showed that Pipeline was used in 6, and a Silk device in one patient.7 The number of stents used was 3–9 per patient. Antiplatelet medication response testing was performed. Additional coiling was used in four patients. Preoperative mRS ranged from 1 to 4, while postoperative outcomes were less favorable with mRS 5–6 in five patients (four died) and mRS 0 and 1 in the other two. Postoperative brainstem ischemia was seen in five patients, subarachnoid hemorrhage in one. The authors concluded that flow diversion did not appear safe for fusiform basilar aneurysms.
A large Australian series reported FD treatment in 32 patients.9 A large portion of these lesions were asymptomatic (20/32). Only four patients had mass effect, and eight developed subarachnoid hemorrhage. Twelve aneurysms were saccular, while the remaining 20 comprised fusiform, blister, sidewall, or dissecting lesions, but no exact itemization was published. Additional coiling was done in 11 patients. Dual antiplatelet therapy was used without platelet inhibition testing, but postoperative heparin therapy was continued for at least 13 h. No patients died. Perforator infarct was seen in three (14%) of 21 basilar aneurysms, and there were two asymptomatic intracranial hematomas. Overall permanent neurologic deficit was noted to be 9.4%. The occlusion rate was 96% at 1 year in patients available for follow-up, but only 23 of 32 patients (71.9%) had ≥1 year follow-up. The authors concluded that FDs were safe for posterior circulation aneurysms that cannot be treated with conventional endovascular techniques.
A German report of 101 FD-treated aneurysms included 22 posterior circulation lesions.5 The authors reported three out of five major complications in the study occurring in the posterior circulation: two cerebellar hemorrhages and one fatal stent thrombosis 2 weeks after stopping clopidogrel.
A European retrospective review of 12 patients with 10 symptomatic and two incidental basilar trunk and superior cerebellar artery (SCA) aneurysms treated with the Silk device described four strokes (three late in perforator distributions), and two cases of in-stent thrombosis, but no deaths.10 The aneurysm occlusion rate was 58% during the mean follow-up of only 16 weeks.
Another recent case series included seven patients with two incidental and three recurrent aneurysms, one patient with headache, and one brainstem compression.8 There were three fusiform and four saccular distal vertebral, basilar and vertebrobasilar junction 6–25 mm aneurysms. Pipeline was deployed in all seven patients, with 1–3 stents for each case. Additional coiling was used in one patient. Follow-up was available for six patients at 3–7 months (mean 5.5). Pre- and postoperative mRS assessments were not specified. Complete occlusion was achieved in three (42.9%), decreased aneurysm filling in two (28.6%), and no change in one (14.3%). There was no significant morbidity or mortality. No perforator infarcts or hemorrhage were seen. The authors concluded that flow diversion in the posterior circulation may be safe in selected patients. They hypothesized that their results were more favorable than earlier ones, because of avoiding overlapping FDs in the perforator rich basilar trunk, minimizing the number of stents used per patient, and adhering to a strict antiplatelet protocol. Although they only had one aneurysm of such type (the other two fusiform aneurysms involved the vertebral arteries only), the authors also concluded that the most difficult entity with the worst outcome appeared to be the fusiform basilar aneurysm with a pre-existing mass effect. This observation is similar to that in other studies (such as Siddiqui et al, described above),7 and in ours.
In another series of 70 patients with FD treatment, 20 had posterior circulation saccular (nine patients) and fusiform (11 patients) aneurysms: 10 vertebral, 2 PICA, 2 AICA, 1 SCA, 5 basilar trunk.6 The median follow-up was only 119 days. Additional coils were used in 14% of all cases. Permanent neurologic deficit was seen in one (5%) patient, and mortality (from thromboembolism and mass effect) was 10% in the posterior circulation. It is not reported if complications were more common in patients with fusiform aneurysms. Complete aneurysm occlusion was seen in 49% (95% CI 35% to 63%) of all (anterior and posterior circulation) cases.
As summarized in table 2, there is significant variability in mortality, permanent new morbidity, and occlusion rates of posterior circulation aneurysms treated with FD. These studies have several limitations. Interpretation of the results is difficult owing to heterogeneity of the patients and aneurysms, relatively short follow-up, retrospective analysis, and relatively small total numbers.
Comparison of recent studies with posterior circulation flow diverter treatment
One of the important observations from the overall outcomes is that mortality and morbidity appear to be higher with symptomatic aneurysms. This poses a difficult clinical dilemma, because, reasonably, physicians feel obliged to offer treatment when symptoms are present to prevent further decline. Unfortunately, it is not known what percentage of the incidentally discovered asymptomatic aneurysms would go on to become symptomatic over time. The challenging question is whether it is worth considering treating asymptomatic posterior circulation aneurysms earlier when they may be a lower treatment risk, or waiting to treat until they become symptomatic, less stable, and the risk of intervention is greater.
The other finding is in line with prior opinions that fusiform basilar aneurysms have the highest treatment risks,7–9 probably owing to extensive involvement of perforators. These aneurysms have unfavorable characteristics for any treatment, including flow diversion. The fate of small perforator arteries is difficult to predict. There is no good understanding of the dynamics of aneurysm thrombosis around a ‘free-floating’ FD stent in a large and elongated fusiform vessel segment. In particular, increased distance from the device wall to the perforator vessel origin seems to be very important. We agree with other authors8 that the higher number of stents may also contribute to an increased risk of complications, probably owing to overlapping coverage of the small perforators, more metal and foreign body presence, increased risk of ischemic events, and longer procedure times. The advances in computational flow dynamics and similar hemodynamic simulation techniques may shortly become useful to model these aneurysms and devices.20 They might assist in the development of less risky, better optimized treatment plans, individualized for each patient.
An important component of preventing perforator infarcts or other ischemic complications is the strict adherence to the obligatory dual antiplatelet therapy. Non-compliance is a rare, but dreaded problem in patients with intravascular stents.5 An unfortunate example is our patient (case No 6) who decided to discontinue his medication despite extensive education about the importance of this treatment. Life-threatening consequences should be explicitly discussed with the patient and family before proceeding with FD treatment.
The use of antiplatelet inhibition testing appears important and provides guidance about the effect of treatment; however, significant thrombotic or hemorrhagic events may still occur despite adequate testing.7 On the other hand, some of the studies featured in this paper had good outcomes with limited or no standardized testing,6 ,9 ,10 clearly indicating the importance of other factors discussed above (aneurysm size, shape, exact location, perforators, number of stents, compliance, etc). Operators should use the testing method with which their practice has the most experience, until further data are available.
No significant post-treatment subarachnoid hemorrhage was seen in our patients, but the importance of adjunctive coiling has been raised by others, especially to reduce the risk of early rupture in the initial phase after FD placement.7 ,8 We usually choose to use coils in aneurysms with a ‘jet-effect’—for example on the outer curvature of the vessel, and/or if a mass effect is less of a concern.
Despite the considerable challenges and increased morbidity/mortality rates, in all but one selected studies good clinical outcome (mRS 0–2) was reached in over 70% of patients (table 2). The average permanent neurologic deficit rate was 11.0%, and mortality 12.3%. Complete occlusion rates were between 43% and 100% (average 74%), but the percentage of patients available for follow-up was as low as 48% in some studies. Results also varied greatly depending on aneurysm type and length of follow-up. Importantly, the outcomes appeared markedly worse for fusiform basilar aneurysms than for other types in most studies. While these results are clearly suboptimal, these lesions are exceptionally challenging owing to the previously discussed anatomical considerations, and flow diversion is a relatively new area in the neuroendovascular field. Further advancements may provide more optimal solutions for these complex lesions.
Conclusions
Atypical posterior circulation aneurysms with complex flow dynamics remain challenging to treat. The combination of unfavorable natural history and increased treatment risks make medical decision-making and patient counseling particularly problematic. Based on our results and previous reports, we advise caution with symptomatic and fusiform large aneurysms in the posterior circulation, which appear to have higher treatment risks than other types. However, favorable results can be achieved with FDs in selected patients with otherwise no optimal therapeutic options. These procedures should preferably be performed in high-volume centers with the most experience. Extended follow-up of previously treated patients will be valuable to better understand the long-term risks and benefits of flow diversion. Newer-generation devices and computational flow dynamic models may help in tailoring treatment to individual patients in the future. Further prospective data are necessary to assess the role of flow diversion in the posterior circulation.
References
Footnotes
Correction notice This article has been corrected since it was published Online First. The first column in table 2 is now included.
Contributors GT: conception and design, data collection and analysis, data interpretation, manuscript preparation, study supervision. MB: data collection, data interpretation and manuscript review. SM: data collection and manuscript review. MSH, TM, PR, FH: data interpretation and manuscript review.
Competing interests PR: eV3—institutional research and educational support; Penumbra—stock holder; Codman—honoraria, Blockade Medical—investor, scientific advisory board.
Ethics approval Institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.