Article Text

Abstract
Background Use of the Pipeline embolization device (PED) in the posterior circulation is of some controversy.
Objective Recent publications have described adverse outcomes associated with the PED for vertebral and/or basilar artery pathology. We assessed our results in the treatment of this challenging subset of aneurysms after Food and Drug Administration (FDA) approval.
Methods We prospectively reviewed our series of PED cases in this cohort. Patients were assessed for aneurysm type, technical success, periprocedural complications, and aneurysm obliteration.
Results Since FDA approval, 17 patients with posterior circulation aneurysms were treated with the PED. These included aneurysms of the vertebral artery (V4) segments (n=8), basilar trunk (n=6), basilar apex (n=2), and cervical vertebral artery (n=1). Two patients had a prior subarachnoid hemorrhage. All of the aneurysms treated were either saccular, had a saccular component, or were dissecting in nature. No dolichoectatic aneurysms were treated. Technical success was achieved in all patients. One complication (1/17 patients; 5.9%), a parenchymal hematoma after ventriculostomy replacement, resulted in permanent disability. Angiographic follow-up has been obtained to date in 14 of the 17 patients and shows complete or near-complete (>90%) obliteration in all cases.
Conclusions Patient selection is essential for safe and effective PED treatment of posterior circulation aneurysms. The PED is equally effective in achieving aneurysm obliteration with an acceptable risk profile as it is in the anterior circulation. Dolichoectatic aneurysms were not included in this treatment cohort. PED may be a preferable alternative to open surgical treatment of posterior circulation aneurysms.
- Device
- Complication
- Flow Diverter
Statistics from Altmetric.com
Introduction
The efficacy and safety profiles of the Pipeline embolization device (PED) in treating wide-necked anterior circulation aneurysms are well described,1 but the same cannot be said for posterior circulation aneurysms. Recently, small series have reported adverse outcomes in this aneurysm subgroup treated with the PED.2 ,3
A number of anatomic factors potentially complicate the endovascular treatment of posterior circulation aneurysms and often necessitate the use of complex endovascular approaches. Aneurysm location and the large numbers of perforating and branching arteries further expose the patient to thromboembolic and ischemic complications.
Issues pertaining to antiplatelet therapy are another source of complications. Dual antiplatelet treatment is integral to the maintenance of patency through the construct. Hemorrhagic complications including persistent epistaxis, gastrointestinal hemorrhage, menorrhagia, and easy bruisability can force the cessation of one or both antiplatelet medications. A lack of responsiveness to antiplatelet therapy also enhances the likelihood of thromboembolic sequelae.
In light of these potentially complicating issues, we undertook a prospective review of posterior circulation aneurysms treated with the PED.
Methods
We prospectively analyzed all patients treated with the PED at our institution following Food and Drug Administration (FDA) approval. We separately evaluated patients with posterior circulation aneurysms. Patient demographic data as well as aneurysm location, anatomic type, number of devices used, angiographic follow-up and complications were assessed. This study was conducted with the approval of our Institutional Review Board.
Dual antiplatelet therapy, including 325 mg aspirin and 75 mg clopidogrel was started at least 3 days prior to the procedure, except in the setting of a subarachnoid hemorrhage (SAH). In this case, a loading dose of intravenous abciximab was administered during the procedure. Platelet inhibition was monitored in all patients and dosages were modified in order to achieve an adequate therapeutic effect. All but two patients were maintained on both aspirin and clopidogrel for at least 6 months after treatment. One patient with SAH demonstrated resistance to clopidogrel, prasugrel and ticlopidine, although the patient did respond to aspirin. This patient was treated initially with aspirin and heparin and then transitioned to warfarin after removal of the ventriculostomy. Three months after treatment, warfarin was discontinued and the patient was maintained on a single daily aspirin. The second patient demonstrated clopidogrel resistance and was treated with a combination of aspirin and prasugrel.
Standard angiographic techniques for catheterization and device deployment are well-described in the literature and were employed in this series. When aneurysms were coiled, a separate microcatheter was jailed within the aneurysm prior to stent deployment. Patients were heparinized to achieve activated clotting times of 250–300 s. All procedures were performed under general anesthesia with electrophysiologic monitoring.
Results
Seventeen patients with posterior circulation aneurysms were treated at our institution following FDA approval of the PED in May 2011. Patients ranged in age from 32 years to 79 years and included nine men and eight women (table 1). Aneurysm locations included: V4 segment (n=8), basilar trunk (n=6), basilar apex (n=2), and cervical vertebral artery (n=1). On average, 2.1 devices were used per patient (range 1–8).
Patient demographics
All patients were evaluated for complications within the 30-day periprocedural period and at the time of their last angiographic follow-up. Five intraprocedural or periprocedural complications occurred. Of these five complications, four were transient and included retention of the distal PED wire, silent thrombosis of the proximal superior cerebellar artery (SCA), a small cerebrovascular accident (CVA), and a urethral tear during Foley catheter placement. One permanent complication (1/17, 5.9%), a parenchymal hematoma after ventriculostomy replacement, resulted in permanent disability.
Fourteen patients were eligible for angiographic follow-up. This ranged from 3 months to 27 months with an average of 11.8 months. Of the 14 patients, 11 demonstrated complete aneurysm occlusion and 3 near-complete (>90%) occlusion.
Illustrative cases
Patient 3
This patient presented in a moribund condition following rupture of a left V4 dissecting aneurysm. The patient's condition continued to deteriorate secondary to a myocardial infarction requiring the insertion of an intra-aortic balloon pump. Angiography demonstrated a hypoplastic right vertebral artery and a dominant left vertebral artery (figure 1A). We performed a reconstructive approach employing two telescoping PEDs (figure 1B). The details of the antiplatelet and anticoagulation regimen are discussed above. Despite the patient's poor presentation and protracted hospital course, the patient recovered fully after rehabilitation. The details of the treatment and immediate angiographic outcome have been previously published.4 Twenty-seven months after treatment, angiography revealed complete remodeling of the vessel wall and no evidence of recurrent aneurysm (figure 1C). The patient remains on a single adult aspirin per day.
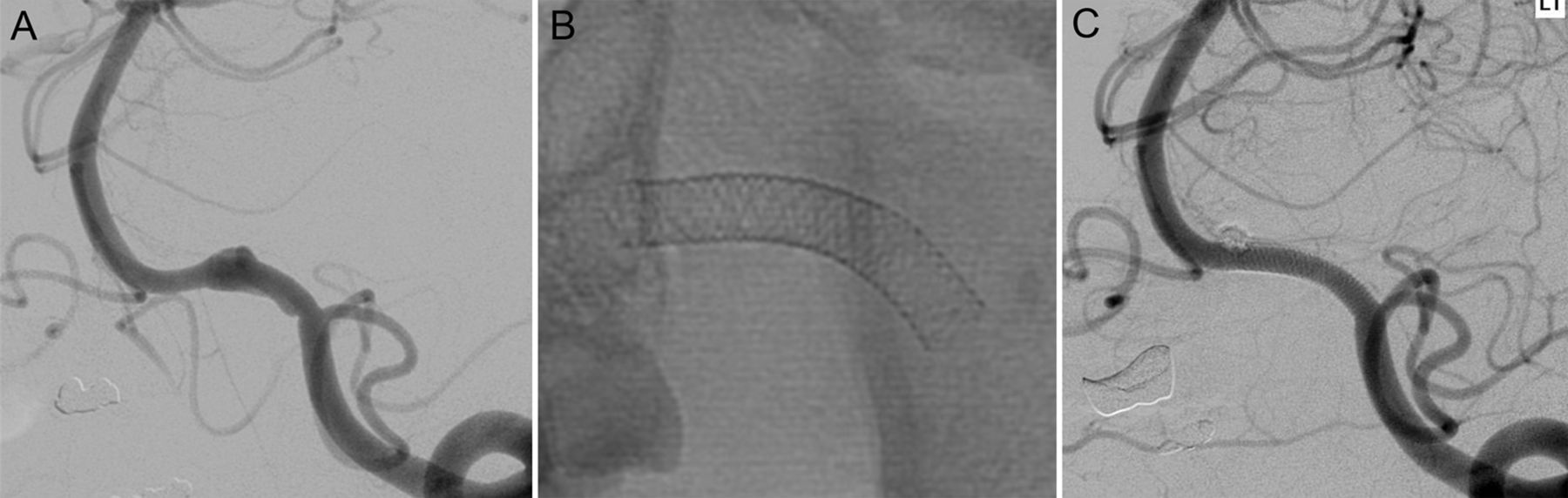
(A) Left vertebral artery angiography shows a ruptured V4 segment aneurysm. (B) Two Pipeline embolization devices measuring 3×16 mm and 3.25×16 mm were placed across the dissected segment in a telescoping fashion. (C) Follow-up angiography 27 months after treatment shows complete remodeling of the injured segment and no evidence of aneurysm recurrence. Used with permission from Barrow Neurological Institute.
Patient 4
This patient was found on follow-up angiography to have a recurrent basilar apex aneurysm 20 years after suffering a SAH and undergoing clip ligation (figure 2A). A single PED spanning the left P1 down to the basilar trunk was deployed (figure 2B) followed by coiling of the aneurysm through a jailed microcatheter. Thrombosis of a branch of the left SCA was noted following coiling (figure 2C) and treated with an intravenous loading dose of abciximab. The patient awoke in a normal neurological condition. Follow-up angiography 27 months after treatment showed no evidence of recurrent aneurysm (figure 2D) and patency of the thrombosed branch.
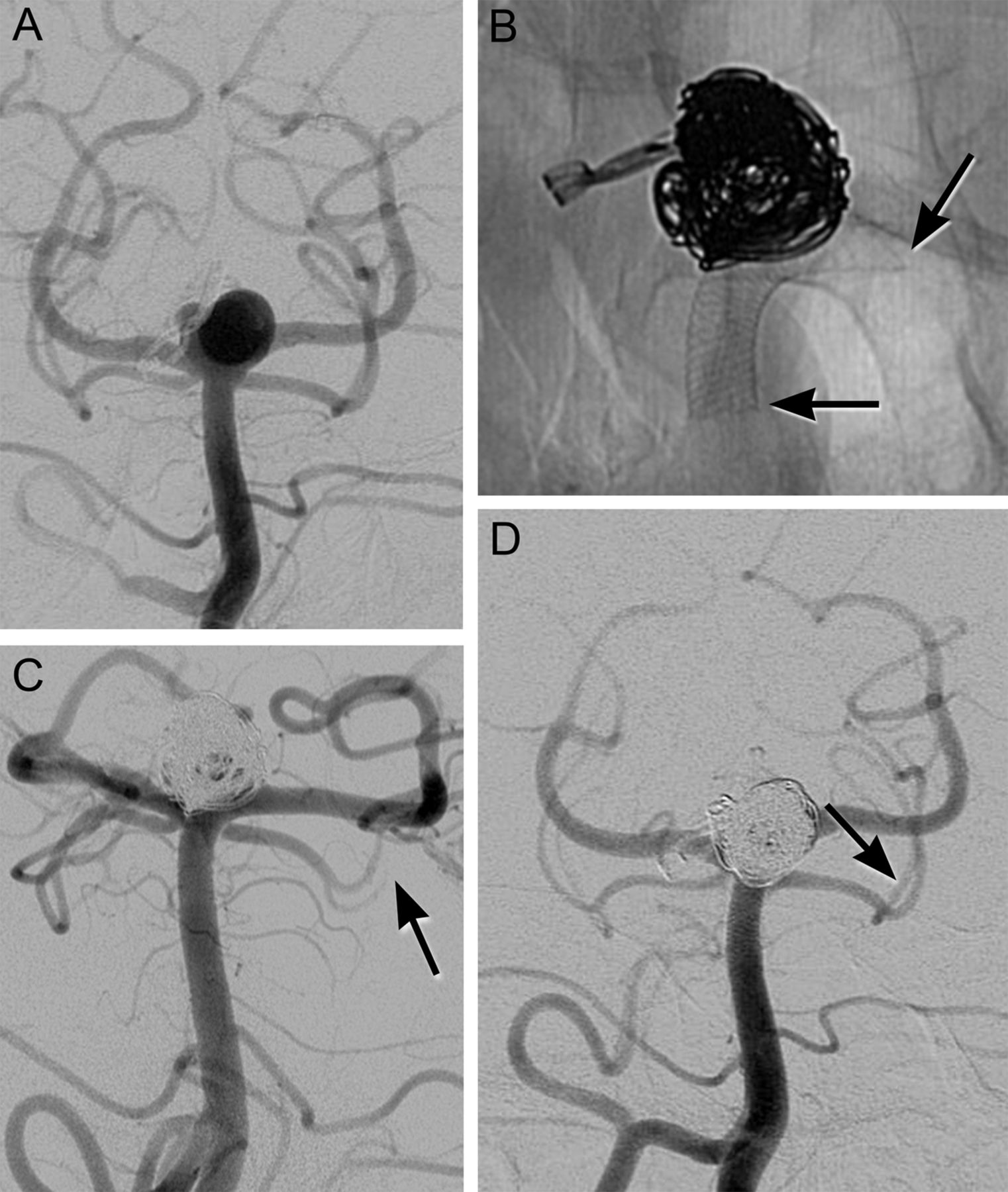
(A) Left vertebral artery angiography shows a recurrent basilar apex aneurysm 20 years after clip ligation for subarachnoid hemorrhage. (B) A single 3.5×20 mm Pipeline embolization device (arrows) was used to cover the neck spanning the left P1 to the basilar trunk. The aneurysm was then coiled through a jailed catheter. (C) Immediately after treatment, thrombosis (arrow) of a distal branch of the left superior cerebellar artery (SCA) was noted and treated with an intravenous loading dose of abciximab. The patient awoke in a normal neurological condition. (D) Follow-up angiography 27 months after treatment shows no evidence of aneurysm recurrence and reopening of the SCA branch (arrow). Used with permission from Barrow Neurological Institute.
Patient 10
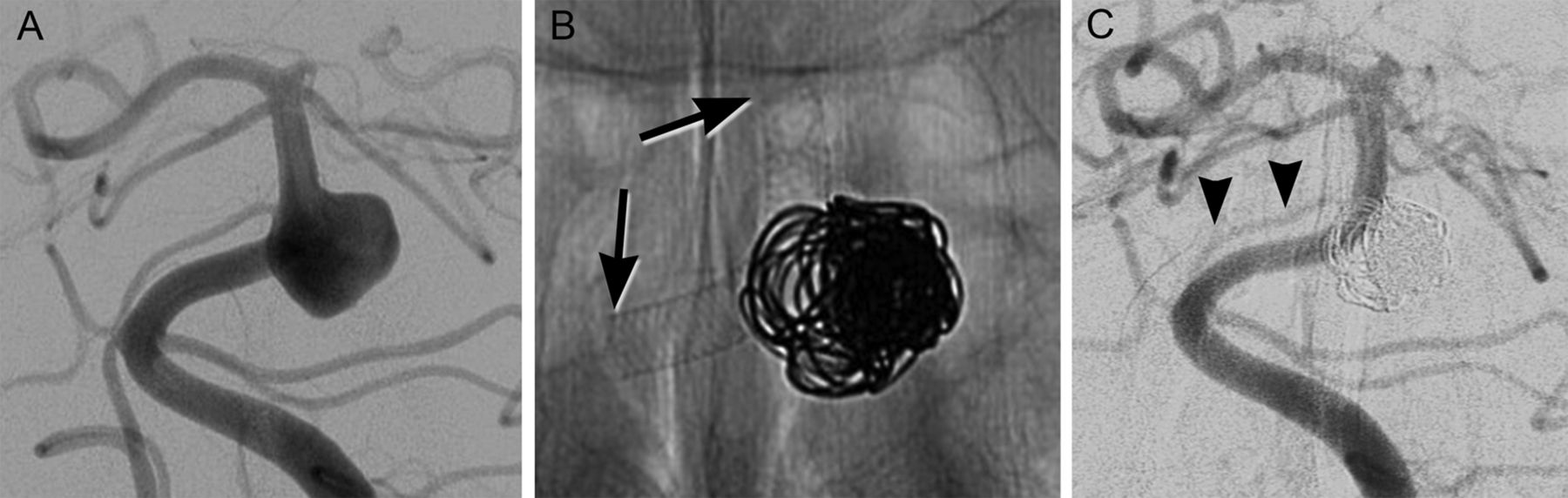
This patient was found to have a large basilar trunk aneurysm during investigation for headaches (figure 3A). The patient underwent PED-supported coil embolization of the aneurysm through a jailed microcatheter (figure 3B). Thirteen months after treatment the patient remains neurologically normal with no evidence of recurrent aneurysm (figure 3C).

{kind=link}
{kind=link}
{kind=link}
(A) Left vertebral artery angiography demonstrates a large basilar trunk aneurysm in a patient with headaches. (B) A single 3.5×20 mm Pipeline embolization device (arrows) was placed across the neck of the aneurysm, which was subsequently coiled through a jailed catheter. (C) Follow-up angiography 13 months after treatment shows no residual aneurysm and patency (arrowheads) of the covered right anterior inferior cerebellar artery (C). Used with permission from Barrow Neurological Institute.
Discussion
A number of factors characteristic of the posterior circulation may produce a higher rate of treatment-related complications. The large number of perforating arteries originating along the basilar trunk and apex, complex aneurysm anatomy, and aneurysm location all influence this risk profile. The current literature evaluating the use of flow diverters in this aneurysm subgroup purports a higher complication rate than that associated with anterior circulation aneurysms.
In their review of seven patients with large or giant fusiform vertebrobasilar aneurysms, Siddiqui et al2 reported poor outcomes (including four deaths) in five patients. A critical evaluation of these cases reveals that the majority were dolichoectatic aneurysms involving long segments of the basilar artery. Multiple devices were placed in all cases with an average of 4.8 per patient.2 All but one patient presented with neurological deficits. Poor outcomes were the result of aneurysm rupture or brainstem infarction.2
These results cannot be applied to the entire cohort of patients with posterior circulation aneurysms. Dolichoectatic aneurysms of the basilar artery carry a dismal prognosis with a mortality rate approaching 35% at 5 years.2 ,5 The sheer length of these lesions requires the deployment of multiple devices, as the authors describe in their study, with long segments that remain unopposed to the construct.2 Compromise of perforating arteries, the requirement for multiple devices, the frequent coexistence of thrombus within the aneurysm fundus, and the presence of neurological instability secondary to mass effect or prior brainstem infarction further compound the potential for poor outcomes.
In a prospective case registry conducted at three Australian neurointerventional centers, Phillips et al3 reported 32 patients with posterior circulation aneurysms treated with the PED. Three permanent complications (3/32, 9.4%) occurred in this cohort and all involved perforator infarctions in patients with basilar aneurysms. Interestingly, all three infarctions occurred after the placement of a single PED, suggesting that coverage of a perforating artery ostium is not the only etiology of stroke in this subset of patients. An additional two patients had asymptomatic intracranial hemorrhages.3
These results led the authors to conclude that “a higher clinical perforator infarction rate may be associated with basilar artery PEDs relative to the internal carotid artery”, and that PEDs should only be used when more conventional endovascular or surgical techniques are not feasible.3
Perforator infarctions probably occur for three distinct reasons.6 In the acute setting, coverage over a perforating artery ostium by one or more tynes of the device may either sufficiently narrow or occlude the artery. Alternatively, acute thrombus within the device may migrate distally through a perforating artery. In the subacute or chronic setting, delayed infarctions may occur as a result of neointimal proliferation over the perforator ostia.
In an analysis of 12 patients with basilar aneurysms treated with the Silk device (Balt, Montmorency, France), Kulcsar et al6 specifically assessed branch vessel and perforator patency after flow diverter placement. Of the 22 branch vessels that were bridged by the Silk device, only one posterior cerebral artery (PCA) occluded at the time of treatment. This was managed with intra-arterial tirofiban administration and produced no neurological sequelae.
Nonetheless, four other complications occurred in this series, including one case of thrombosis through the construct 12 h after treatment. This patient presented in poor neurological condition (modified Rankin Scale score (mRS) of 4) and required the placement of an additional Enterprise stent (Codman, Raynham, Massachusetts, USA) for complete coverage of the aneurysm neck. The patient worsened as a result of treatment to an mRS score of 5.
Three patients presented with delayed ischemic insults, including two thalamic infarcts at 7 months and 4 weeks after treatment and one pontine infarct 5 weeks after treatment. This suggests that neointimal hyperplasia may progressively narrow or occlude perforating arteries. The authors astutely recognized that perforator patency is virtually impossible to ascertain during treatment, given that angiography often fails to opacify these small vessels. The potential of neointimal proliferation underscores the need for diligent antiplatelet therapy and patient compliance.
While they do not specifically mention the morphology of the aneurysms treated (ie, dolichoectatic or saccular), they state that the majority of patients were symptomatic, previously treated endovascularly, or deemed to be at high risk of aneurysm rupture. Certainly, this higher risk cohort would be expected to develop acute or subacute complications more frequently.
In their series of 251 aneurysms treated with the PED (19 of which involved the posterior circulation), Saatci et al7 described a single patient who developed thrombosis of the right PCA after jailing it with a PED extending from the left PCA to the basilar trunk. The patient sustained a brainstem infarction and subsequently died. The authors did not specifically state whether any complications other than the PCA thrombosis occurred in this subset of patients. We are unsure why major posterior circulation branches would be more prone to thrombosis after PED jailing than branches of the internal carotid artery. Such complications are more likely to be related to issues with antiplatelet therapy, aneurysm selection, or device problems such as vessel dissection or PED malposition.
Aneurysm morphology and presentation are critical factors to consider when selecting posterior circulation aneurysms for treatment with the PED. In their report of seven patients with posterior circulation aneurysms, Chalouhi et al8 treated only one fusiform aneurysm that exerted brainstem compression. This patient failed to improve clinically and demonstrated no change in the morphology of the aneurysm after treatment. No major complications occurred in this series. The authors argue that perhaps ‘symptomatic’ fusiform aneurysms, specifically those compressing the brainstem, should not be treated with flow diversion due to the frequent need for multiple telescoping devices. This factor may add to procedural morbidity.8
Within their series of 31 patients with posterior circulation fusiform aneurysms, Raphaeli et al treated four with flow diversion (Silk).9 Two complications occurred in this cohort including one death and one case of delayed transient hemiparesis. The patient who died had symptoms of brainstem compression secondary to a giant, partially thrombosed vertebral artery aneurysm which was treated with a single flow diverter. This case, as well as those of Chalouhi et al, suggests that aneurysm enlargement from further thrombosis compounds brainstem compression producing either devastating neurological sequelae or death. The argument against the use of this technology in the setting of such clinical instability is clear.
Basilar artery thrombosis, both acutely and in a delayed fashion, is another source of complications in this patient subset. Acute thrombosis is probably produced through a number of mechanisms including lack of response to antiplatelet medication, malposition or lack of apposition of the stent, or arterial injury at the time of PED deployment. Careful assessment of appropriate response and compliance with the antiplatelet regimen as well as the exclusion of unfavorable (dolichoectatic or circumferential) aneurysms will lessen the likelihood of this life-threatening complication.
More troubling are reports of delayed thrombosis. Klisch et al10 described two patients with fusiform basilar trunk aneurysms who developed thrombosis after clopidogrel was stopped when follow-up angiography at 1 year demonstrated slight residual filling of both aneurysms. The authors postulate that flow diverters remain more thrombogenic and undergo neoendothelialization more slowly when the devices are within the thrombosed portion of these fusiform aneurysms. When encountering residual filling in this situation, the authors argue that placing additional devices through the construct is preferable to altering the antiplatelet regimen.10
Fiorella et al11 reported a patient with a V4 aneurysm who developed thrombosis 23 months after treatment with PED-supported coil embolization. The authors suggest that ‘over-exuberant neointimal hyperplasia’ occurred within the construct as a result of an aggressive biological response to the polyglycolic acid-impregnated coils.11 This patient's antiplatelet regimen had also been modified in the months preceding his demise.
These reports underscore our lack of understanding of the need and duration of antiplatelet therapy, as well as uncertainty regarding the interaction of these devices with coils and other endovascular hardware.10 ,11 Furthermore, these cases involved circumferential aneurysms, a subgroup that is not included in our present analysis and that is not optimally treated with flow diversion.10 ,11
Other complications have been described in patients with posterior circulation aneurysms treated with the PED. Colby et al12 reported a sixth cranial neuropathy in a patient with a giant vertebrobasilar aneurysm. Fischer et al13 reported a ‘severe’ cerebellar hemorrhage after treatment of a fusiform basilar trunk aneurysm. Like the complications discussed above, these complications occurred in patients whose aneurysms were not ideally suited for treatment with this device.12 ,13
Distal wire tip fracture occurred in a case reported by Briganti et al.14 Following removal of the fractured wire, the patient developed thrombosis of the SCA requiring emergency thrombolysis. Fortunately, the patient eventually made a complete recovery.14 In our case, the distal wire tip was retained in a small perforator arising from the right PCA. We did not retrieve the fractured portion. The patient awoke normally and did not manifest any late clinical sequelae.
Our series demonstrates that, with proper patient and aneurysm selection, the PED can be used safely and effectively. We encountered five complications after use of this device in this setting, only one of which was permanent. Including the distal wire tip fracture, the other transient complications involved a clinically silent SCA thrombosis, small CVA, and a urethral tear from traumatic Foley catheter placement. Our single permanent complication was an intracerebral hemorrhage after external ventricular drain replacement. This event left the patient disabled and was probably exacerbated by antiplatelet therapy. Other than improper aneurysm selection, these complications represent the main categories accounting for patient morbidity: issues pertaining to antiplatelet therapy, perforating or branch vessel thrombosis, and non-PED-related procedural difficulties.
The utility of this device has been demonstrated in the management of V4 aneurysms, a large proportion of which are dissecting and prone to re-rupture.4 Eight V4 aneurysms were treated in our series. Of the seven patients undergoing angiographic follow-up, five had complete aneurysm occlusion and two had near-complete occlusion.
Dissecting aneurysms proximal to the V4 segment and distal along the course of the basilar artery are also amenable to PED treatment. De Barros Faria et al reported the use of the PED for the treatment of 21 dissecting aneurysms of the posterior circulation involving the V4 segment, vertebrobasilar junction, basilar trunk, and the posterior inferior cerebellar artery. The utility and safety of this device for this particular subset of dangerous aneurysms represents an important therapeutic advance.15 Despite the added potential morbidity associated with antiplatelet therapy, use of the PED in the setting of SAH secondary to a posterior circulation dissecting aneurysm should be considered when other conventional endovascular and microsurgical treatment options are either not possible or fail.
Conclusion
The PED can be used safely and effectively in the treatment of specific posterior circulation aneurysms. Patients with saccular or dissecting aneurysms were managed with a safety profile comparable to that associated with the anterior circulation. We avoided treating patients with dolichoectatic or fusiform aneurysms, as well as patients with neurological instability from brainstem compression. Importantly, this device is effective in treating V4 aneurysms, a subgroup often associated with re-rupture (prior to treatment) and poor patient outcomes. Nonetheless, potential sources of complications pertain largely to antiplatelet therapy and vessel thrombosis. With careful patient selection, these risks can be mitigated and should prove no more commonplace than complications occurring in the anterior circulation.
References
Footnotes
Contributors All authors made substantial contributions to the conception or design of the work; the acquisition, analysis, or interpretation of data for the work; drafted the work or revised it critically for important intellectual content; and provided final approval of the version to be published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None.
Ethics approval Ethics approval was obtained from the Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.