Article Text

Abstract
Background Experience with the endovascular treatment of cerebral aneurysms by flow diverter devices (FDDs) is limited to four devices (Pipeline, Covidien; FRED, Microvention; Silk, Balt Extrusion; Surpass, Stryker), as reported in different studies.
Objective To describe the initial experience and the technical innovations of a new-generation FDD (p64 Flow Modulation Device, Phenox, Bochum, Germany).
Methods Between December 2014 and February 2015, six intracranial aneurysms in five patients (four women, one man; mean age 63 years) were treated with the p64 Flow Modulation Device.
Results Immediate post-treatment angiography showed reduced flow into all aneurysms. No long-term angiographic data are available. The device may be easily deployed and totally retrieved with a unique mechanical detachment. No periprocedural technical complications occurred. No early or delayed aneurysm rupture, no ischemic or hemorrhagic complications, and no neurological morbidity or death were seen.
Conclusions Treatment of cerebral aneurysms with the p64 Flow Modulation Device is a safe procedure with no technical complications. The mechanical detachment and the 100% retrievability are significant advantages of this new device. However, large prospective studies with long-term clinical and angiographic follow-up are necessary to assess the role of the p64 in the endovascular treatment of intracranial aneurysms.
- Aneurysm
- Flow Diverter
- Device
- Intervention
Statistics from Altmetric.com
Introduction
Experience with flow diverter devices (FDDs) has emerged in the past 7 years as a new paradigm in the endovascular treatment of cerebral aneurysms. They are rapidly becoming a suitable and, in selected cases, preferred alternative to traditional endosaccular treatment with coils.
These new devices comprise a high-attenuation braided mesh stent placed in the parent artery at the level of neck which disrupts the intra-aneurysmal flow and subsequently creates intra-aneurysmal thrombosis; the exposed surface of the FDD is also a good support for the development of the neointima.1 ,2
Since the approval of the Pipeline embolization device (Covidien, Mansfield, Massachusetts, USA) and the Silk (Balt Extrusion, Montmorency, France) different studies have confirmed the efficacy of this technique, with a high rate of occlusion and acceptable morbidity and mortality.3–11 On the other hand, the experience with new FDDs, such as FRED (Microvention, Tustin, California, USA),12 ,13 Surpass (Stryker Neurovascular, Fremont, California, USA)14 ,15 and Pipeline Flex (Covidien)16 is still limited.
This study aimed at describing the initial experience and the technical innovation of a new-generation FDD (p64 Flow Modulation Device, Phenox, Bochum, Germany). No studies reporting endovascular aneurysm treatment with this device have yet been published.
p64 Flow Modulation Device
The p64 Flow Modulation Device device is a braided mesh tube, composed of a 64 nickel–titanium alloy (nitinol) with radiopaque markers along the length of the device and eight proximal bundle markers. The device is compatible with a 0.027 ‘ID microcatheter’. It is available in sizes 2.5–5 mm diameter with 12–36 mm length (depending on diameter size). It received the CE mark of approval in the 2012. The usual insertion technique, common to the other FDDs, involves deploying the distal tip of a delivery microcatheter (XT27, Stryker, Freemont, California,USA; Marksman, Covidien, Mansfield) beyond the aneurysm neck and then pushing the p64 to the tip of the delivery wire to which it is attached. The system is then aligned with the aneurysm under fluoroscopy and the p64 is deployed by withdrawal of the microcatheter. This requires a combination of pushing the delivery wire and retrieving the microcatheter, to allow the p64 to expand and to compensate for any resulting foreshortening. During the device deployment, the distal wire tip must be able to advance distally, the device should be fully expanded along the entire implant length, and the proximal end (detachment zone) should not be located in a narrow curve. The option of retrieving the device after complete deployment is a clear advantage; owing to a controlled mechanical detachment, the p64 can be retrieved into the microcatheter and removed or repositioned until its complete length has been extruded. Once a satisfactory position is reached, the device is detached.
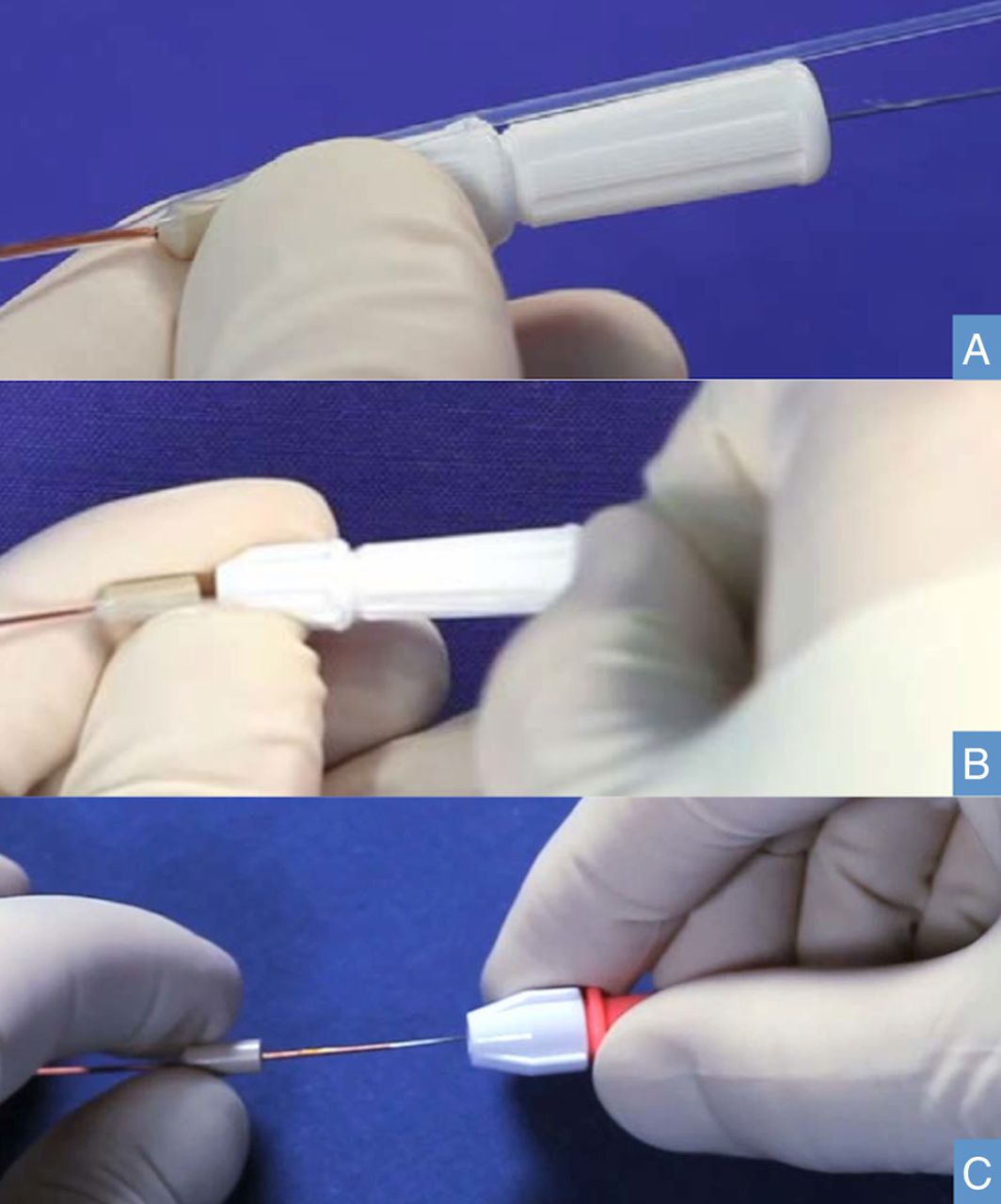
The mechanical detachment may be synthesized in four steps. First, it is necessary to remove the peel-away sheath, tearing it off parallel to the handle and torquer (figure 1A, B). The second step is to loosen the white torquer at the proximal end of the delivery wire and remove it. The third step is the placement of another standard torquer about 1 cm proximally to the end of the detachment tubing and tightening it to the delivery wire (figure 1C). The last step is pulling the proximal end of the polymer tube towards the torquer, while holding the delivery wire in a fixed position.

Mechanical detachment. (A and B) Peel-away sheath removal; (C) after loosening the white torquer, another torquer is placed proximally to the end of the detachment tubing and tightened to the delivery wire; detachment is by pulling the proximal end of the polymer tube toward the torquer.
Materials and methods
Study design
This study was designed to define the role of endovascular management with a new FDD (p64 Flow Modulation Device, Phenox, Bochum, Germany) in the treatment of intracranial aneurysms.
Six aneurysms in five patients were treated between December 2014 and February 2015 with the p64 FDD. Four patients had single aneurysms. In one patient with three aneurysms, only two were treated (one small aneurysm of the middle cerebral artery (MCA) was left intact).
Inclusion criteria were patient consent to the endovascular procedure and aneurysms difficult to treat by both coiling and clipping because of their anatomical configurations (wide neck, fusiform, posterior circulation).
Radiological definition was obtained in all cases by CT angiography, with native images and two-dimensional multiplanar reconstructions, and by digital subtraction angiography (DSA).
The aneurysm location, size, neck, dome to neck ratio, and proximal and distal diameter of the parent vessel were considered. The size and length of the device was chosen according to the proximal diameter of the parent artery, as is usual for this technique; the device was oversized in one case to reduce the risk of occlusion of the perforator.
The end points were an assessment of periprocedural technical complications and early morbidity and mortality.
Patient and treatment characteristics
Five patients (four women, one man, ranging in age from 47 to 76 years (mean age 63 years) were included in the study (table 1).
Patient, aneurysm, and device characteristics
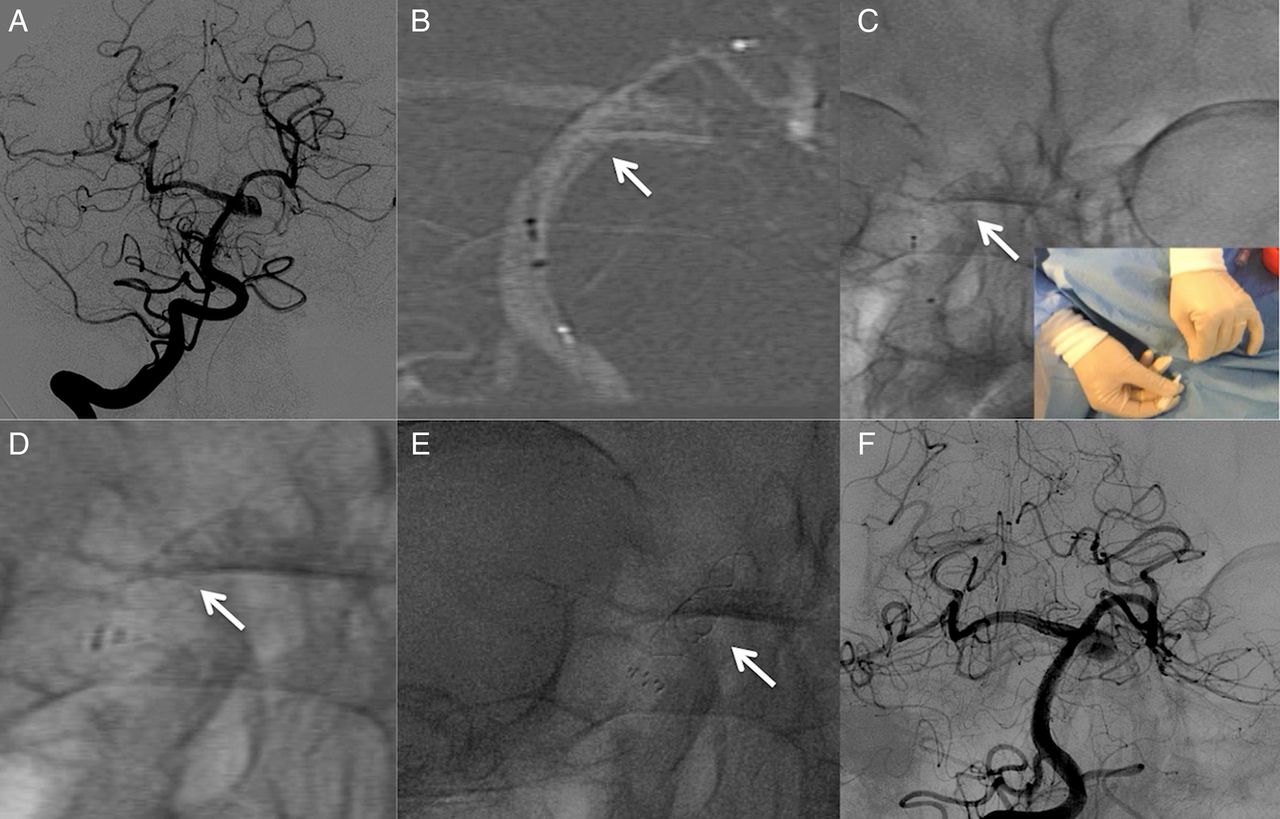
Four patients had unruptured aneurysms and one was treated in the subacute phase (10 days after) of subarachnoid hemorrhage (SAH) (figure 2).
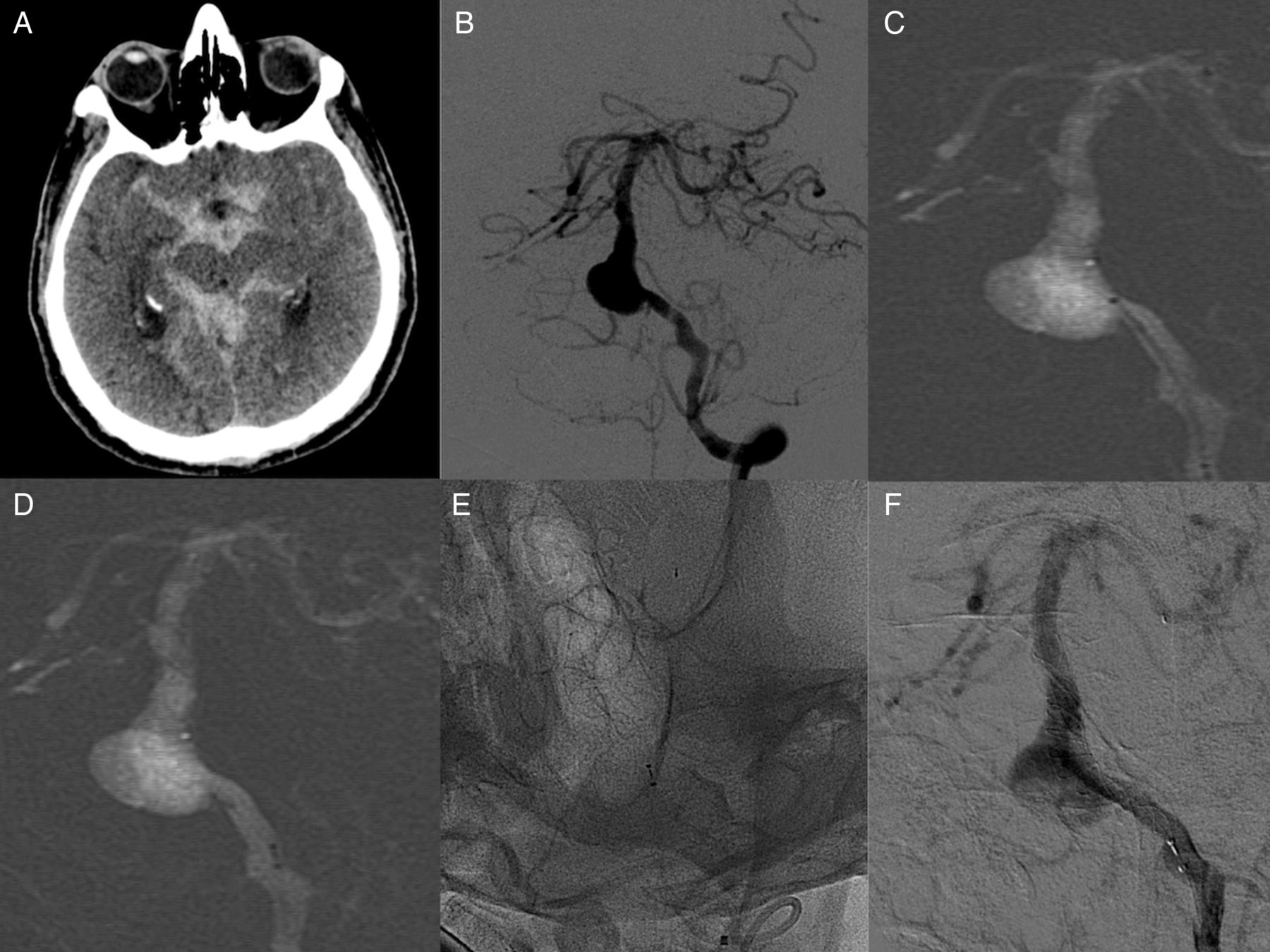
(A) CT scan of a 76-year-old man presenting with subarachnoid hemorrhage. (B) Digital subtraction angiography shows a large fusiform aneurysm of the basilar artery (vertebrobasilar junction): the right anterior inferior cerebellar artery arose from the sac; the right vertebral artery was hypoplastic, ending in the right posterior-inferior cerebellar artery (not shown). (C and D) Endovascular treatment, roadmapping images: p64 deployment. (E) Non-subtracted image of the deployed device. (F) Subtracted image at the end of the procedure shows immediate contrast stasis in the sac.
The FDD was the only treatment in four patients; endosaccular coils were also implanted in one case (figure 3). No previous endovascular or surgical treatments were performed.

A 58-year-old woman harboring a large fenestration basilar artery aneurysm with compression on the brainstem: left (A) and right (B) vertebral artery angiograms. (C) p64 Deployment: from the left vertebral artery to the basilar trunk. (D) Early angiogram after the p64 deployment: immediate contrast stasis in the sac. (E and F) Worms–Bretton and laterolateral projections after coiling of the sac (left vertebral artery injection). (G) Right vertebral artery angiogram at the end of the procedure. (H) Non-subtracted image shows fully opened p64 and coils.
In the patient with multiple aneurysms—that is, in the posterior communicating artery (PComA), internal carotid artery (ICA) bifurcation and M1 segment MCA, the first two were treated by a single device (figure 4).
(A) A 68-year-old woman harboring multiple small aneurysms on the right side (PComA, ICA bifurcation, M1 middle cerebral artery). (B) Endovascular treatment of the PComA and ICA bifurcation aneurysms by a single p64. (C and D) Non-subtracted and subtracted images show immediate contrast stasis in both aneurysm sacs. ICA, internal carotid artery; PComA, posterior communicating artery.
Aneurysm characteristics
Of the six treated aneurysms, three were located at the basilar artery (BA), one at the anterior communicating artery (ACoA), one at the PComA and one at the ICA bifurcation; the untreated aneurysm was at the MCA. All were saccular, except for one which was fusiform. The aneurysm size ranged from 3 to 15 mm (median diameter 9 mm).
The neck size ranged from 2 to 8 mm (mean 4.5 mm). The dome to neck ratio ranged from 0.4 to 1 (mean 0.6) (table 1).
Endovascular treatment and medication
Four patients were pretreated with 75 mg daily of clopidogrel for 5 days, together with 150 mg of aspirin. The patient treated in the subacute phase of SAH, received a loading dose of clopidogrel (600 mg) 4 h before the procedure.
Preoperative platelet function monitoring with a VerifyNow assay was performed in four of the five patients, but not in the patient treated in the subacute phase of SAH. No resistance to clopidogrel was seen.
All patients received continuous intravenous infusion of heparin during the procedure, and a bolus of 1000 IU/h during the procedure, to maintain an activated clotting time >250–300 s.
Corticosteroids were administered only in two patients with large aneurysms of the posterior circulation (16 mg of dexamethasone during the procedure and 16 mg/daily in the first week).
The procedure was performed under general anesthesia through catheterism of the right common femoral artery by using an 8F vascular sheath and a triaxial system (Neuronmax Penumbra, LIR 5.5 Phenox, XT27 Stryker). The p64 was then placed at the level of the aneurysm. The correct apposition to vessel wall was assessed with DSA and non-subtracted angiographic images. The procedure was considered successful if the p64 completely covered the aneurysm (0.5–1 cm proximal and distal to the aneurysm neck).
Intra-aneurysmal contrast stasis was seen in all aneurysms immediately at the end of the procedure.
All patients underwent clinical examination and CT immediately after the procedure to exclude hemorrhage or brain ischemia.
Results
No intraprocedural and periprocedural technical complications occurred (table 2).
Treatment characteristics
The device was retrieved and repositioned in three patients, with BA, ACoA, and PComA/ICA aneurysms, respectively.
Immediate post-procedural angiography demonstrated reduced flow into all aneurysms. No long-term angiographic data are yet available.
The patient harboring a fusiform BA aneurysm, treated in the subacute phase of SAH showed clinical and radiological improvement and was discharged with no disability (modified Rankin Scale (mRS) 0).
In the patient with a large aneurysm at the BA fenestration, treated with p64 and coils, MR showed decreased compression and edema of the brainstem. The preprocedural disability score was unchanged (left hemiparesis, mRS 3).
No neurological morbidity was seen immediately after the procedure and at discharge in the other three patients.
The five patients were clinically examined on 16 February 2015. The follow-up ranges from 15 to 60 days. Clinical conditions were stable with mRS 0 in four patients and unchanged mRS 3 in one.
No early or delayed aneurysm rupture, no subarachnoid or intraparenchymal hemorrhage, and no deaths occurred in the follow-up period.
Discussion
Endovascular occlusion with coils is the more widely used endovascular treatment for both ruptured and unruptured intracranial aneurysms.17 ,18 Technical advantages include the possibility of deploying, retrieving, and repositioning the coils until the correct position is obtained, and the possibility of good radiological control before the detachment, owing to their excellent radio-opacity.
The possibility of treating uncoilable aneurysms (fusiform, wide-neck, large, giant, and bifurcation) with no risk of recanalization makes flow diversion a unique endovascular technique.
However, technical procedural problems are not uncommon for flow diversion and it is more difficult to visualize FDDs under fluoroscopy. Additionally, first-generation devices were not completely retrievable; thus, obtaining the correct position at the start was very important to avoid mispositioning and failure of the procedure. Furthermore, the relatively new experience with these devices and the long learning curve explained the high percentage of periprocedural technical complications in the first series.7 ,9 ,19 ,20
Other technical problems include the radial force, the risk of shortening, and the difficulty of choosing the length and size of the device.
Our initial experience has shown that the p64 has undoubted benefits over other FDDs (table 3). These include the good radial force, the 100% retrievability, and the mechanical detachment.
Technical aspects of flow diverter devices
In our small series, we could deploy the device as intended in all cases; the flexibility of the system was good and its visibility allowed controlled manipulation. No adverse events related to the device occurred. Thus p64 is equivalent to, or better than, other known FDDs (Pipeline Flex, Silk, FRED, Surpass), which have similar functions but only partial retrievability (50–80%).
In our series the treatment was chosen because both coiling and clipping were difficult. We preferred the p64 system rather than other FDDs, because of the possibility of retrieving and mechanically detaching the device. In three patients, where the initial position of the device was unsatisfactory it was possible to retrieve the fully opened device and redeploy it in the correct position.
The choice of device size was based on several factors—mainly, the vessel diameter proximal to the aneurysm neck; the proximal diameter is usually larger than the distal diameter. The device was oversized in one case for different reasons. The use of a device with 64 braiding wires, instead of 48, with major metal coverage (defined as the ratio of the metal surface area to the total surface), and major pore density (defined as the number of pores per unit surface area) may lead to a higher rate of aneurysm occlusion; however, it might also lead to stenosis or occlusion of side branches or perforators once covered with dense metal mesh.21 The patency of perforators must be considered while increasing the pore density of the device. Reduction of the pore size below orders of cellular lengths may allow neointimal cells to bridge the gap between device struts and completely cover the perforator ostia.22 The correlation of aneurysm occlusion with the metal coverage cannot be confirmed in ‘in vivo’ human studies; however, occlusion of side branches and perforators has been reported in different series.4 ,23 ,24 ,25 Additionally, when FDD porosity increases (as in oversized devices), metal coverage decreases.26 Although no clear evidence exists, we preferred to oversize the device in the posterior circulation to reduce the risk of occlusion of perforators and side branches.
The choice of oversizing is also related to the ‘short landing zone’; in oversized FDDs the landing zone of insufficient length may lead to device deformation with minimal or moderate terminal stenosis.27
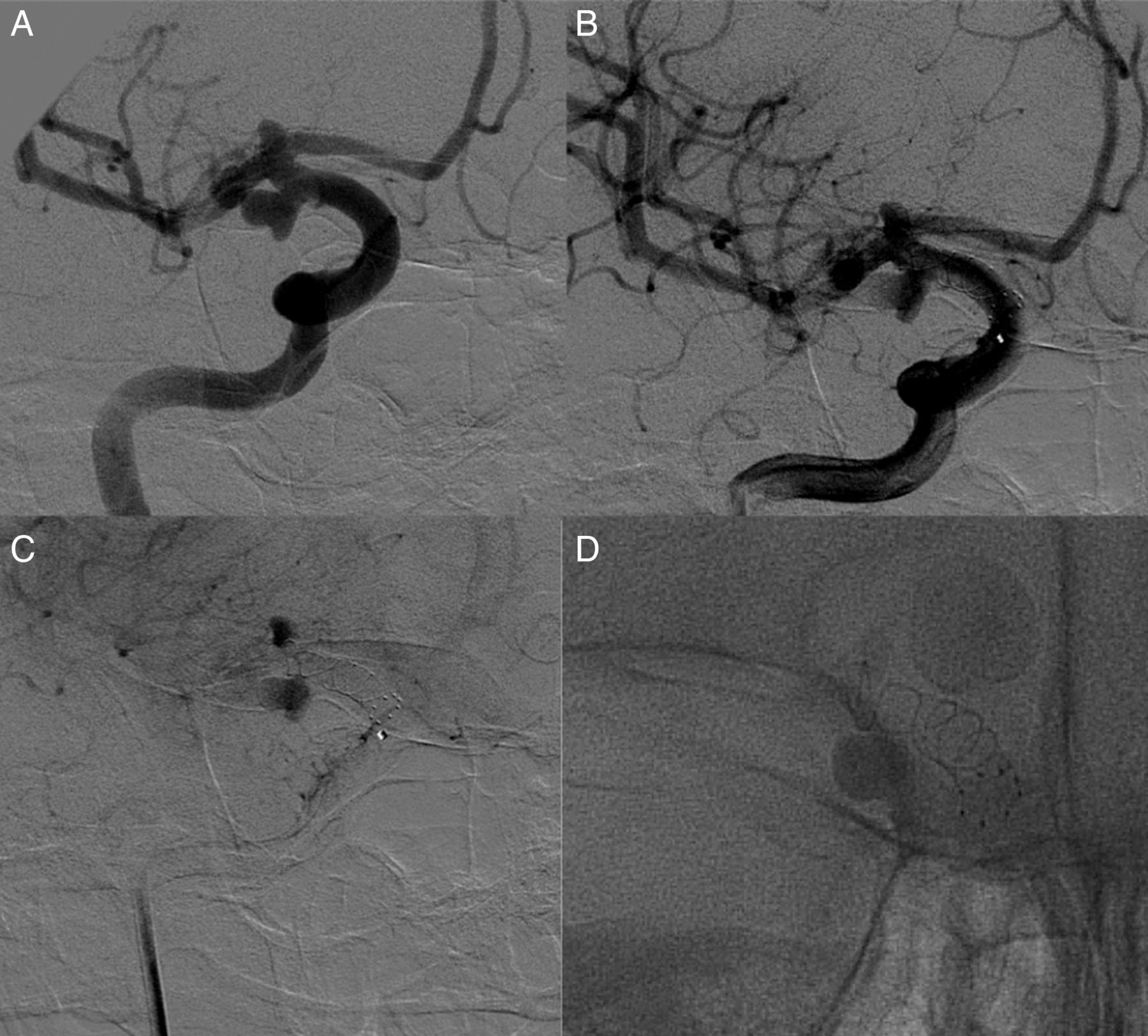
In one case we used an oversized p64 (size 3.5×15 mm) in a vessel of smaller proximal diameter (3 mm), where the first apposition did not completely cover the aneurysm because of the ‘memory shape’ of the device. The advantage of using a 100% retrievable device is that it permits recovery and repositioning of the p64 (figures 5 and 6).
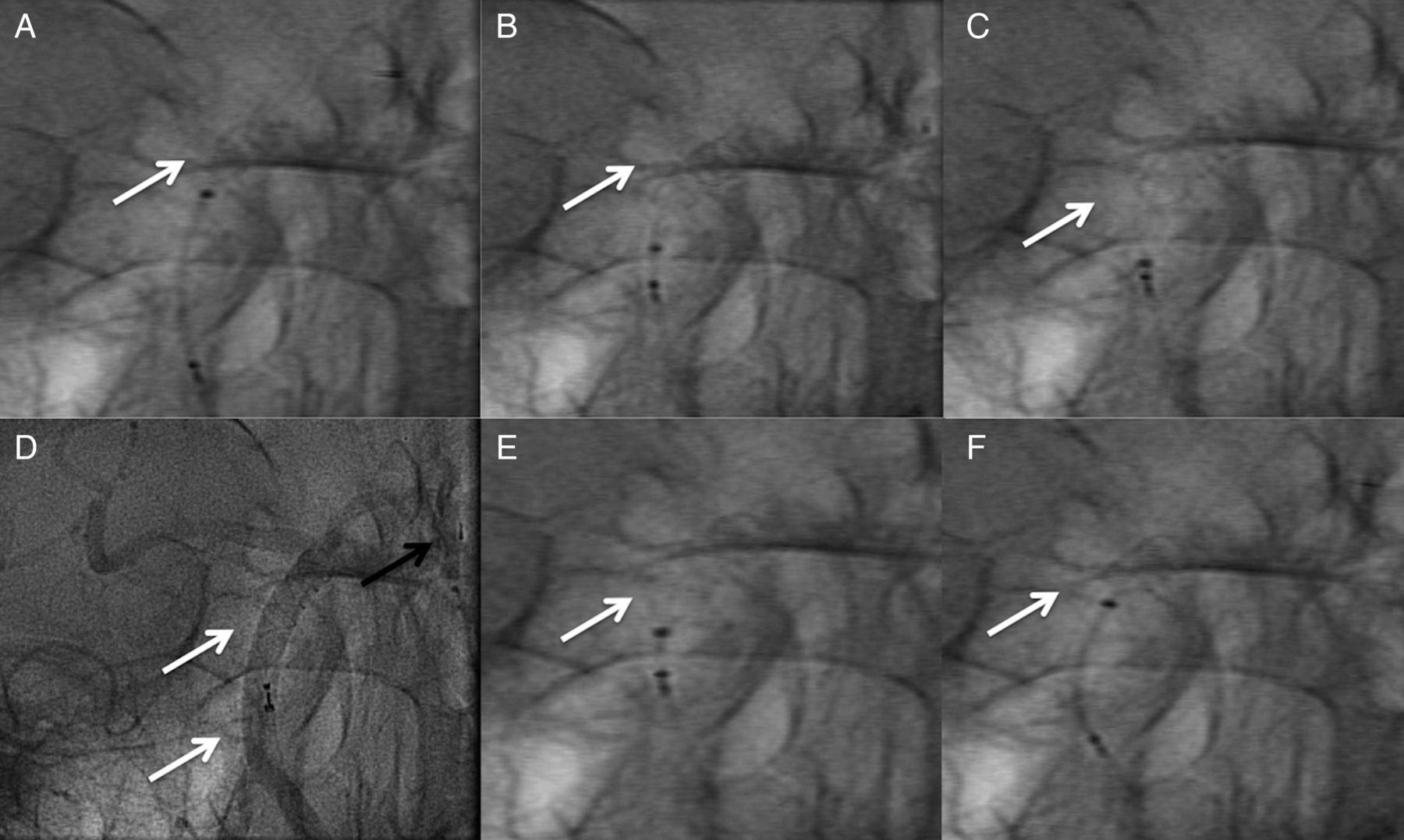
(A–C) Fluoroscopy images: device deployment. (D) Non-subtracted images after deployment: device mispositioning. Black arrow shows the distal delivery wire and its marker. (E and F) Fluoroscopic images: device recovery.

(A) A 47-year-old woman harboring a saccular laterobasilar aneurysm, upper to left superior cerebellar artery origin. (B) Roadmapping images: device deployment. (C) Fluoroscopic images: mechanical detachment of the device. (D and E) Fluoroscopic and non-subtracted images of the deployed device. (F) Angiogram after the deployment: immediate contrast stasis in the sac.
Of three patients with posterior circulation aneurysms, one was treated in the subacute phase of SAH and another had left hemiparesis from brainstem compression. Aneurysms in this location have less unfavorable outcome and higher complication rate, morbidity, and mortality after endovascular and surgical procedures, than those of the anterior circulation. Toth et al28 reported, 12.3% mortality and 11% permanent neurologic morbidity for aneurysms of the posterior circulation treated with FDDs. In our three patients, treated with p64, no early morbidity and mortality were seen.
The use of an FDD has been reported recently, mainly to treat ICA aneurysms proximal to the circle of Willis.3–11 Experience beyond the circle of Willis is still limited24 ,29 ,30 and effectiveness is controversial owing to the lack of small-sized (<3 mm) devices. On the other hand, a small-size p64 device (2.5 mm) enables the treatment of aneurysms in smaller arteries while maintaining patency of the parent vessel.
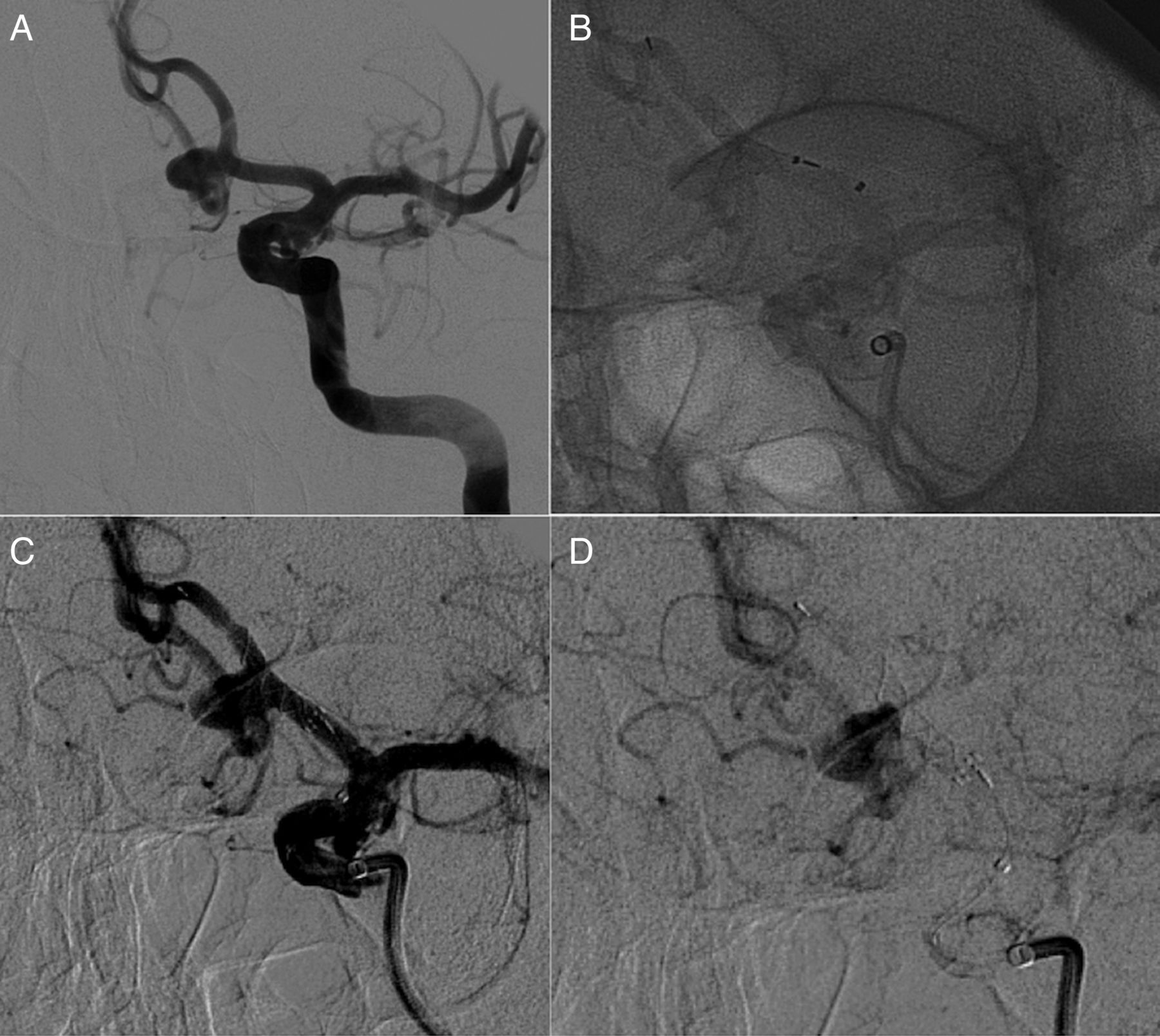
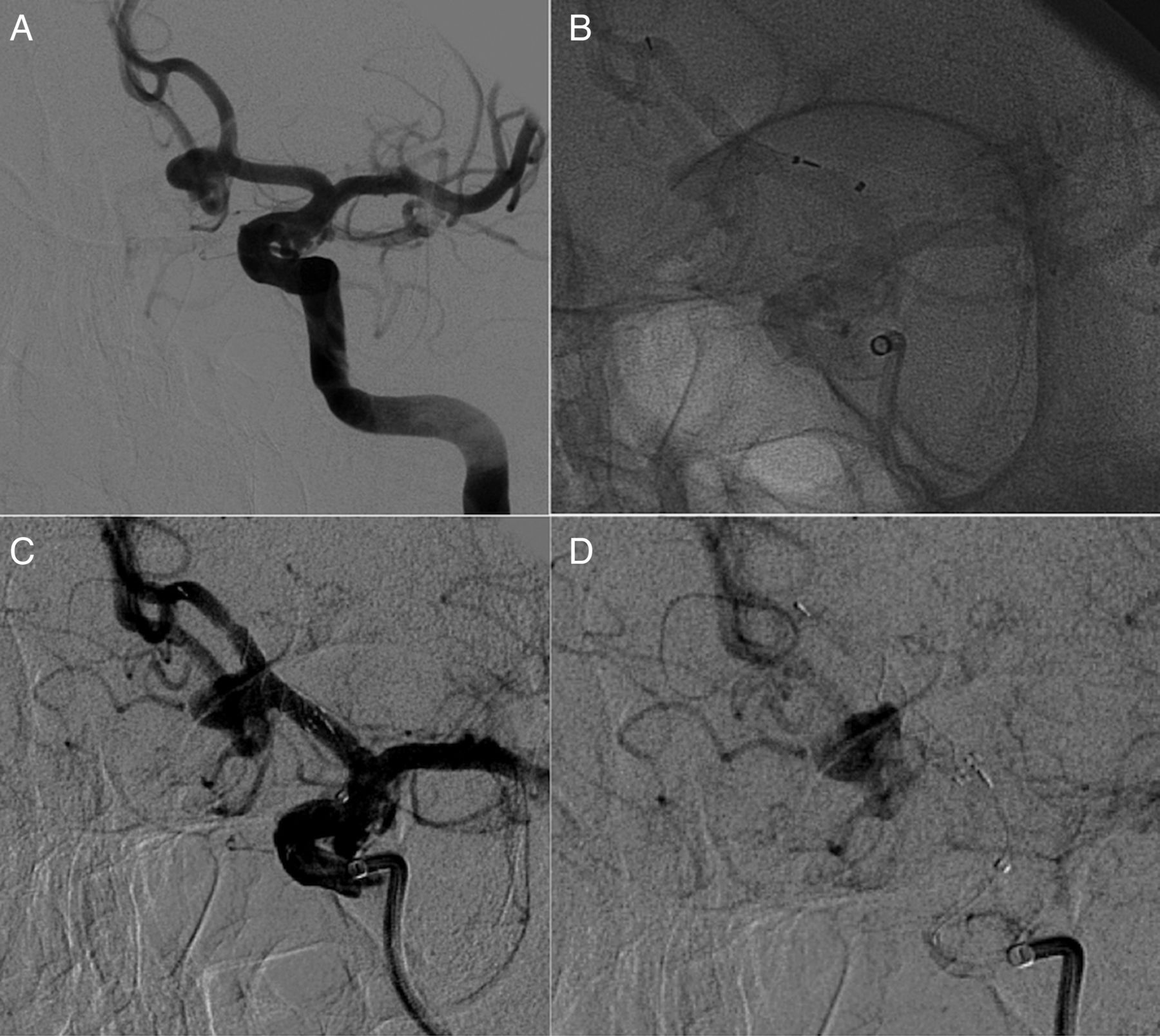
In our patient with an ACoA aneurysm, the p64 FDD offered a good profile, with the possibility of adapting its tubular shape to tortuous and small vessels (<2.5 mm), with good early angiographic results (figure 7).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) A 67-year-old woman harboring a small anterior communicating aneurysm at the corner of the left A2. (B) Non-subtracted images: p64 deployment. Because of the unsatisfactory positioning, the device was retrieved and redeployed (not shown). (C and D) Non-subtracted and subtracted images at the end of the procedure: immediate contrast stasis in the sac.
Our limited experience shows that this new device, which permits 100% retrievability, enables better treatment of ICA aneurysms and also posterior circulation aneurysms and those located beyond the circle of Willis.
Conclusion
The preliminary, immediate and short-term results of this limited series show that treatment with the p64 Flow Modulation Device is safe and has no technical complications. The mechanical detachment, the 100% retrievability, and the 64 nitinol braiding wires are significant advantages of this new device.
However, large prospective studies with long-term angiographic follow-up are necessary to assess the role of the p64 in the endovascular management of intracranial aneurysms.
References
Footnotes
Contributors FB designed the data collection tools, monitored data collection, cleaned and analyzed the data, and drafted and revised the paper. He is guarantor. GL, FM analyzed the data, and drafted and revised the paper. MM monitored data collection, analyzed the data, and drafted and revised the paper. DC monitored data collection for the whole study, and revised the draft paper. FC designed the data collection tools, monitored data collection, and revised the draft paper.
Competing interests FB serves as proctor for Covidien with a modest remuneration. The other authors have no conflict of interest.
Patient consent Obtained.
Ethics approval
We declare that all human and animal studies have been approved by the ethics committe of our institution and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. We declare that all patients gave informed consent before inclusion in this study. The study has been approved by the ethics board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Participants gave informed consent for data sharing.