Article Text

Abstract
The role of simulation in formal neuroendovascular training has not been defined. This report details the general principles underlying the use of simulation in training, the critical aspects of the simulation environment which would aid it as a teaching tool specific to the field of neuroendovascular care, summarizes the available evidence to support a milestone-based curriculum, and outlines an example of what such a curriculum would entail. Building on these foundations, we articulate the rationale for the development and widespread adoption of a simulation curriculum for formal neuroendovascular training.
- Technology
Statistics from Altmetric.com
Simulation as a training tool
The role of simulation in training is long established in the aerospace, flight, and military industries. Increasingly, simulation is being adopted as both a training and evaluation tool for medical services. As a training tool it allows participants to acquire skills; as an evaluation tool it allows analysis of whether the trainees are achieving level-appropriate milestones. Simulation is now widely accepted for enhancing the resident training experience in a wide range of scenarios, including surgical training of laparoscopic procedures,1–4 endoscopy,5 colonoscopy,6 ,7 thoracoscopy,8 cataract surgery,9 peripheral vascular endovascular interventions,10 and airway management.11–13
There are two main components to a procedure that simulation can reinforce. First, the order of steps required to successfully perform a given procedure can be rehearsed under different scenarios (cognitive rehearsal). For example, one can perform A then B then C, and evaluate the outcome of this management algorithm. After the outcome is identified by the simulation system (adverse or desired), another treatment algorithm can be employed in an iterative manner.14 ,15 This learning environment could be separately beneficial and efficient, particularly for relatively rare yet vital occurrences in real-world patient encounters such as critical resuscitation.16 ,17 For example, there is evidence that simulation of cardiopulmonary resuscitative efforts can improve performance and subjective perceptions of self-competence among trainees.17 ,18 Simulation training can also be more efficient, which could become increasingly important especially in the era of work hour reform. There is evidence that an intensive curriculum-based simulation module can be as beneficial as 6 months of clinical ward experience.19
Second, simulation of technical procedures provides a no-risk environment for rehearsal of mechanical skills (technical rehearsal). Simulation has been shown to be effective for relatively simple procedures such as direct or peripherally inserted central venous access catheter placement and transnasal endoscopy.19–22 These findings reflect a transfer of skills acquired from the simulator to an actual patient encounter. It would be expected that the closer a simulation can mimic an actual procedure, the more readily the skills can be transferred. Strategies employing simulation into training must also incorporate periodic retraining of skills to avoid deterioration over time.23
Simulation in neuroendovascular training
Simulation of laparoscopy has been fully incorporated into the training of general surgery residents—that is, general surgery training programs are required under the Accreditation Council for Graduate Medical Education (ACGME) to provide a simulation and skills laboratory for trainees. While a few recent small-scale studies have shown potential efficacy in simulation for neuroendovascular training,24–26 the role of simulation in this arena is yet to be defined.
The benefits of simulation include providing a zero risk environment to both the patient and trainee for the acquisition of imaging and technical skills. Further, there is no use of ionizing radiation in simulation. Repetition is key for gaining proficiency at a mechanical skill, and simulation can provide a safe environment for the repetition of essential skills. This is particularly and intuitively important in the neuroendovascular field in which procedural errors can have devastating neurologic consequences. In addition, a critical aspect of any given procedure can be compartmentalized for repetitive exposure. Simulation of the critical skill—for example, catheterizing a small anterior communicating artery aneurysm with unfavorable anatomy—could be performed in a time compressed and repetitive manner, bypassing the other steps of the procedure including groin access, guide catheter advancement, obtaining working projections, etc. This is of particular benefit for procedures that may be encountered very infrequently. A key learning point from a procedure can be harnessed by uploading to a simulation software system that can then replicate the environment and conditions, allowing the trainee to enhance their skill set as well as allowing others who were not involved in the actual case to benefit from the experience. Additionally, by incorporating patient-specific anatomy from non-invasive imaging, procedure ‘dress rehearsals’ could be performed by the trainee both before and after the actual intervention.
Political challenges in the field
There are challenges that currently exist in the socioeconomic and political climate of the neuroendovascular field which present a challenge for widespread incorporation of a simulation curriculum into fellowship training. The challenge is perhaps best exemplified by the many names it is referred to (neurointerventional surgery, neuroendovascular surgery, neurointerventional radiology, neurointerventional surgical neurology), which reflects the fact that the field is a melting point of three different specialties (neurosurgery, neuroradiology and neurology), each with distinct boards for certification. As such, there is not one unifying authority to oversee this rapidly growing field. As a result, fellowship training is beginning to spiral out of control, with centers sprouting across the country and graduating fellows without central oversight. Absent from a central governing body, there are not any enforceable program requirements with regard to case volume and diversity, center resources, etc. Concern over the quality of fellowship training and market saturation has led several major centers (including ours) indefinitely to suspend fellowship training until a viable solution to this problem is achieved.27 In the near future it is expected that a governing body will be created with representation from all three specialties, with oversight of a certification process that will determine what centers have the volume, case distribution, and faculty commitment to train fellows in the field of neuroendovascular intervention. This would be an opportune time for a milestone-based clinical curriculum to be determined for fellows in training, similar to the ACGME curriculum that is in place for residents at accredited centers. We believe a simulation curriculum will be integral to the efforts of training competent fellows and that incorporation of simulation will be most effective at the inception of a fellowship certification system. To that end, we propose the following outline for a milestone-based simulation curriculum.
Milestone-based simulation curriculum
A milestone-based curriculum for simulation has the advantage of being tailored to the trainee—that is, a first and second year fellow would have a completely different set of expectations of skill sets. The focus of the curriculum would be to achieve milestones in a stepwise fashion, beginning with fundamental core skill acquisition rather than artificial timeframes—that is, a ‘passing score’ would be required prior to proceeding to the next milestone and would be based on demonstrating proficiency at a skill set rather than a fixed time frame. For example, a trainee should not have the expectation or be expected to coil a complex bifurcation aneurysm unless the trainee can (a) perform a thorough diagnostic cerebral angiogram to identify the aneurysm; (b) provide the necessary working angles to understand the relevant anatomy including the relationship of the parent-daughter vessels, aneurysm neck, etc; and (c) devise a treatment plan (balloon-assisted versus stent-assisted versus unassisted) to achieve safe and effective treatment of the aneurysm (figure 1).
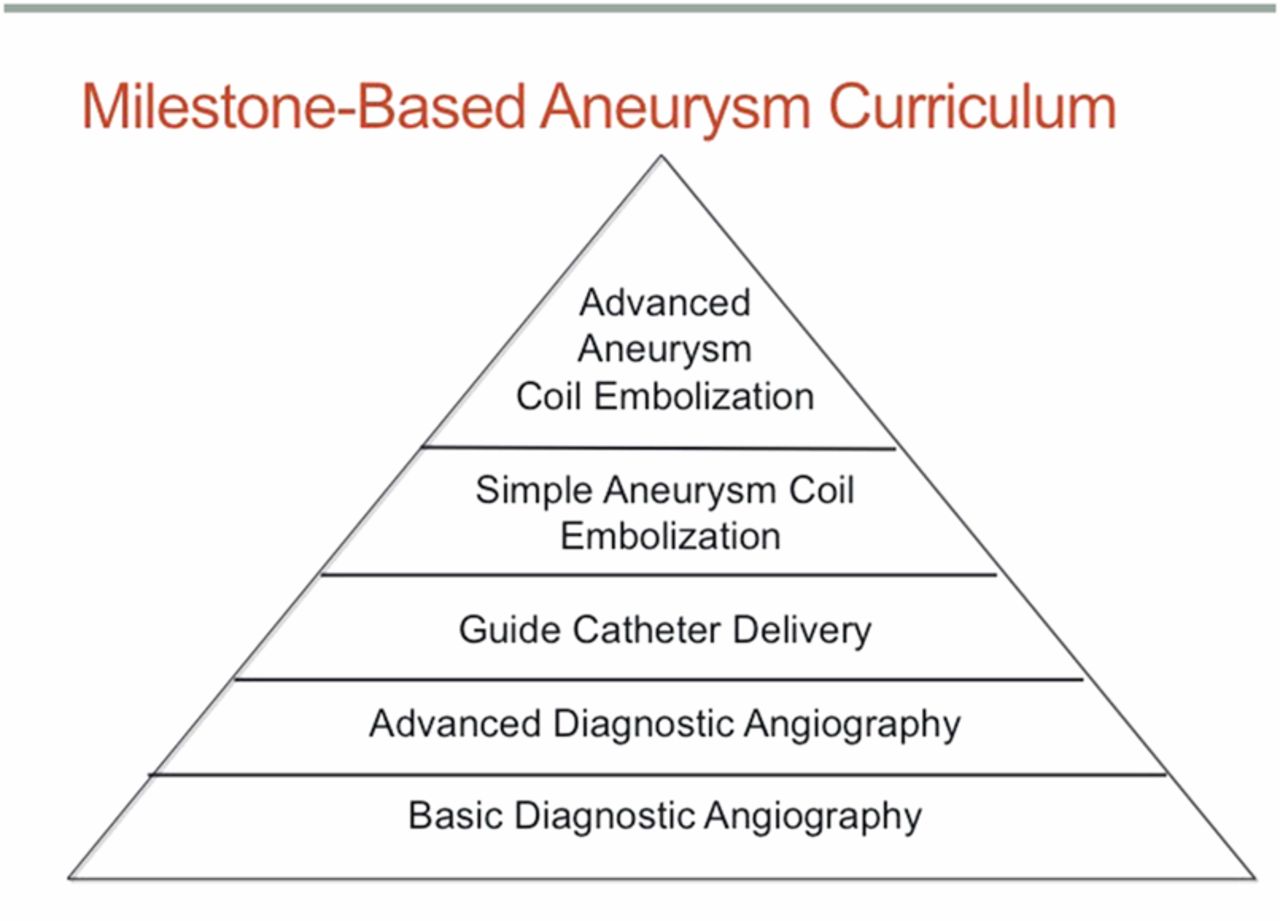
The basis of a curriculum would be to achieve milestones in a stepwise fashion, beginning with fundamental core skill acquisition rather than artificial timeframes. Demonstrating proficiency at a skill set would be required prior to proceeding to the next milestone.
Supervision in simulation training
A simulation environment is not intended to and should not replace appropriate supervision of the trainee during skill set acquisition. Inadequate supervision runs the risk of promoting bad habits to the uninitiated who might place emphasis on speed rather than safety. When supervising a procedure, the teacher would have the opportunity to alter the environment to evaluate the response by the trainee. For example, during the introduction of the first coil into an aneurysm, the teacher could introduce an aneurysmal perforation.
Another advantage of simulation is that every experience would not require supervision. An initial introduction to the skill set could be given to the trainee in both a real and virtual (simulated) environment. A ready example would be forming a secondary curve catheter and selecting a left common carotid artery in a bovine arch. Having been introduced to the technique, the learner could then work on their skill set in the virtual setting. This iterative approach would be expected to occur unsupervised.
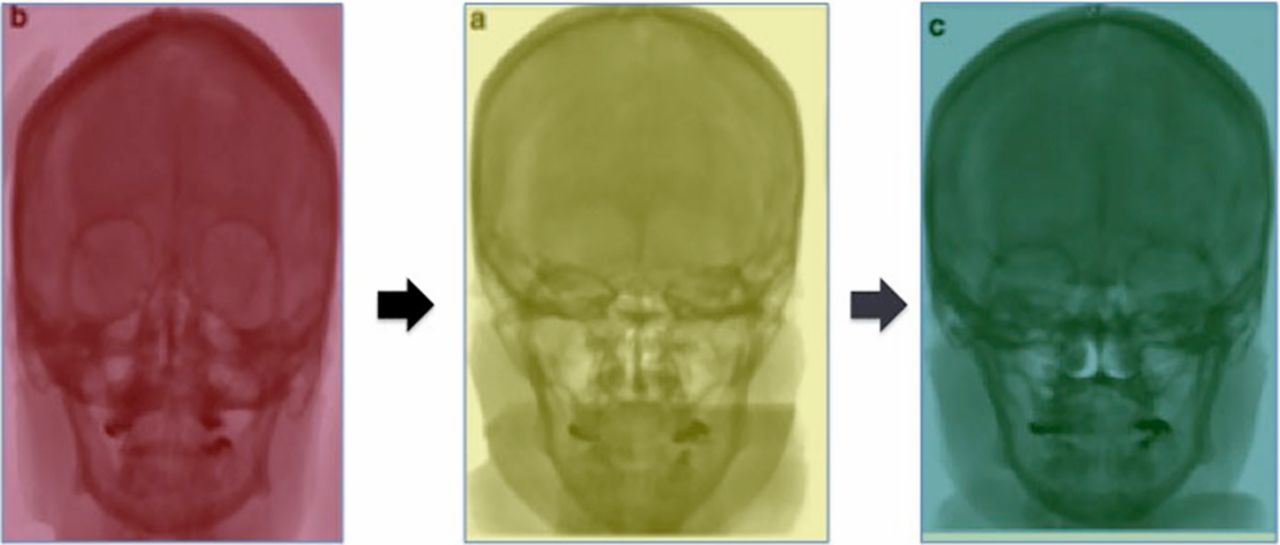
Every mechanical procedure can be broken down into individual steps that must be performed in a stepwise fashion. More sophisticated simulator systems could incorporate feedback such as visual or auditory cues during the procedure marking the completion of each milestone (figure 2). Such a feedback system would provide immediate commentary, reinforcing proper technique and reaffirming to the trainee that the procedure was performed correctly, even in the absence of a formal teacher. This real-time feedback would be more instructive to the learner than remote feedback such as a report at the conclusion of the procedure.
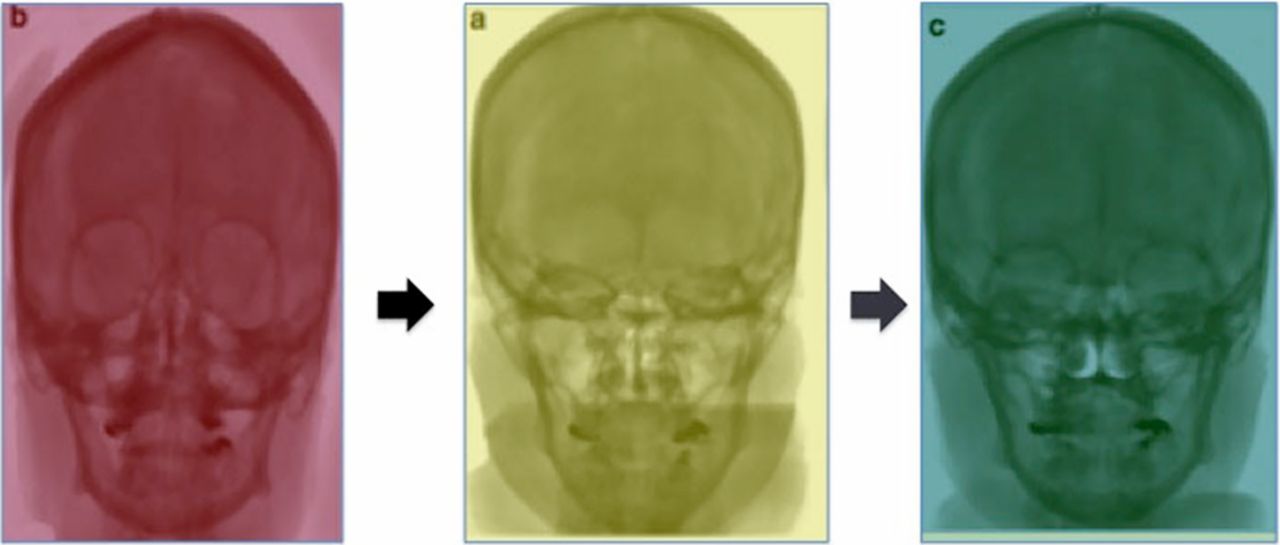
Milestone 1: Core diagnostic surveillance imaging. Standard idealized projections are quantified (cranial/caudal°). Trainees can practice approximating the idealized projection. Visual feedback, in this case a color change signifying achieving an adequate anteroposteior projection, provides immediate feedback to the trainee to correct the projection.
Evidence in support of simulation in neuroendovascular training
Historically, simulation training in the field of neuroendovascular surgery has been restricted to animal laboratories and flow models. The limitation of these is that they are costly and require waste of actual products and devices as well as cumulative and unnecessary radiation exposure. Recently, sophisticated neuroendovascular simulators employing a digital virtual reality are available and pilot programs incorporating them to train neurosurgical residents have been promising.24–26 There are several different software systems available for simulating angiographic procedures. The most extensively studied system is the Simbionix simulator (Simbionix USA Corp, Cleveland, Ohio, USA). Simbionix provides an interactive biplanar fluoroscopic display to perform both diagnostic and interventional procedures on a number of ‘patient’ case scenarios with unique vasculatures. A broad selection of groin sheaths, diagnostic catheters, guide catheters, guidewires, and microwires may be selected and the software incorporates the unique mechanical properties of each. While the behavior of the catheter in the vessel is simulated, actual catheter and wire manipulations are incorporated by motion tracking sensing capabilities in the hardware component of the simulator. The tracking system measures the horizontal translation and roll of each tool at the fixed insertion point, and these values are translated into the simulated space. Each catheter and wire combination is defined by its set of biomechanical properties, such as shear (angulation and torquability) and Young's modulus (stiffness measure).
To simulate the behavior of the catheters as they are navigated in the vasculature, the software then calculates the collision of the catheter and wires with the vessels. Each vessel applies a force vector to a catheter segment in order to maintain the position of the catheter within the intraluminal compartment. The magnitude of this force vector is an adjustable parameter that may have different values along the vessel. Combining the catheter properties with the vessel properties, the software determines the physical state that balances the outer force vectors (applied from the vessel on the tool) and the inner force vectors (the energy required to maintain the tool in its conformational shape rather than return to its free space configuration). In this manner, information such as angulation, friction and forward loading are all incorporated into the algorithm to produce haptic feedback and allow the catheters to navigate in a realistic fashion. Simulated contrast can be administered during both simulated real-time fluoroscopy and digital subtraction angiography. Roadmap assistance for navigation can also be simulated.
We previously reported the results of a pilot study designed to test the feasibility of incorporating the Simbionix simulator in uninitiated trainees.26 Neurosurgical residents in their postgraduate years 1–5 with little or no prior experience in diagnostic angiography and vessel selection were recruited into a standardized training protocol consisting of a didactic demonstration and hands-on learning environment. First and second year fellows with considerable vessel selection experience served as internal controls. The results demonstrated significant improvements in procedural and fluoroscopic times among trainees, reflecting improved catheter technique for angiography on a simulator over a short period of time. Residents who lacked formal training and experience in angiography were able to complete the task in a time approaching that of the experienced fellows at the completion of the training.
The initial pilot program used a simple type I arch as the platform upon which to learn basic vessel selection technique with a primary curve catheter. It was followed by a study investigating the utility of a simulation-based training curriculum for acquiring skills employing a secondary curve catheter in the setting of complex arch anatomy. In this case, trainees with moderate exposure to vessel selection techniques —that is, having ‘passed’ Milestone 1: Basic vessel selection—were enlisted to determine if the benefits of simulation training can be extended beyond straightforward anatomy to a novel challenging task requiring more advanced catheter skill sets. Using a similar learning experience consisting of a didactic demonstration and hands-on time, residents became more proficient at vessel selection in a type II and bovine arch over a relatively compressed time period, with objective data demonstrating more efficient completion of the task.
These findings provide preliminary data in support of a stepwise milestone-based training curriculum for neuroendovascular simulation training. Despite the potential utility of such software simulation systems in ‘dry lab’ settings, there are a number of shortcomings that must be addressed in future iterations. Currently, percutaneous arterial access is not simulated, and neither is the critical skill set of maintaining catheter hygiene including flushing and injections to prevent air from entering the system and thromboembolic events. Catheter flush maintenance becomes increasingly important as the system becomes more complex with tri- and quad-axial catheter combinations, rotating hemostatic valves, etc. For this reason, a combination of both ‘dry’ and ‘wet labs’ which would involve flow models may be beneficial. The cost of acquiring such simulation systems may be prohibitive, and we envision a system in which several Centers of Excellence host trainees from other institutions at various time points during their training rather than expecting each institution to house a fully equipped simulation laboratory. Lastly, biplanar table control is another skill set that is not adequately replicated with the currently available simulation systems. Integrating the simulator with the biplane equipment (figure 3) would overcome such an obstacle and allow trainees to simulate cases in the actual biplane suite while learning the hand and foot pedal controls without exposing themselves or patients to unnecessary radiation.

{kind=link}
{kind=link}
{kind=link}
(A, B) Integration of the simulation system with the biplanar angiography suite would allow acquisition of table controls, including hand and foot pedals, in a radiation-free environment. This could further enhance the simulation experience by allowing cases to be performed in the angiography suite. Multidisciplinary exercises involving anesthesia, nursing, and technician personnel on how to respond in the event of an intraprocedural crisis could be incorporated to optimize the working team dynamic.
Further investigation should incorporate a larger number of participants across a broader range of backgrounds from across multiple centers in the USA. We encourage a widespread and uniform effort to build and incorporate a simulation training curriculum into formal neuroendovascular surgery training.
Milestone-based aneurysm curriculum
Milestone 1: Core diagnostic angiography
Core imaging skill set
Principle: Imaging is fundamental to any neurointerventional procedure. The treatment algorithm will depend entirely on understanding the relevant anatomy. Image acquisition should be approached in a standardized fashion (eg, standard anteroposterior and lateral views), but then tailored to the individual patient's pathophysiology (eg, performing an Alcox maneuver to better delineate the relationship of a posterior communicating artery to an aneurysm).
Standard imaging projections
The trainee should demonstrate the ability to obtain standard anteroposterior and lateral projections as well as standard magnified oblique views
These projections are of high yield for the identification of commonly encountered neurovascular lesions
Core vessel selection/catheter skill set
Principle: Vessel selection for the purposes of performing diagnostic cerebral angiography is fundamental to any neurointerventional procedure.
Proficiency with a primary curve diagnostic catheter (type I, II arch)
The trainee should demonstrate the ability to catheterize the four arteries supplying the head and neck: bilateral carotid and vertebral arteries
Milestone 2: Advanced diagnostic angiography
Advanced imaging skill set
Principle: Working projections are necessary to safely treat intracranial aneurysms by interrogating the neck, the origins of the parent and daughter vessels, etc.
Working projection
The trainee should demonstrate the ability to provide working projections on aneurysms of varying complexities, anterior and posterior circulation
Trainees should identify when a three-dimensional (3D) rotational angiogram will aid in obtaining working projections, and how to use the 3D images to optimize the working projection
Advanced vessel selection/catheter skill set
Principle: Vessel selection in challenging arch anatomy for the purposes of performing diagnostic cerebral angiography is fundamental to any neurointerventional procedure.
Proficiency with a secondary curve diagnostic catheter (type II, bovine, anomalous arch)
The trainee should demonstrate the ability to catheterize the four arteries supplying the head and neck: bilateral carotid and vertebral arteries.
Milestone 3: Guide catheter delivery
Principle: Safe guide catheter delivery to the vessel of interest is fundamental to any neurointerventional procedure. The guide catheter provides support for micronavigation and sufficient luminal volume to introduce microcatheters, stent delivery catheters, balloon catheters, etc. No intracranial lesion can be addressed without first safely delivering an appropriately sized guide catheter.
Guide catheter delivery
The trainee should demonstrate the ability to advance a guide catheter from the aortic arch into the vessel of interest
‘Pitfalls’ introduced to maximize learning experience and assess how the trainee will respond: challenging cervical curvature, bifurcation atherosclerosis, catheter-induced vasospasm, flow stagnation, dissection, etc.
The trainee will have the opportunity to demonstrate skill sets using coaxial and triaxial catheter systems, over-the-wire catheter exchanges, in addition to heparin and calcium channel blocker administration.
Milestone 4: Simple aneurysm coil embolization
The trainee will need to demonstrate competence in:
Aneurysm microcatherization including selecting a favorable tip configuration (straight, 45°, 90°, ‘C’ shape, etc) and microwire combination. Emphasis on technique and control of devices.
Coil selection by size, length and shape as well as coil introduction. Emphasis on keeping the coil mass contained within the aneurysm and achieving complete or near complete aneurysm occlusion (Raymond 1 or 2) with a satisfactory coil packing density (>30%).
‘Pitfalls’ introduced to maximize learning experience and assess how the trainee will respond: aneurysm perforation, coil herniation, thrombus formation on coil, loss of a daughter branch, etc.
The trainee will have the opportunity to demonstrate management schemes to address such pitfalls in addition to protamine and antihypertensive medication and external ventricular drain (EVD) placement.
Milestone 5: Advanced aneurysm coil embolization
The trainee will need to demonstrate competence in:
Balloon and/or stent selection including size (diameter and length): emphasis on technique and control of devices
Emphasis on protecting the daughter vessels and achieving complete or near complete aneurysm occlusion (Raymond 1 or 2) with a satisfactory coil packing density (>30%).
References
Footnotes
Contributors All authors made a material contribution to the article, the revision of the article, and the final approval of the article for submission to this journal.
Competing interests AST, RDT, AMS, and MIC have the following interest: Consultant – Microvention, Penumbra, Stryker, Medpace, Medina Medical, and Covidien. Research grants – Penumbra, Microvention, and Stryker. Advisory Committee – Penumbra, MedPace, Medina Medical, and Stryker.
Provenance and peer review Not commissioned; externally peer reviewed.