Article Text

Abstract
Background and purpose Endovascular recanalization in ischemic stroke is often performed under general anesthesia. Some studies have shown a detrimental effect of general anesthesia. The reasons are unknown.
Methods This was an observational study with retrospective and prospective phases. From 2008 to 2010, 60 patients treated by endovascular recanalization due to proximal vessel occlusion were analyzed with regard to ventilation parameters, blood gas values, blood pressure, and clinical parameters (pre-protocol phase). Subsequently, a protocol with target values for end-tidal CO2 (Petco2) and systolic blood pressure (SBP) was introduced and prospectively analyzed in 64 patients in 2012 (protocol phase).
Results In the pre-protocol phase, significant hypocapnia (<30 mm Hg), a decrease in SBP after intervention (p<0.001), and an increase in SBP after extubation (p<0.001) were observed. After implementing the protocol in 2012, 63% of Petco2 values and 55% of SBP values (median) of the duration of intervention were within the predefined range. Severe hypocapnia and hypotension (SBP <100 mm Hg) after the intervention were significantly reduced. Longer duration of Petco2 values within 40–45 mm Hg, intracerebral hemorrhage, longer door to needle time, older age, unsuccessful recanalization, longer duration of endovascular treatment, and higher cumulative dose of norepinephrine were associated with an unfavorable outcome (modified Rankin Scale score >2). Intracerebral hemorrhage (OR 0.028, p=0.001), age (OR 0.9, p=0.013), and cumulative dose of norepinephrine (OR 0.142, p=0.003) were independent predictors of an unfavorable outcome.
Conclusions In patients receiving endovascular stroke treatment under general anesthesia, the cumulative dose of norepinephrine was an independent predictor of an unfavorable outcome. Further studies are needed to evaluate the optimal management of blood pressure in these patients, and whether avoidance of catecholamines could partly explain the improved outcomes for patients treated under conscious sedation in retrospective studies.
- Angiography
- Blood Pressure
- Intervention
- Stroke
- Thrombectomy
Statistics from Altmetric.com
Introduction
Despite discrepancies between recanalization success and clinical outcome, recanalization by mechanical thrombectomy with stent retrievers is currently often chosen for the treatment of acute ischemic stroke (AIS) with middle cerebral artery, internal carotid artery, or basilar artery occlusion in larger stroke centers. Whether these interventions should be done using intubation and general anesthesia (GA) or conscious sedation (CS) in spontaneously breathing patients is debated.1–3 Physicians favoring GA argue that stenting in intracranial arteries can be difficult, and small movements can cause complications such as vessel rupture and imprecise device placement. In addition, intubation may prevent aspiration, increase patient comfort, and help improve and accelerate the intervention.4 Those in favor of CS reason that time to treatment is shorter, and the detrimental side effects of intubation and mechanical ventilation can be avoided. Indeed, several retrospective studies have suggested outcome advantages for CS compared with GA for endovascular stroke treatment.5–9 Potential mechanisms for the association between GA and poor outcome are not known. Davis et al7 found an association between anesthesia induced hypotension and worse outcome, and a benefit for a systolic blood pressure (SBP) >140 mm Hg. In addition to blood pressure, the effect of the partial pressure of carbon dioxide (Paco2) on the cerebral microcirculation via cerebral vasodilation has been suggested as another important influence on the outcome of patients undergoing endovascular recanalization under GA.10 A retrospective study in 106 patients undergoing endovascular treatment has recently demonstrated that hypocapnia increased the risk of an unfavorable outcome.11
The present study had three objectives: (a) to test, in the pre-protocol phase, whether derangements in SBP and CO2 occur to a relevant degree in patients with occlusion of the internal carotid artery or middle cerebral artery that were treated by endovascular recanalization; (b) to prospectively test the feasibility of applying a protocol directed at target ranges for SBP and Petco2 in a comparable cohort; and (c) to analyze correlations between these parameters and other intervention related parameters with outcome at 3 months.
Methods
This study was approved by the local ethics committee of the Medical Faculty, University of Heidelberg; informed consent was waived as the study was observational and data collection was done as part of clinical routine (reference number S-189/2013).
General anesthesia was used in all patients in this study. In the pre-protocol phase from 2008 to 2010, we retrospectively analyzed all patients from an internal hospital database who underwent endovascular recanalization for AIS due to occlusion of the internal carotid artery or middle cerebral artery. In our hospital, only patients with a National Institutes of Health Stroke Scale (NIHSS) score of >10 were treated using this therapy. Additional information was gathered by evaluation of medical charts from our digital archive.
All patients were treated according to a previously published standard operating procedure (SOP).12 Intubation was performed in the neurointensive care unit by a neurointensivist and experienced nursing staff. We used intravenous etomidate (20 mg, 40 mg in rare cases with insufficient sedation) for sedation, fentanyl (0.2–0.3 mg) for analgesia, and rocuronium (50 mg) as a muscle relaxant. Sedation was continued using intravenous propofol and intravenous remifentanil (120–300 mg/h and 0.3–0.8 mg/h, respectively). During the intervention, a neurointensivist with experience in managing ventilated patients with acute brain injuries was in charge of monitoring the patient's vital signs and ventilation settings. A interventionalist with several years’ experience in interventional neuroradiology was exclusively involved in the recanalization procedure but not in the systemic or ventilator management.
We assessed the door to needle time in patients receiving recombinant tissue plasminogen activator, method of recanalization, age, NIHSS score on admission and at discharge, any intracerebral hemorrhage (ICH), symptomatic ICH (sICH; according to the European Cooperative Acute Stroke Study (ECASS) definition: increase in NIHSS score of ≥4 points or leading to death), modified Rankin Scale score at 90 days (obtained by telephone interview of the patient, relatives, or general practitioner as part of our prospective hospital registry), ventilation parameters after the intervention (tidal volume, breathing rate, positive end-expiratory pressure peak pressure), blood gas analysis after the intervention (while patients were still mechanically ventilated), SBP before the intervention, after the intervention for a period of 10 h or until extubation, SBP after extubation for 10 h, and time until extubation. In the pre-protocol phase, no data were available on these parameters during the intervention itself. Monitoring at that time was not available for analysis.
We then developed a protocol with predefined target values during the intervention based on pathophysiological assumptions and suggestions from previously published articles.7 ,10 For Petco2, a target range of 40–45 mm Hg was chosen, as mild hypercapnia was shown to increase cerebral blood flow in patients with intact autoregulation13 and this was regarded as beneficial for the ischemic penumbra. For SBP, a target range of 140–160 mm Hg was chosen. Hypotension directly after intubation was treated with a bolus dose of norepinephrine and norepinephrine infusion. The dose was adapted to SBP during the intervention. Norepinephrine was routinely given through a peripheral line in the arm that was not used for blood pressure measurements to avoid fluctuations in administration. Extravasation or vessel irritation due to norepinephrine is not a relevant issue in our practice. Our blood pressure targets did not change during or after the intervention in any part of the protocol phase of the study.
A new chart for data collection during the intervention was introduced, in which type of sedation, blood pressure, catecholamine dose, heart rate, O2 saturation, Petco2, ventilation settings, body temperature, and application of additional medication were documented at least every 10 min. Blood pressure was measured at least every 5 min. The initial impression was that documentation of these values at 10 min intervals was enough as patients were thought to be fairly stable during the intervention. Based on our findings reported here, however, we recently changed the protocol. Currently, pulmonary and circulatory parameters are recorded every 5 min. In addition, all remaining parameters assessed in the pre-protocol phase were also collected prospectively. In 2012, we tested the application and the effects of this goal directed protocol in patients with anterior circulation AIS due to proximal vessel occlusion with an NIHSS score >10. All patients received cranial CT and CT angiography or cranial MRI and MR angiography, and were considered adequate for mechanical recanalization after an interdisciplinary discussion between neurologists and neuroradiologists.
Clinical outcome was assessed 3 months after stroke by an investigator not blinded to the treatment but to the analysis by standardized telephone interview or inpatient visit using the modified Rankin Scale. Good outcome was defined as a score of 0–2 on this scale (ability to live independently).
Statistical analysis was done using Microsoft Excel V.2003 and SPSS V.21. Descriptive data analysis was performed, and reported p values are to be interpreted accordingly.14 Medians with IQRs were given for descriptive statistics for all variables. Univariate analysis was performed using the Wilcoxon rank sum test or χ2 test for continuous or binary variables, respectively, for comparisons between two independent groups. Multivariate analysis was done applying binary logistic regression models. Variable selection was performed using the backward elimination method based on likelihood ratio tests where variables were removed if the related p value was above 0.10. Two-sided p values are reported throughout.
Advice on statistical analysis was obtained from the Institute of Medical Biometry, University of Heidelberg.
Results
Retrospective study (pre-protocol, 2008–2010)
Some of the data from this patient population have been used in previous publications, but different variables were investigated with respect to different study subjects, such as saving time in the preparation of patients for recanalization12 or the role of hemoglobin.15
From 2008 to 2010, 80 patients with AIS and occlusion of a large vessel were treated with mechanical recanalization under GA. Nineteen patients were excluded because they suffered from basilar thrombosis; one was excluded because the required data were incomplete. Of the remaining 60 patients, the following median values were calculated from the first recorded blood gas analysis and corresponding ventilation settings after the intervention: tidal volume 593 mL (IQR 504–699), Paco2 33.0 mm Hg (IQR 25.3–37.8), pH 7.45 (IQR 7.37–7.51), and Pao2 181.0 (IQR: 128.0–252.5). For circulatory measurements in the first 10 h after intervention, median baseline SBP before the endovascular intervention (in the emergency room) was 150.0 mm Hg (IQR 140.0–170.0); SBP after the intervention was 134.0 mm Hg (IQR 122.5–143.5), resulting in a statistically significant median pre–post intervention difference in SBP of −19.5 mm Hg (IQR −37.6–0.75; p<0.001). After extubation, median SBP increased to 146.0 mm Hg (IQR 131.0–159.0), resulting in a statistically significant difference from intubation to extubation of +9.0 mm Hg (IQR −3–23; p<0.001). These results are summarized in figure 1.

Pre-protocol phase. (A) Systolic blood pressure (SBP) values at different time points in relation to the intervention. (B) Distribution of tidal volumes measured after the intervention. (C) Distribution of arterial carbon dioxide tension (Paco2) values measured after the intervention.
ICH was present in 30 cases; only four of these were symptomatic using the ECASS definition. Outcome data after 90 days were available for 43 patients. Only six had a favorable outcome.
Prospective study (protocol, January 2012 to December 2012)
In the protocol phase, 96 patients with AIS were treated by endovascular recanalization. For 83 patients, follow-up data of sufficient quality were available. Thirteen patients were excluded because they had an occlusion in the posterior circulation. Six patients were excluded because documentation during the intervention was incomplete. Hence 64 patients were analyzed.
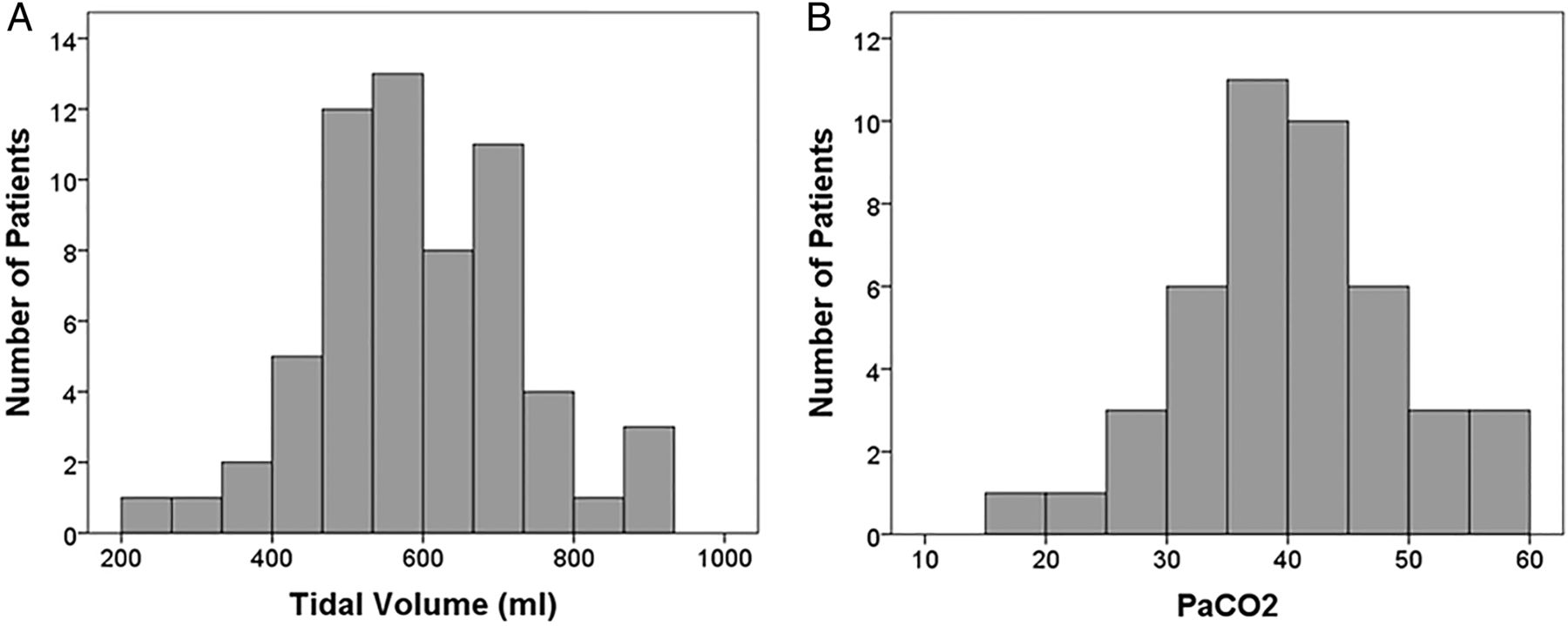
Petco2 was kept within the target range during 63% (median, IQR 0–87) of the intervention. Comparing median values for Paco2 in the neurointensive care unit (in the first blood gas analysis after the intervention) between the pre-protocol and protocol phases, a significant increase was found (33.0 mm Hg, IQR 25.3–37.8 vs 39.9, IQR 34.6–47.0; p<0.001). A corresponding difference was found for pH (7.45, IQR 7.37–7.51 vs 7.36, IQR 7.31–7.41; p<0.001). Tidal volume and Paco2 in the protocol phase are displayed in figure 2. SBP was within the predefined range for 52% of the duration of the intervention (median, IQR 34–80). In contrast, there was no significant difference between SBP values before or after intervention, or before or after extubation. The median modified Rankin Scale score after 90 days was 3 (distribution of scores: 0 (8%); 1 (16%); 2 (19%); 3 (9%); 4 (17%); 5 (5%); 6 (27%)).

Protocol phase. (A) Distribution of tidal volumes measured after the intervention. (B) Distribution of arterial carbon dioxide tension (Paco2) values measured after the intervention.
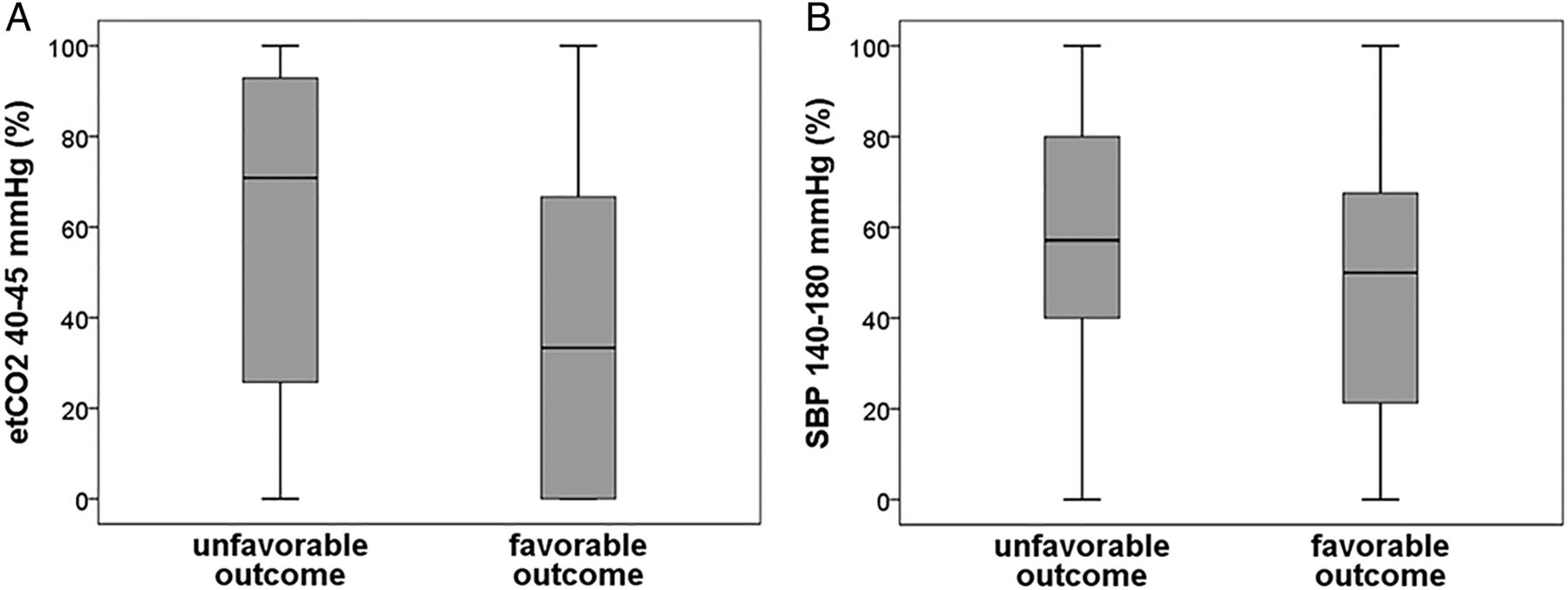
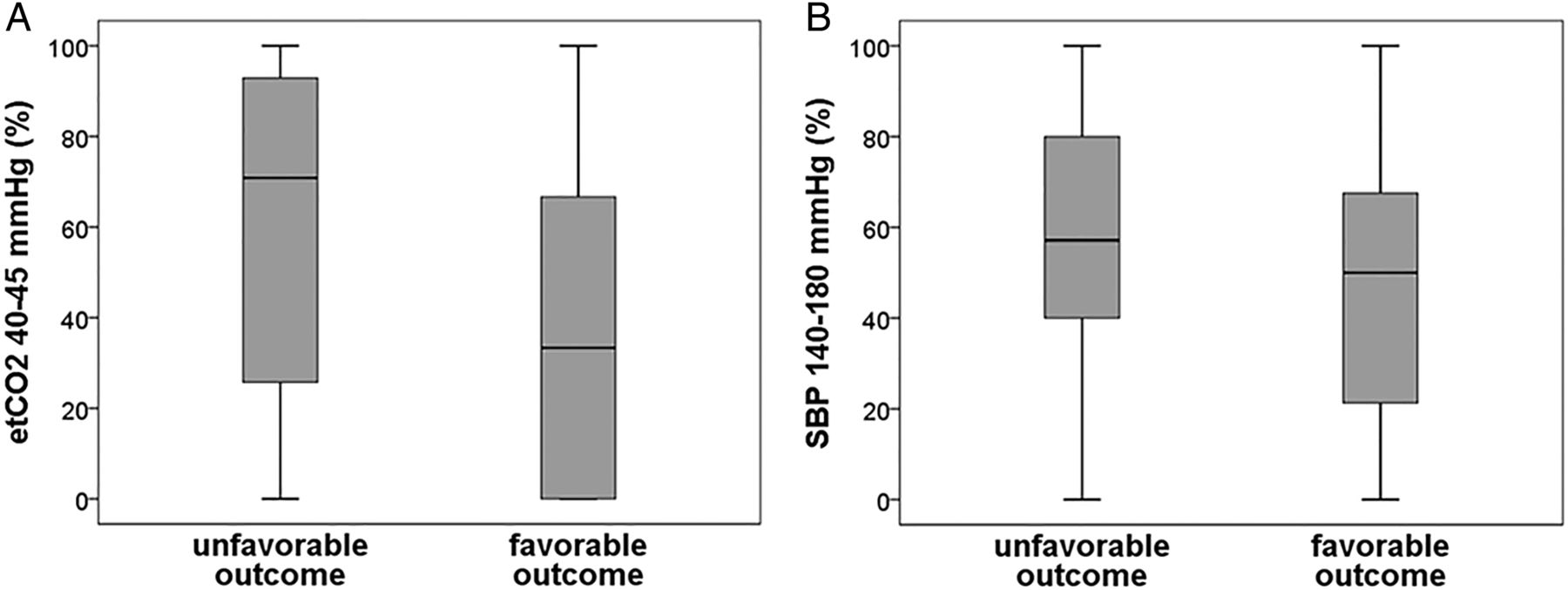
In a subsequent univariate analysis, the following parameters were associated with an unfavorable outcome: longer time in the Petco2 range of 40–45 mm Hg (p=0.04), any ICH (p=0.001), longer door to needle time for alteplase (p=0.03), longer duration of intervention (p=0.001), older age (p=0.03), incomplete recanalization (Thrombolysis in Cerebral Infarction <2b, p=0.013), and higher cumulative dose of norepinephrine required to stabilize the blood pressure (p=0.001) (table 1, figure 3).
Factors associated with outcome: univariate analysis
{kind=link}
{kind=link}
{kind=link}
Protocol phase. (A) Percentage of end tidal carbon dioxide tension (Petco2) values within the range of 40–45 mm Hg during the intervention. (B) Percentage of systolic blood pressure (SBP) values within the range of 140–180 mm Hg during the intervention.
The median gradient between the first Paco2 obtained after the intervention and the temporally closest Petco2 was 0.2 (IQR −3.4 to 7). ICH occurred in 21 patients. Only four of these were sICH by the ECASS definition. The rate of sICH was not different between the groups. Median SBP was not different between the groups. The median value was within the target range (141 and 142 mm Hg for favorable and unfavorable outcome, respectively). Nonetheless, blood pressure drops >20 mm Hg occurred in 51% of patients. This was not significantly different in patients with a favorable or unfavorable outcome. Although there were a higher percentage of values between 140 and 180 mm Hg and a higher decrease in baseline to median blood pressure during the intervention in patients with an unfavorable outcome, this did not reach statistical significance. Only one patient did not receive norepinephrine and was included in the analysis (0 mg).
To identify independent predictors of an unfavorable outcome, we applied backward variable selection starting with the binary logistic regression model including all variables that were statistically significant in the univariate analysis. Any ICH (p=0.001; OR 0.028; CI 0.004 to 0.21), cumulative dose of norepinephrine (p=0.003; OR 0.142; CI 0.038 to 0.525), and age (p=0.013; OR 0.9; CI 0.852 to 0.981) were found to be independent risk factors predicting an unfavorable outcome (table 2). The effect of norepinephrine was independent of the duration of the intervention (p=0.719).
Predictors of good outcome: binary logistic regression (n=64)
To investigate the influence of arterial collateralization, we analyzed a subgroup of 33 patients who received CT angiography instead of MR angiography initially, as CT angiography based scoring is the only non-invasive scoring method that has been validated and tested for reliability regarding collateralization status.16 We found that 60% of patients with moderate or good collaterals had a favorable outcome while only 28% of those with poor collaterals had a favorable outcome. This is in line with previous studies, although it did not reach statistical significance, probably due to the small sample size. Subgroups of patients with good and poor collaterals did not show any difference in Petco2 or SBP values (data not shown).
Discussion
The present study produced three main results. (1) The introduction of a goal directed SOP may have helped to avoid severe hyperventilation and hypotension in the post-intervention period after endovascular treatment of patients with anterior circulation AIS under GA. (2) A higher percentage of time of Petco2 values within the range of 40–45 mm Hg was associated with an unfavorable outcome in the univariate analysis. (3) The cumulative dose of norepinephrine was as independent predictor of outcome.
After implementation of the protocol, we successfully influenced the rate of hypocapnia and hypotension after the intervention. However, the achievement of target values during the intervention was still low in our study (63% and 55% for Petco2 and SBP, respectively), probably due to suboptimal adherence on the part of the managing neurointensivists and/or difficulty in fulfilling protocol goals in individual patients. But the implementation may still have helped to reduce extreme values. This suboptimal achievement means, on the one hand, that we could not fully judge the effect of the protocol and guarantee consistent management of the patients. On the other hand, it gave us the chance to evaluate the effects of different Petco2 and SBP values during the intervention in two almost equally sized groups. For future optimization of protocol adherence, we would probably have to improve the education of staff regarding the protocol and control its adherence by external monitoring. A favorable outcome occurred in only 14% of patients who underwent our pre-protocol. This may be explained by several factors. Firstly, endovascular stroke treatment was only beginning to be used more systematically in our hospital in 2008 (number of interventions of the anterior circulation was 6 in 2008 compared with 83 in 2012). Secondly, a variety of devices or intra-arterial alteplase alone were used in the first years, whereas approximately 90% were treated with stent retrievers in 2012, yielding much better recanalization rates. Thirdly, an SOP that led to a significant decrease in door to recanalization times was only introduced at the end of 2009.12 For these reasons, we did not compare outcome parameters between the pre-protocol and protocol phases.
The optimal Petco2 values for patients with brain damage remain unclear. Currently, many anesthesiologists use mild hyperventilation prophylactically in neurosurgical procedures as intracranial pressure is lowered by hyperventilation through pH induced cerebral vasoconstriction.17 While elevated intracranial pressure during neurosurgical procedures can be a substantial issue, vasoconstriction during an AIS can be detrimental. The penumbra is only supplied by collaterals which might be constricted during any phase of hyperventilation, potentially leading to enlargement of the ischemic area. In the pre-protocol phase, we showed that hyperventilation occurs frequently in our patient cohort, which is in agreement with the data of Takahashi et al.11 On the other hand, mild hypoventilation could lead to a steal phenomenon in areas with decreased cerebrovascular reserve. This was observed in patients with high grade carotid artery stenosis where the application of the vasodilative drug acetazolamide mainly dilated vessels in the unaffected brain regions, potentially decreasing cerebral blood flow to hypoperfused areas where vessels are already maximally dilated.18 A similar pathophysiological effect may occur in AIS during hypoventilation related vasodilation. This might be the reason for the association of Petco2 values of 40–45 mm Hg with an unfavorable outcome in the univariate analysis of our study. One other study has studied the effect of Petco2 in these patients.11 The authors found a significantly lower Petco2 during the intervention in patients with an unfavorable outcome, 60 and 90 min after the intervention, but not 30 min after the intervention. Takahashi et al found that the mean Petco2 level was approximately 32 versus 35 mm Hg in the unfavorable compared with the favorable outcome group, respectively. If we consider our results and those of Takahashi et al, the favorable target value for Petco2 in AIS may be approximately 35–40 mm Hg as both mild hyperventilation to Petco2 <35 mm Hg and mild hypoventilation to Petco2 40–45 mm Hg were associated with an unfavorable outcome. In our study this association was seen only in the univariate analysis and so should be interpreted accordingly.
The cumulative dose of norepinephrine was an independent predictor of worse outcome in our study. This effect was independent of the duration of angiography. This is an important finding as norepinephrine is widely used to stabilize blood pressure during interventions. Norepinephrine has a combination of β1 (inotropic and chronotropic) and α agonist effects. One could assume that norepinephrine as a vasoconstrictor could have an adverse effect on the collateral cerebral circulation. This effect, however, seems to be limited in cerebral vessels due to a lower sensitivity and a lower density of α receptors.19 Nonetheless, in a condition of critical hypoperfusion, any small change in collateral blood flow may have a relevant influence on infarct size. In addition, an α receptor independent harmful effect on the brain has been reported.20 Another study found that this effect might be mediated by post-stroke inflammation.21 This may be compatible with our finding that the median norepinephrine dose was not significantly different between groups in contrast with the cumulative dose. A different explanation would be that the greater use of norepinephrine is simply an indication of more severe hypotension in these patients that was only partially compensated by the use of norepinephrine and continued to exert deleterious effects. In this scenario, however, median doses of norepinephrine and median blood pressure values should also have been different between the groups of patients with an favorable and unfavorable outcome. We cannot exclude the fact that a higher demand for norepinephrine mainly reflects more hemodynamic instability. Interestingly, our study, as well as the study by Takahashi et al, did not find a significant effect of blood pressure on outcome. This is in contrast with other studies that have shown a better outcome for patients with blood pressures >140 mm Hg.7 ,9 ,22 In our study, there was a larger decrease from baseline SBP to mean SBP during the intervention in the group of patients with an unfavorable outcome, which did not reach statistical significance. This could be due to the relatively small sample size. We also could not reproduce the previously reported adverse effect of the lowest SBP on outcome.7 ,9 We assume that application of our protocol with predefined target values may have led to less episodes with relevant hypotension so that the blood pressure effects observed by Davis et al7 and Whalin et al9 could not be observed in our study. Although it was not an independent predictor of outcome in our study, blood pressure has been reported to affect AIS outcome in several studies.22–26 Hence we assume that severe hypotension during the intervention is potentially detrimental in AIS and suppose that it should be counteracted. However, whether this should be best achieved by reduction of sedatives, volume administration, or catecholamines (and which type of catecholamine) remains uncertain. It may thus be more beneficial to use sedatives with less hypotensive side effects and use the lowest possible dose. Our findings raise the possibility that correcting hypotension seen in GA with vasopressors may not improve clinical outcomes and therefore GA should be avoided in patients who can safely receive CS. Indeed, several retrospective studies indicate that GA is inferior to CS in endovascular stroke care27 and our study may have addressed some of the contributing factors. However, this current controversy of GA versus CS has to be solved by prospective randomized trials.
Our study has several limitations. Data in the pre-protocol phase were retrospective, with all of the usual inherent limitations. In addition, it was not possible to conduct a proper before and after design with identical groups of patients as there were no systematically documented data available on blood pressure and ventilation in the pre-protocol phase. Furthermore, our findings cannot be easily generalized as they were obtained in a single neurovascular center. Selection bias could have occurred as the study was not randomized and we had to exclude 20 patients due to insufficient data. The reported rates of ICH in our study included any ICH as well as sICH (ECASS definition). If limited to the latter, 6.7% and 6.3% (pre-protocol and protocol phase, respectively) of patients suffered from sICH, which is comparable with that reported in other studies.28 Nonetheless, even asymptomatic ICH seems to have an influence on outcome, possibly reflecting indirect effects of the stroke type, hemodynamics, collaterals, or the interventional procedure, which could not be differentiated further. Due to the relatively high rate of any ICH, other effects on outcome might have been obscured.
The Paco2–Petco2 gradient was quite small, and had partially negative values, so that ventilation settings must have been changed in some of the cases before arterial blood gas was analyzed. For this reason, and for differences in measurement time points, we did not compare Petco2 values in the protocol phase with Paco2 values in the pre-protocol phase but only Paco2 values between the two phases.
Finally, patient numbers in the protocol phase may have been too small to show significant effects in the logistic regression, especially for well known predictive factors for outcome (eg, recanalization status and NIHSS score) and also with regard to Petco2. Although the results from larger trials regarding the known predictive factors were partially reflected in the univariate analysis of our study, this should be interpreted with caution. Another reason amplifying the restrictions of a small sample size with regard to NIHSS score is that only moderate and severe strokes were selected for endovascular treatment. Due to the limited range, it is more difficult to show statistically significant differences with small patient numbers.
Conclusion
In our study, we found that cumulative dose of norepinephrine was an independent predictor of outcome in patients undergoing endovascular stroke treatment under GA. This finding may offer an explanation for the beneficial effect of treating these patients under CS that was found in retrospective studies. Further studies are needed to understand the impact of blood pressure and Paco2 in patients with acute ischemic stroke to optimize peri-interventional stroke care.
References
Footnotes
Contributors SM, JB, and WH designed the study. SM, AS, MW, and MK were involved in data acquisition and analysis. SM, JB, WH, MK, MM, and MB interpreted the data and wrote the manuscript. All authors approved the final version for publication.
Competing interests None.
Ethics approval The study was approved by the local ethics committee of the Medical Faculty, University of Heidelberg.
Provenance and peer review Not commissioned; externally peer reviewed.