Article Text

Abstract
Background One of the primary device expenditures associated with the endovascular treatment of aneurysms is that of detachable coils. Analyzing the cost efficiency of detachable coils is difficult, given the differences in design, implantable volume, and the presence of additives. However, applying a volume per cost metric may provide an index analogous to unit price found in grocery stores.
Methods The price information for 509 different coils belonging to 31 different coil lines, available as of September 2013, was obtained through the inventory management system at the study site, and normalized to the price of the least expensive coil. Values were used to calculate the logarithmic ratio of volume over cost.
Results Operator choice among coil sizes can vary the material costs by five-fold in a hypothetical aneurysm.
Conclusions The difference in coil costs as a function of cost per volume of coil can vary tremendously. Using the present pricing algorithms, using the longest available length at a particular helical dimension and system yields improved efficiency.
- Economics
- Coil
Statistics from Altmetric.com
Introduction/purpose
Coil embolization is currently the most common method of intracranial aneurysm treatment in the USA, and a major revenue driver of neurointerventional surgery. However, compared with surgical clipping, aneurysm recurrence after coiling occurs in a larger proportion of patients.1 ,2
Stable aneurysm occlusion after coil embolization may be related to coil packing density, with lower packing attenuation being associated with higher recurrence rates.3–5
The goal of endovascular therapy for intracranial aneurysms is to achieve an optimal packing density to prevent recurrence and hopefully reduce rupture rates. This treatment strategy requires the deployment of multiple coils of distinct type, shape, length, and size in order to achieve adequate endoluminal volumetric packing of the aneurysm. Selection of each specific coil influences the volume left to be filled by subsequent coils within the same aneurysm in the same treatment session, and therefore impacts on the number of coils, and therefore cost, required to treat each aneurysm.
Given that payment for the treatment of a patient with an aneurysm (ruptured or unruptured) is often set to a specific limited amount, the cost of the devices used during treatment has a direct effect on the profitability and financial sustainability of this therapy. For aneurysm coiling procedures, the cost of each coil and the number of coils used largely determine the total material costs. Coil costs vary significantly on a per unit basis, and no systematic way of evaluating cost efficiency has been established. As the healthcare system becomes increasingly cost sensitive, understanding and controlling costs will prove to be instrumental in maintaining the future health of the specialty while maintaining optimal patient outcomes.
Modeling procedure material costs on a volumetric efficiency basis may help identify methods of simultaneously reducing coiling costs and achieving minimum packing density. To date, no analysis has been done to model this relationship. Here, we have evaluated the efficiency in a cost per volume analysis of the current list of coils available for intracranial aneurysm embolization.
Materials and methods
A comprehensive list of coils was obtained from the inventory at one of our institutions. Coil characteristics were reviewed, including coil type, length, and size of its tertiary structure. Coils were grouped as frame, finish, or fill coils by an experienced interventional neuroradiologist (FKH). Frame coils were determined by tertiary structural elements, and finish coils were determined by size and length. Coil volumes were obtained from the database of AngioSuite Neuro Edition software. Note that coils with hydrogels were assessed at maximal, post swelling volume per AngioSuite volumetric data. Coil efficiency was determined using the logarithmic relationship between the volume of occlusion per each individual coil and the normalized cost of each coil. The cost efficiency value for each coil was then evaluated against coil size.
A model to illustrate cost efficiency comparing the use of various lengths of a single coil line to achieve 30% packing density of a 4 mm spherical aneurysm after prior framing with a 4 mm×7.5 cm Codman Micrusphere Spherical 10 (Codman, Raynham, Massachusetts, USA) was performed and is shown in table 1.
Number of coils of different lengths required to fill a 4 mm aneurysm according to their length
Results
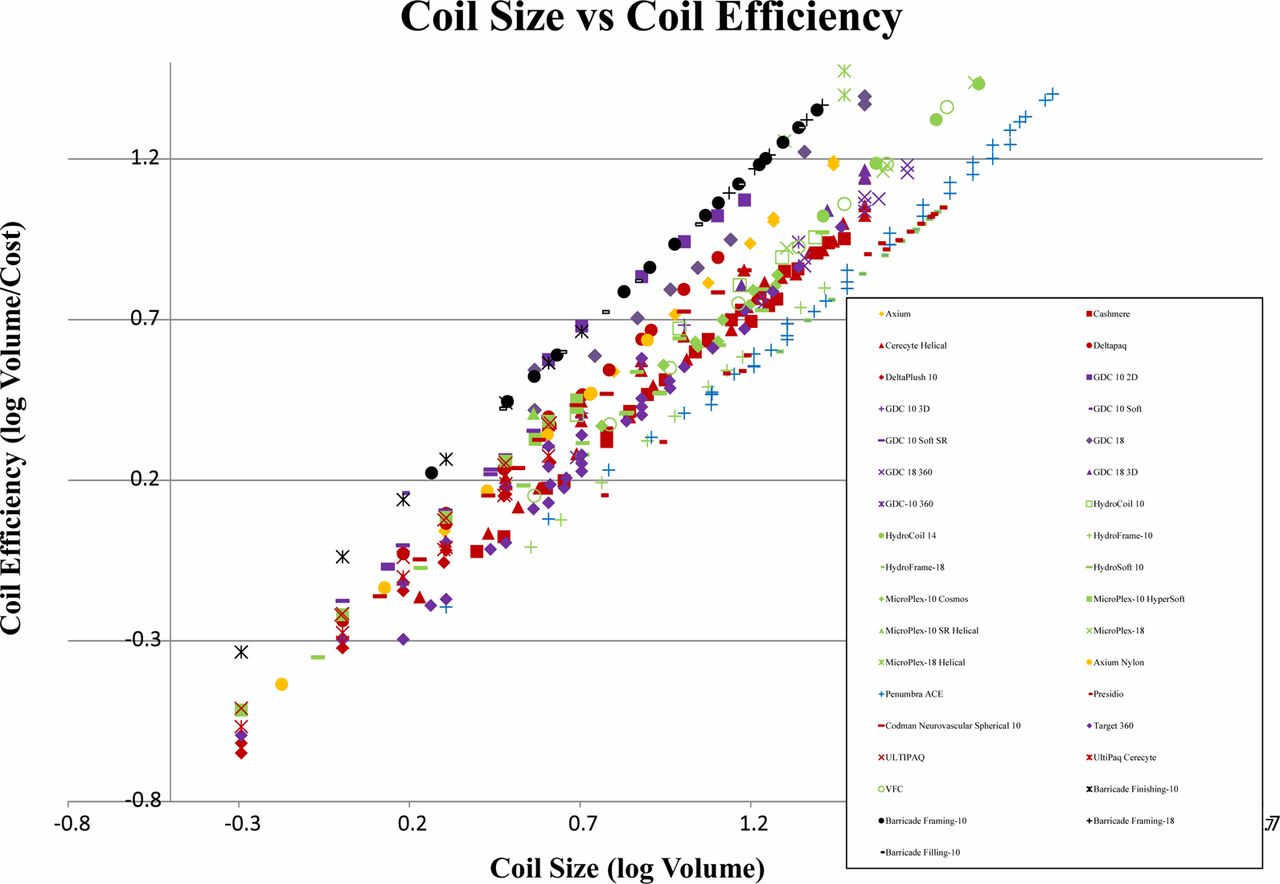
The price information for 509 different coils belonging to 31 different coil lines, available as of September 2013, was obtained through the inventory management system at the study site, and normalized to the price of the least expensive coil. Values were used to calculate the logarithmic ratio of volume over cost, obtaining an efficiency value for each coil. A strong log–log relationship between coiling cost efficiency versus coil size for individual coils was found (figure 1). Linear regression of this relationship over all coils was found to be R2=0.903. Linear regression R2 values were not improved by performing regression on coil subsets partitioned by frame, fill, and finish divisions (R2 values of 0.896, 0.831, and 0.886, respectively). These results are displayed in figure 1.
Operator choice among coil sizes can vary the material costs by five-fold in this particular example.

{kind=link}
Coil size versus coil efficiency, demonstrating a linear relationship. Coils of the same vendor are represented by the same color, and coils of the same product line are represented by the same marker shape.
Discussion
Previous studies of material cost comparisons between coil embolization and surgical clipping tend to conclude that embolization is the more expensive procedure. Brinjikji et al6 recently reported that not only has the cost of endovascular treatment in both uncomplicated and complicated by major mortality cases been found to be more expensive than their surgical clipping counterparts, but also that coiling costs have grown at a faster rate (4.6% vs 3.6% average annual cost increase between coiling vs clipping, respectively). Hoh et al7 reported similar findings and alluded to equipment material costs as the driver of the cost increase. This likely derives from the fact that to treat an aneurysm, several coils are required, in contrast with a single or a few surgical clips, with the number of coils being the major driver of the cost of this therapy. Indirect costs related to surgery may include longer recovery times and hospital stays but is beyond the scope of this paper. Elucidating the mechanisms influencing final equipment cost will enable operators to control costs without sacrificing clinical outcomes.
Our data show that there is a strong positive linear relationship between coil size and coil cost efficiency, as represented by a value of volume of aneurysm filled per cost. A large component of this relationship is the relatively flat pricing structure for coils of the same line, regardless of size. A very long coil which achieves a larger volume of occlusion may have a relatively similar price to a small coil of the same line which would fill a smaller volume of the aneurysm being treated.
Our analysis demonstrates that the largest determinant of coiling cost efficiency is coil length. Factors such as vendors, coil lines, and frame/fill/finish designation were not found to impact coiling cost efficiency. From this analysis, we conclude that using longer coils with larger volumetric filling, compared with smaller coils with lower volumetric filling, will translate to a lower number of coils required, and subsequently reduced cost per aneurysm treated.
To illustrate the wide variance of size determined cost efficiencies between different coils, it would cost 389 times more to coil a hypothetical 1 cm spherical aneurysm to 30% packing density using the least cost efficient coil (Deltaplush 10, 2 mm×1 cm) compared with the most cost efficient coil (MicroPlex-18 Helical, 10 mm×30 cm) (ratios calculated at available institutional prices with currently available coils at the time of data collection). Even the median cost efficiency coil (Target 360, 4 mm×15 cm) would cost 34.5 times as much as the most volumetrically efficient one. Note that the most important determinate of volumetric efficiency was coil length.
Choice of individual coils during embolization depends on several factors, including the experience of the operator, familiarity with a specific coil line, selection of delivery devices, and peri- and intraprocedural factors. Device cost, and overall procedure cost, should not be obviated when selecting devices, especially in our era of medical care cost containment. Awareness of the vast difference in cost efficiency by coil volume may help operators control cost. However, coil selection should be based on cost only after the safety of using a specific coil is considered, and as part of the overall treatment strategy.
This study did not address intrinsic engineering differences in the coils, including material differences, coil structure design, detachment zone design, or detachment devices. The use of longer coils with a better cost efficiency ratio will fill larger volumes compared with shorter coils, and will translate into a smaller number of devices being implanted. This may also translate into shorter procedural duration with the implications this may represent, including lower radiation doses, shorter requirement of anesthesia, and better time efficiency in the use of angio suites. However, these factors were not evaluated in this study, and may warrant further investigation.
Limitations of our study include the fact that prices reflect only those available to our institution at the time of the analysis. While pricing structures reflect prevailing pricing strategies by vendors, the precise numbers and relationships may vary should pricing strategies change or price negotiations occur. While the cost/volume data are specific to one institution, we have constructed a datasheet for coils available at our institution that allows us to assess price fluctuations in the coils and their cost/volume characteristics. Replacing our institutional pricing values with another would provide easy referencing for coil cost/volume efficiency.
Furthermore, one key assumption made throughout this analysis has been that the required volume of coil implanted is proportional to the volume of the aneurysm. This assumption was based on previous studies that found packing density thresholds to relate to stable occlusion and outcomes.3 However, factors governing stable coil embolization and aneurysm occlusion are not completely understood. Flow diverting devices, such as the pipeline flow diverter stent, have recently shown good outcomes,8 and suggest that packing density may not be the most important endpoint. Other metrics, such as the porosity ratio at the inflow zone of the aneurysm, may prove to be better predictors of outcome and endpoints for therapy. With this alternative treatment paradigm, cost per volume would not be representative. However, in intrasaccular treatment paradigms, packing volume will likely remain one factor among many in predicting treatment stability.
Finally, this approach in the assessment of hybrid coils, such as implants including hydrogels, is limited. Volume of gel coils was assessed to be that at maximum theoretical expansion, which may not be achieved in every case. Furthermore, one of the key potential benefits of hydrogel may relate to biological reactions to the gel9 and may factor into reduced recurrence rates, as seen in the HELPS trial.10
Conclusion
The difference in coil costs as a function of cost per volume of coil is enormous. While the biomechanical aspects of a given coil must justify their use, cost efficiency considerations may also present in an operator's mind during coil selection. For instance, if two coils have an equivalent sum of benefits and drawbacks in a given clinical situation, the less expensive might be reasonably chosen.
Using the currently available pricing algorithms, it is uniformly more cost efficient to use the longest available coil length for any given coil system and coil diameter that will fit in a given aneurysm volume. Using the longest coils which will fill a larger volume, compared with shorter coils, translates to a lower number of coils being required, leading to lower procedural costs. In an era of increasing cost awareness, such modeling will help operators control costs.
References
Footnotes
Contributors FKH: conceived and designed the research, acquired the data, and made critical revisions to the manuscript. CW: acquired the data, analyzed and interpreted the data, performed the statistical analysis, drafted the manuscript, and made critical revisions to the manuscript. ECC: drafted the manuscript. All authors approved the final manuscript.
Competing interests FKH has ownership in Blockade Stock.
Provenance and peer review Not commissioned; externally peer reviewed.