Article Text

Abstract
Background Acute ischemic stroke (AIS) due to emergent large-vessel occlusion (ELVO) has a poor prognosis.
Objective To examine the hypothesis that a better collateral score on pretreatment CT angiography (CTA) would correlate with a smaller final infarct volume and a more favorable clinical outcome after endovascular therapy (EVT).
Methods A retrospective chart review of the University of Tennessee AIS database from February 2011 to February 2013 was conducted. All patients with CTA-proven LVO treated with EVT were included. Recanalization after EVT was defined by Thrombolysis in Cerebral Infarction (TICI) score ≥2. Favorable outcome was assessed as a modified Rankin Score ≤3.
Results Fifty patients with ELVO were studied. The mean National Institutes of Health Stroke Scale score was 17 (2–27) and 38 of the patients (76%) received intravenous tissue plasminogen activator. The recanalization rate for EVT was 86.6%. Good clinical outcome was achieved in 32% of patients. Univariate predictors of good outcome included good collateral scores (CS) on presenting CTA (p=0.043) and successful recanalization (p=0.02). Multivariate analysis confirmed both good CS (p=0.024) and successful recanalization (p=0.009) as predictors of favorable outcome. Applying results of the multivariate analysis to our cohort we were able to determine the likelihood of good clinical outcome as well as predictors of smaller final infarct volume after successful recanalization.
Conclusions Good CS predict smaller infarct volumes and better clinical outcome in patients recanalized with EVT. These data support the use of this technique in selecting patients for EVT. Poor CS should be considered as an exclusion criterion for EVT as patients with poor CS have poor clinical outcomes despite recanalization.
- CT Angiography
- Stroke
Statistics from Altmetric.com
Introduction
Acute ischemic stroke (AIS) due to emergent large-vessel occlusion (ELVO) in the intracranial circulation has a poor natural history and results in high morbidity and mortality without successful revascularization.1 Treatment of AIS with intravenous tissue plasminogen activator (IV tPA) has been shown to improve outcome, yet there is a low rate of recanalization in patients with LVO.2 Endovascular treatment (EVT) with the newest generation of stent-retrieval devices has resulted in significantly higher rates of recanalization.3 ,4 Recent randomized clinical trials have shown that the higher recanalization rates achieved with EVT compared with IV tPA result in better outcomes with the former.1 ,5–9 However, the rate of good outcomes varied widely in these clinical trials from 32.6 to 71.0%.1 ,8 ,9
Studies suggest that the volume of core infarct at presentation observed by diffusion-weighted imaging is the strongest and most reliable predictor of outcome and response to IV tPA and EVT.10–12 The size of the final infarct and growth of the penumbra are also influenced by the extent of leptomeningeal collaterals.13 CT angiography (CTA) can be used to identify collaterals and has also been shown to predict outcome in patients who receive IV tPA and may improve the degree of recanalization with EVT.14
We hypothesized that patients with good leptomeningeal collaterals seen on CTA would have smaller infarct volumes and better clinical outcome after successful mechanical revascularization.
Methods
This study is a retrospective chart review of the University of Tennessee Health Science Center acute ischemic stroke database from February 2011 to February 2013, including consecutive patients who underwent EVT for the treatment of AIS due to LVO. The major inclusion criteria were the presence of LVO on pretreatment CTA and age >18 years. Baseline characteristics were gathered, including details of treatment, and determination of clinical outcome.
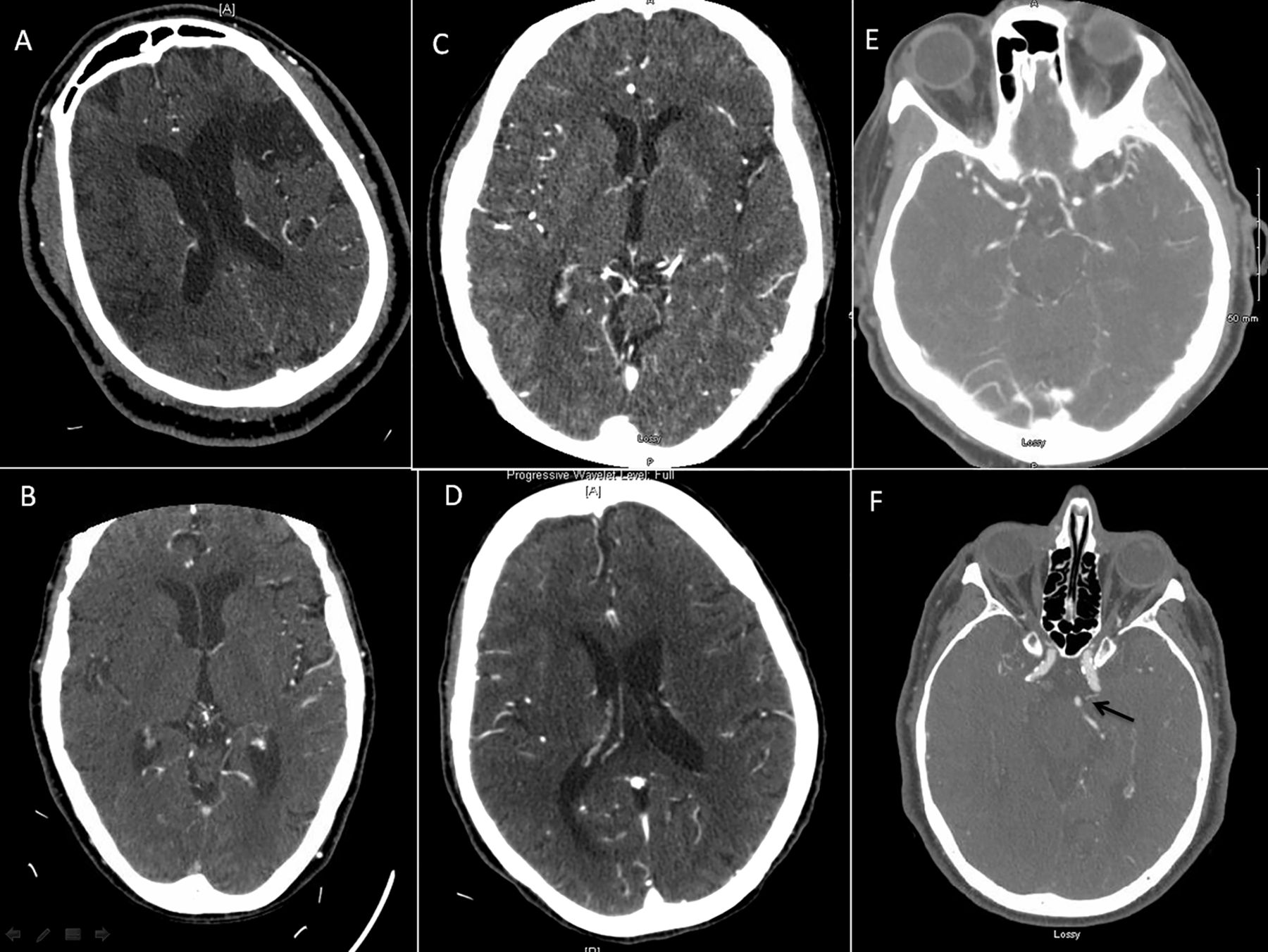
CT and CTA were performed on a 64-slice scanner. CT slice thickness was 1.25 mm with acquisitions in axial, sagittal, and coronal planes with 3D reformations. All diagnostic imaging was independently interpreted by two blinded neuroradiologists (MW, AFC). The CTA site of arterial occlusion and the CTA collateral scores (CS) were recorded. CS for the anterior circulation were reported in a dichotomized fashion (ie, poor vs good) using a methodology that has been shown to predict clinical outcome in the setting of IV tPA. This technique uses standard injection rates and acquisition parameters for CTA of the head and neck that are obtained identically to those for imaging the craniocerebral vasculature in the setting of AIS (figure 1).14 Patients with vertebrobasilar occlusion were assigned a good collateral score, if two posterior communicating arteries were seen on the CTA and the occlusion did not involve the top of the basilar artery. The neuroradiologists also calculated the final infarct volume using the ABC/2 method of volume calculation based on 12–24 h MRI, diffusion-weighted imaging, or last follow-up CT, if MRI was not available.15 According to the institutional protocol, the site of arterial occlusion, angiographic collateral score (ie, the Acute Stroke Therapy by Inhibition of Neutrophils—or ASTIN—method), and degree of recanalization (ie, the Thrombolysis in Cerebral Infarction—or TICI—score) were recorded prospectively in the stroke database at the time of treatment by the interventional team.16

CT angiography (CTA) collateral score (CS). (A) CTA image from a patient in late 50s with a right middle cerebral artery (MCA) M1 occlusion with no vascular markings apparent in the entire occluded MCA territory consistent with CS of 0. (B) Patient in early 80s with right MCA M1 occlusion with vascular markings apparent in <50% but >0% of the occluded MCA territory consistent with CS of 1. (C) Patient in mid-50s with a left MCA M1 occlusion with collaterals in >50% but <100% of the occluded MCA territory consistent with CS of 2. (D) Patient in late 70s with a right MCA M1 occlusion with almost complete reconstitution of the entire MCA territory (100%) consistent with CS of 3. For the purpose of study, collaterals were reported in a dichotomized fashion—poor (CS=0) versus good (CS=1, 2, and 3). (E). Patient in mid-to-late 60s with basilar occlusion, good collaterals, and two large posterior communicating arteries. (F) Patient in mid-60s with basilar occlusion and poor posterior circulation collaterals with one small posterior communicating artery visualized on the left (black arrow).
The primary clinical outcome was the modified Rankin scale (mRS) score at discharge. According to institutional protocol the mRS was reported prospectively on the physical therapy progress notes and abstracted by the investigators. A mRS of ≤3 was considered a favorable outcome at discharge. Final infarct volume was recorded as a secondary outcome.
Univariate predictors of outcome were determined with χ2 and Student t tests. Stepwise multivariate regression analysis (MVR) was performed to determine predictors of outcome. The results of our MVR analysis were then used to estimate the likelihood of a good clinical outcome based on the individual characteristics of the patient's clinical situation and treatment course. Statistical analysis was performed using STATA SE/13.0 software (College Station, Texas, USA).
Because our study was a retrospective study using data from a prospective clinical stroke registry, the grading of clinical outcomes and the degree of recanalization were not blinded, which might have led to selection bias. We attempted to address this by blinding the neuroradiologists—who were not involved in the care of the patients—when they determined the CS and final infarct volume.
Institutional investigation review board approval for this study was granted based on the prospectively maintained University of Tennessee Health Sciences Center acute ischemic stroke database (10-01003-XP).
Results
A total of 50 patients who met the inclusion criteria were treated during the study period. The mean patient age was 64.6 years and the mean National Institutes of Health Stroke Scale (NIHSS) score was 17 (range 2–27). The majority of patients were treated with IV tPA (76.0%) and with third-generation thrombectomy devices (90%), defined as a stentriever and/or direct aspiration via a large-bore (≥5 Fr) intracranial reperfusion catheter. The most common sites of arterial occlusion were the middle cerebral artery (M1) (50%), middle cerebral artery (M2) (10%), internal carotid artery (30%), and basilar artery 5 (10%). Good CS were observed in 38/50 (76%) patients. A comparison of patients with good CS and those with poor CS showed no significant differences in their baseline characteristics (table 1). The overall rate of TICI ≥2 recanalization was 86.6%.
Baseline characteristics of patients with good collateral score versus poor collateral scores
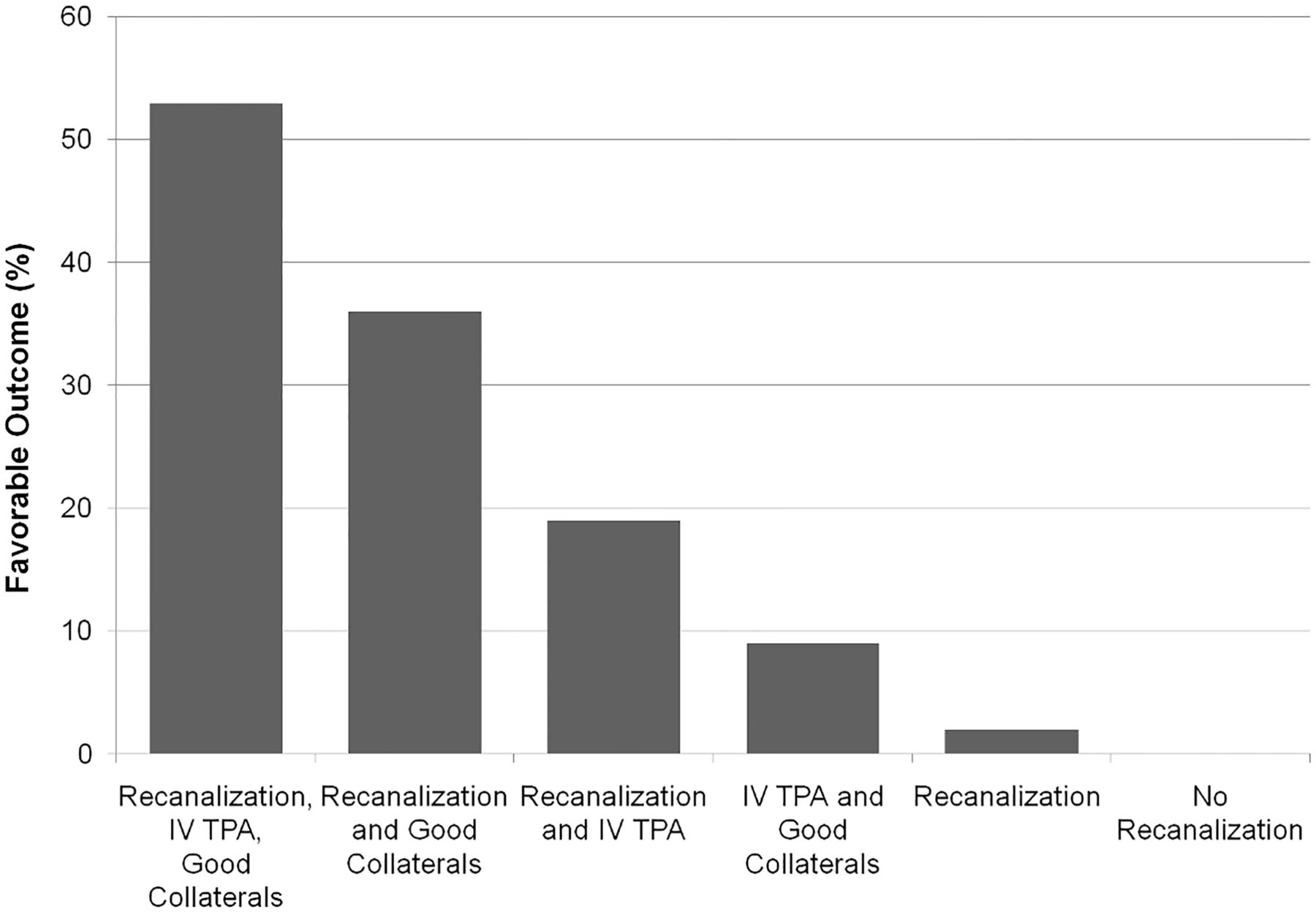
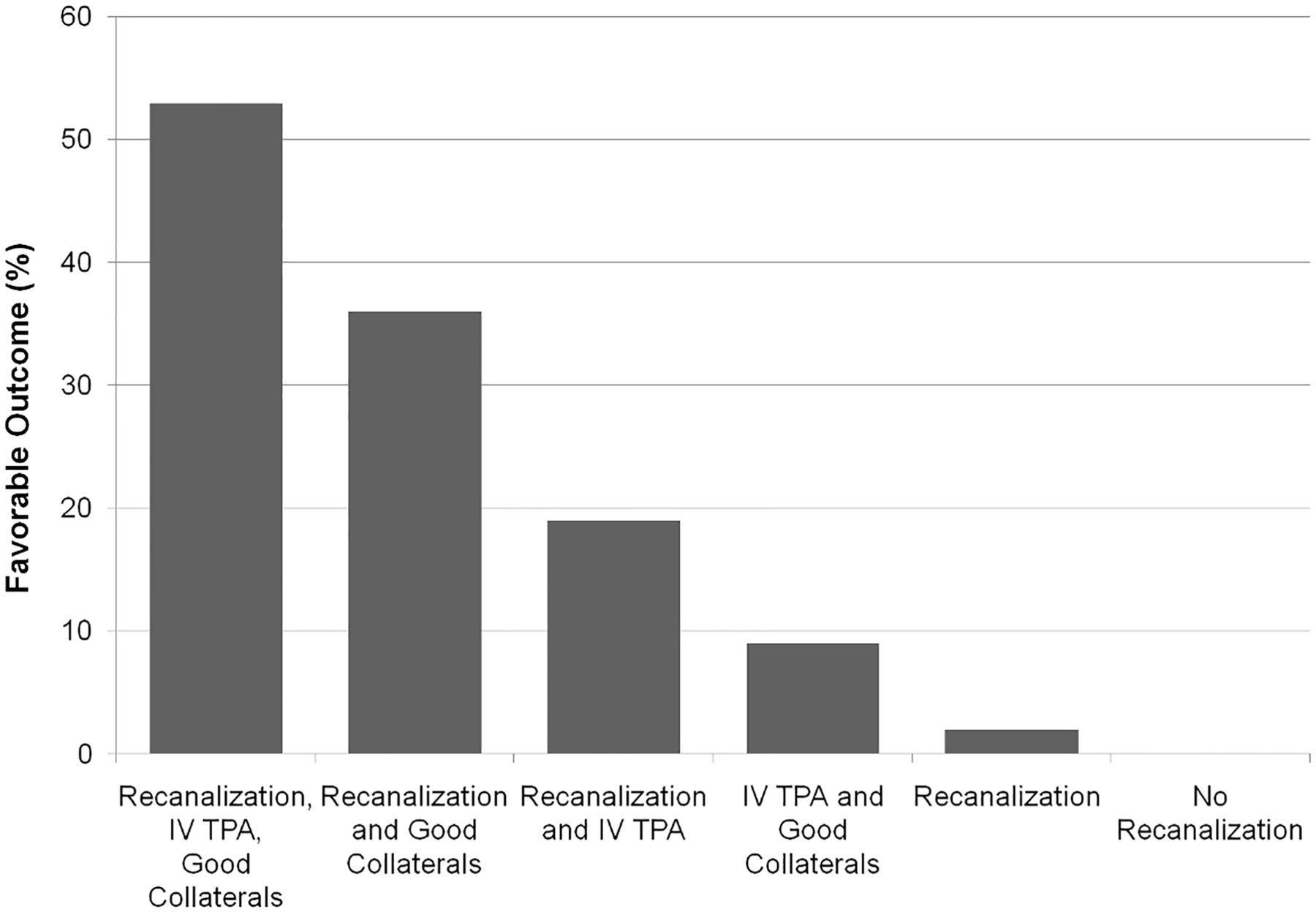
Univariate analysis showed that successful recanalization (p=0.02) and the presence of a good CS (p=0.043) both predicted favorable discharge outcome. There was a lower final infarct volume in patients who had good collaterals (106 vs 174.4 ml, p=0.08). Multivariate analysis showed good CS (p=0.024) and successful recanalization (p=0.009) to be predictors of favorable outcome. Additional multivariate analysis of the final infarct volume emphasized the importance of collaterals in patients who had revascularization, demonstrating a significantly lower final infarct volume in the group with good CS (p=0.001). Patients with higher systolic blood pressure on presentation had significantly higher final infarct volumes despite successful revascularization (p<0.0001). The predictors of good outcome from the multivariate analysis and the use of IV tPA were then used to predict the likelihood of a good outcome. The highest percentage of good clinical outcomes (52.7%) was seen when a patient was treated with IV tPA, had good CS, and successful recanalization. The absence of one of these three favorable clinical characteristics progressively reduced the rate of good outcome, with a good clinical outcome of only 2.0% seen in patients who had recanalization with poor CS and without IV tPA administration (figure 2).
{kind=link}
{kind=link}
Rates of good clinical outcome as determined by collateral score, recanalization, and intravenous tissue plasminogen activator (IV tPA) administration.
Discussion
This study shows that a good CS predicts both a favorable clinical response and decreased final infarct volume in patients with ELVO treated with mechanical embolectomy. The best imaging selection strategy for patients with ELVO remains unresolved with contradictory results that expose the limitations of CT and MR perfusion. Results of the DEFUSE 2 prospective registry suggested that MRI perfusion (MRP) could be used to predict favorable response to EVT, with good outcome in patients with a favorable ‘target mismatch’ MRP profile.12 However, a similar MRP protocol in MR RESCUE, a randomized clinical trial, failed to corroborate this hypothesis.6 The MR CLEAN trial did demonstrate the superiority of EVT compared with IV thrombolysis alone; however, only 32.6% of patients achieved a favorable clinical outcome.1 There was no prespecified multimodal imaging patient selection criteria in the trial, therefore it is encouraging to see that both ESCAPE and EXTEND-IA did have higher rates of good outcomes (53% and 71% mRS 0–2) than MR CLEAN using CTA collaterals and perfusion CT to select patients.8 ,9 Although our study was not a randomized controlled trial, it does provide unique information about collaterals compared with ESCAPE and other trials using multimodal imaging selection because our cohort of patients were all treated. Therefore, information about outcomes in patients with unfavorable imaging profiles as determined by CS can be evaluated.
The result from the predictive model in our study shows that patients with poor CS have only 2% good outcomes despite revascularization. Owing to the high cost and potential risk of these procedures, identifying this subgroup is as important as finding salvageable patients. Furthermore, revascularization of patients with poor CS may result in significant harm with higher infarct volume, increased malignant brain edema, and higher rates of intracerebral hemorrhage as seen in MRI studies.17 We could not draw any conclusions about this owing to the small number of patients in our study. Additionally, the low rate of symptomatic intracerebral hemorrhage (2.0%) and improved outcomes in patients receiving IV tPA adds further data to support the safety and efficacy of bridging therapy, particularly in the group of patients with good CS. The multivariate analysis also showed that patients with higher presenting systolic blood pressure fared worse despite good CS. This significance of this finding is unclear, but it may suggest that these patients are unhealthier or that acutely raised systolic blood pressure is a marker of a large volume infarction or intense ischemia.
A recent study by Nambiar et al18 showed similar results with statistically significant improved outcome (70% mRS ≤2 at 90 days) in patients with EVT with intermediate to good CTA collaterals based on the regional leptomeningeal collateral score from pretreatment CTA. The higher rates of good outcome reported by Nambiar et al may be attributed to several factors, including 90-day outcomes, differences in the definition of successful recanalization (TICI ≥2 in our study and TICI ≥2b in the study of Nambiar et al), the inclusion of patients with basilar occlusion in our study, and the overall higher presenting NIHSS in our cohort (ie, 17 vs 14). Despite these differences, the similar results reinforce the importance of collateral status as a potential patient selection tool.
This study has several important limitations. As mentioned above, this was a retrospective study using data from a prospective clinical stroke registry. Therefore, the grading of clinical outcomes and the degree of recanalization was not blinded. In contrast, the CS and final infarct volume determinations were obtained by blinded neuroradiologists who were not involved in the care of the patients. The final infarct volume was not evaluated on the same day of illness in all patients, and some patients received follow-up imaging with MRI and others with CT. Additionally, infarct volume data were not available for all patients as routine imaging was not mandated. We believe this might have led to an overestimation of final infarct volumes given the propensity to image sicker patients who did not fail to recanalize or who did not have clinical improvement after recanalization.
Rapid and reproducible imaging is essential to modern AIS care. This study adds to the growing body of reports that supports the use of CTA collaterals independent of perfusion imaging as a rapid and accurate method assisting in patient selection for EVT.
Acknowledgments
The authors thank Andrew J Gienapp (Department of Medical Education, Methodist University Hospital, Memphis, Tennessee and Department of Neurosurgery, University of Tennessee Health Science Center, Memphis, Tennessee) for technical and copy editing, preparation of the manuscript and figures for publishing, and publication assistance with this manuscript.
References
Footnotes
Twitter Follow Asim Choudhri at @AsimChoudhriMD
Contributors All authors of this work met International Committee of Medical Journal Editors criteria for authorship and made substantial contributions to the conception and design, acquisition of data, analysis and interpretation of data, drafting, critical revision, and final approval of this manuscript.
Competing interests LE has served as a consultant for Stryker Neurovascular, Microvention, and Codman Neurovascular. DH has served as a consultant for Covidien. ASA served as a consultant for Covidien, Johnson and Johnson, Siemens, Stryker, and Terumo; and received grants from Siemens and Terumo.
Ethics approval University of Tennessee Health Sciences Center acute ischemic stroke database (10-01003-XP).
Provenance and peer review Not commissioned; externally peer reviewed.