Article Text

Abstract
Background Rapid recanalization of occluded vessels is crucial for good clinical outcome in acute ischemic stroke. Endovascular treatment is usually performed via a transfemoral approach, but catheterization of the carotid arteries can be problematic in cases of difficult anatomy or vascular pathologies in some cases.
Objective To describe our experience with a technique involving surgical access to the carotid artery and consecutive transcarotid endovascular thrombectomy in patients with acute stroke.
Methods In a retrospective review of a prospectively maintained registry we identified 6 patients who underwent acute endovascular thrombectomy via a surgical access to the carotid artery.
Results Admission National Institute of Health Stroke Scale (NIHSS) ranged from 7 to 23. Intracranial recanalization (thrombolysis in cerebral infarction, TICI≥2b) was achieved in all patients (100%). Recanalization was achieved within 19±5 min after establishing carotid access. One patient developed a small neck hematoma, which was surgically removed without complications. No complications related to endovascular therapy were seen. At 3 months’ follow-up, five patients had survived. Three patients (50%) had regained excellent neurological function (modified Rankin Scale, mRS 0–1).
Conclusions Surgical carotid access for endovascular stroke treatment is feasible, with considerable advantages, in patients with expected problematic access or for whom transfemoral endovascular carotid access has failed.
- Thrombectomy
- Stroke
- Intervention
- Embolic
- Catheter
Statistics from Altmetric.com
Introduction
Endovascular thrombectomy aims to become the preferred treatment modality for acute ischemic stroke caused by occlusion of large cerebral arteries, especially in patients with high clot burden or with a contraindication for intravenous thrombolysis.1–3 Rapid recanalization of occluded vessels is crucial for good clinical outcome.4 In the majority of cases, access to the carotid artery can be achieved via femoral puncture and catheterization of the aortic arch within minutes. However, there are anatomical circumstances where this approach is very time-consuming, or may even prove to be impossible, thereby significantly affecting clinical outcome.4–7 Alternative methods for access to the carotid artery are therefore required. In this report we describe our experience with a technique involving surgical access, so called ‘cutdown’, to the carotid artery and consecutive transcarotid endovascular thrombectomy in patients with acute stroke.
Methods
Standard in-house procedure
Patients with acute ischemic stroke admitted to our institution are treated by either intravenous recombinant tissue plasminogen activator (rtPA) administration, a combination of intravenous rtPA administration and endovascular treatment, or endovascular treatment alone. Usually, in patients admitted later than 4.5 h after onset of symptoms, or with unknown onset, only endovascular treatment is considered if cross-sectional and perfusion imaging reveal sufficient tissue at risk. Individual treatment decision is an interdisciplinary process involving senior vascular neurologists and interventional neuroradiologists. Decision-making is based on clinical criteria (National Institute of Health Stroke Scale (NIHSS) >6 and NIHSS <6 in the presence of aphasia), the results of initial CT studies, and the absence or presence of contraindications for any of the above-mentioned procedures. Initial CT studies in patients with acute ischemic stroke comprise unenhanced cranial CT, CT angiography (CTA), and perfusion CT. Endovascular thrombectomy is considered when there is an occlusion of large arteries: the internal carotid artery (ICA), M1 and M2 segments of the middle cerebral artery, A1 segments of the anterior cerebral artery, basilar artery, and P1 segments of the posterior cerebral artery.
Clinical and radiological data of all patients selected for endovascular stroke therapy are prospectively entered into an in-house stroke registry of our institution.
Patient selection
In a retrospective analysis, we identified 223 patients with acute stroke in the anterior circulation who were treated by endovascular thrombectomy between June 2012 and September 2014. In nine of these cases (4%), access to the carotid artery via femoral puncture and catheterization of the aortic arch proved to be impossible, or was stopped because it took longer than 45 min. The reasons were as follows: catheterization of the abdominal aorta was impossible in two cases, recent surgery of the aortic arch and chronic occlusion of the common carotid artery (CCA) in one case, and massive elongation of aortic arch and supra-aortic vessels in six cases. In these nine cases, direct access to the carotid artery was considered as treatment of last resort, and a vascular surgery team was called to the angiography suite. In the first four cases, percutaneous puncture of the carotid artery was attempted first. This was successful in three cases. In the fourth patient, puncture resulted in dissection of the CCA, and treatment was continued by switching to surgical access. In the last five cases, surgical access to the carotid artery was performed without a prior attempt of percutaneous puncture.
This report describes the result of six consecutive patients, in whom we performed a combined surgical and endovascular thrombectomy involving (1) surgical access to the carotid artery, (2) endovascular thrombectomy, and (3) surgical closure of the operation site.
Surgical procedures
Surgical access to the carotid artery was provided by a vascular surgeon as follows: to gain access to the carotid artery, the patient's neck is slightly rotated to the opposite side and a 5–6 cm long incision is made along the anterior border of the sternocleidomastoid muscle. After intravenous administration of 5000 IU of heparin, the deep jugular vein is lateralized and the carotid bifurcation is exposed while giving careful attention to the vagal and hypoglossal nerves. Hereupon, the common, internal, and external carotid arteries are marked with vessel loops. After cannulation of the CCA with a standard 19-gauge needle, an 8F or 6F sheath with a length of 10 cm (Optimed, Ettlingen, Germany) is carefully placed into the CCA with the use of a 0.035 inch standard angled Radifocus guidewire (Terumo, Tokyo, Japan). The larger sheath is placed whenever possible, in order to increase the efficacy of aspiration. Finally, after visualization of the carotid bifurcation with angiography, the sheath is placed into the ICA over the guidewire under fluoroscopic control. If immediate placement of the sheath is not possible owing to a high-grade carotid stenosis, eversion carotid endarterectomy (eCEA) is performed before further neuroradiological endovascular treatment. When the endovascular intervention is finished the vascular surgeon removes the sheath, closes the puncture site with a purse-string suture, and closes the operation site after placement of a Redon drain.
Endovascular procedures
Neurointerventional stroke treatment in our institution is performed under general anesthesia by interventional neuroradiologists. The basic steps of the intervention are as follows: the neuroradiologist places a long sheath or balloon catheter in the carotid artery via a femoral access. If the femoral arteries cannot be catheterized, or transaortic access is not feasible, brachial access is chosen. First, distal aspiration thrombectomy is performed, if the occlusion site is accessible, with a distal aspiration catheter (eg, Sofia, Microvention, Tustin, USA; DAC, Stryker Neurovascular, Fremont, USA; Navien, Covidien, Irvine, USA). If aspiration thrombectomy does not achieve full recanalization, mechanical thrombectomy with a stent retriever is performed (eg, Trevo ProVue, Stryker Neurovascular, Fremont, USA; ReVive, Codman Neurovascular, Raynham, USA). The thrombus is passed with a microcatheter through which a stent retriever is placed and expanded within the thrombus. The stent retriever is then slowly withdrawn after an incubation period of 3–5 min. Manual aspiration and an aspiration pump (Penumbra, Alameda, USA) provide constant aspiration through the sheath and distal aspiration catheter during retrieval. Carotid artery stenting (CAS) is performed with a self-expanding stent (Carotid Wallstent, Boston Scientific, Natick, USA) under administration of a glycoprotein IIb/IIIa inhibitor (Tirofiban), if necessary to gain access to the occlusion site.
Results
All six patients presented with tortuous carotid vessels and carotid stenosis. In four patients, eCEA was performed in addition to the endovascular treatment (table 1). Three of these eCEA were performed before interventional thrombectomy, since passage of the carotid artery was impossible otherwise. Mean (±SD) overall procedure time (from end of CT imaging until recanalization) was 148±52 min. Mean duration of carotid cutdown (from the beginning of surgical procedures to the first DSA imaging via carotid access) was 42±19 min.
Provides an overview of clinical and procedural data of all patients
Admission NIHSS ranged from 7 to 23. Intracranial recanalization (thrombolysis in cerebral infarction, TICI≥2b) was achieved in all cases (100%).8 Recanalization was achieved within 20±4 min (mean± SD) after establishing carotid access. In five cases, stent retrievers were used. In one case recanalization was achieved by direct aspiration only. Three patients had received IV lysis using rtPA between CT imaging and endovascular treatment. Three patients were recanalyzed by endovascular thrombectomy only.
One patient who was postoperatively treated with 500 mg aspirin and heparin (partial thromboplastin time 40–50 s) developed a small hematoma within the operation site owing to postoperative oozing (case 3). The hematoma was surgically removed without complications 5 days after surgery. No other access-related complications and no complications related to endovascular therapy were seen.
Clinical symptoms of five patients improved during follow-up. At 3 months’ follow-up, three patients (50%) had regained excellent neurological function (modified Rankin Scale, mRS 0–1). One patient died from sepsis after discharge (case 4).
Illustrative case
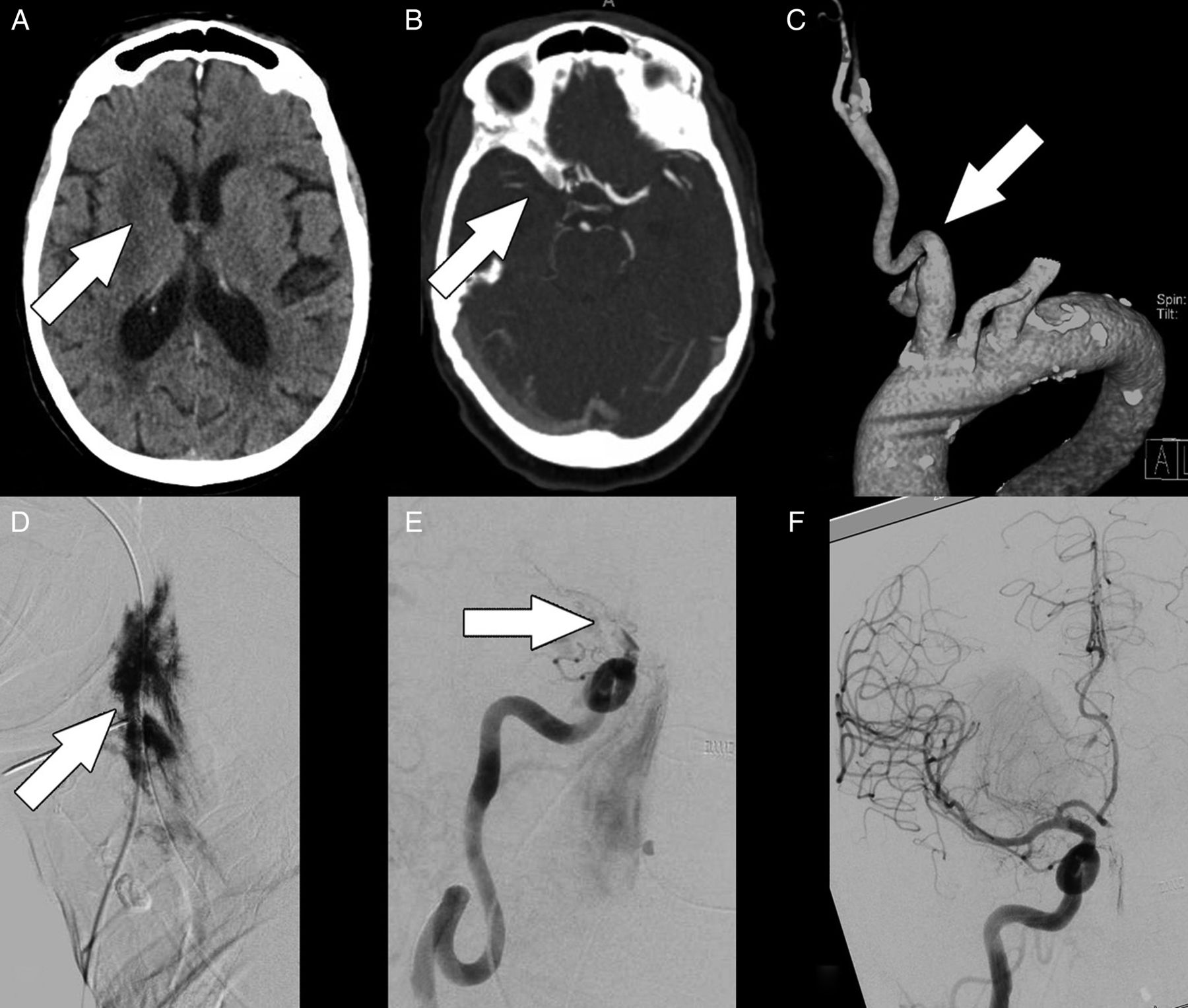
An elderly patient presented with wake-up stroke with a middle cerebral artery syndrome (NIHSS: 23 and mRS: 5). Cranial CT showed infarction of the right basal ganglia (figure 1). There was cortical mismatch in the territory of the right middle cerebral artery between cerebral blood flow and cerebral blood volume on perfusion CT, indicative of tissue at risk. CTA showed occlusion of the right carotid T and a high-grade stenosis of the right ICA. In addition, elongated supra-aortic vessels and a complicated aortic arch were noted. IV lysis was not applied because the time of symptom onset was unclear. Instead, a decision to carry out endovascular thrombectomy was made and the patient was transferred to the angiography suite. After intubation, access through the right-sided femoral artery was established. However, owing to the complex vascular anatomy, catheterization of the right-sided ICA proved impossible within 45 min, and direct percutaneous access to the carotid artery was considered instead. The vascular surgery team was informed and remained on standby for the rest of the procedure. Ultrasound-guided puncture of the CCA and insertion of a 4F sheath were successful, but replacement of the 4F sheath with a 6F sheath caused perforation of the calcified CCA with extravasation of contrast agent at the puncture site. The vascular surgery team immediately exposed the carotid artery and inserted an 8F sheath. Consecutive DSA procedures showed occlusion of the carotid T (TICI 0). Complete recanalization (TICI 3) was achieved within 23 min after two passes with a Trevo ProVue stent retriever device and distal aspiration through a DAC70 catheter. There were no procedural or postinterventional complications. Clinical symptoms improved considerably 3 months after discharge (mRS 4).
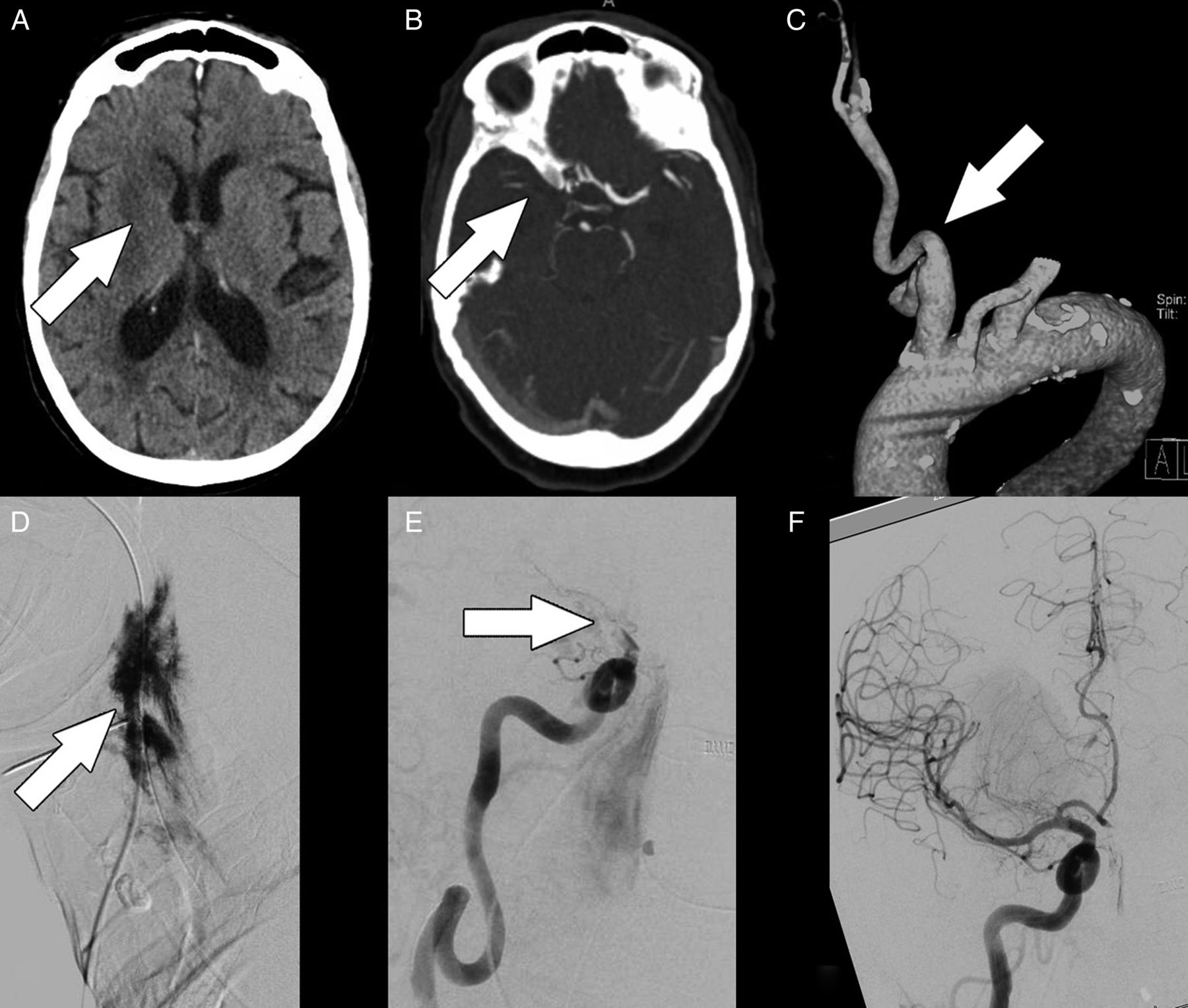
Elderly patient with a wake-up-stroke (case 1). There is infarction of the right basal ganglia on initial CT imaging (A: arrow). CT angiography (CTA) shows occlusion of the right carotid T (B: arrow). A three-dimensional reconstruction of CTA data (C) shows a complicated aortic arch with a proximal origin of the brachiocephalic artery and a tortuous common carotid artery (CCA) (C: arrow). After ultrasound-guided puncture of the CCA and insertion of a 4F sheath were successful, replacement of the 4F sheath with a 6F sheath caused perforation of the calcified CCA with extravasation of contrast agent at the puncture site (D: arrow). After surgical carotid access was established, DSA shows occlusion of the carotid T (thrombolysis in cerebral infarction, TICI 0) (E: arrow). Complete recanalization (TICI 3) was achieved after two passes with a Trevo ProVue device and distal aspiration through a DAC70 catheter (F).
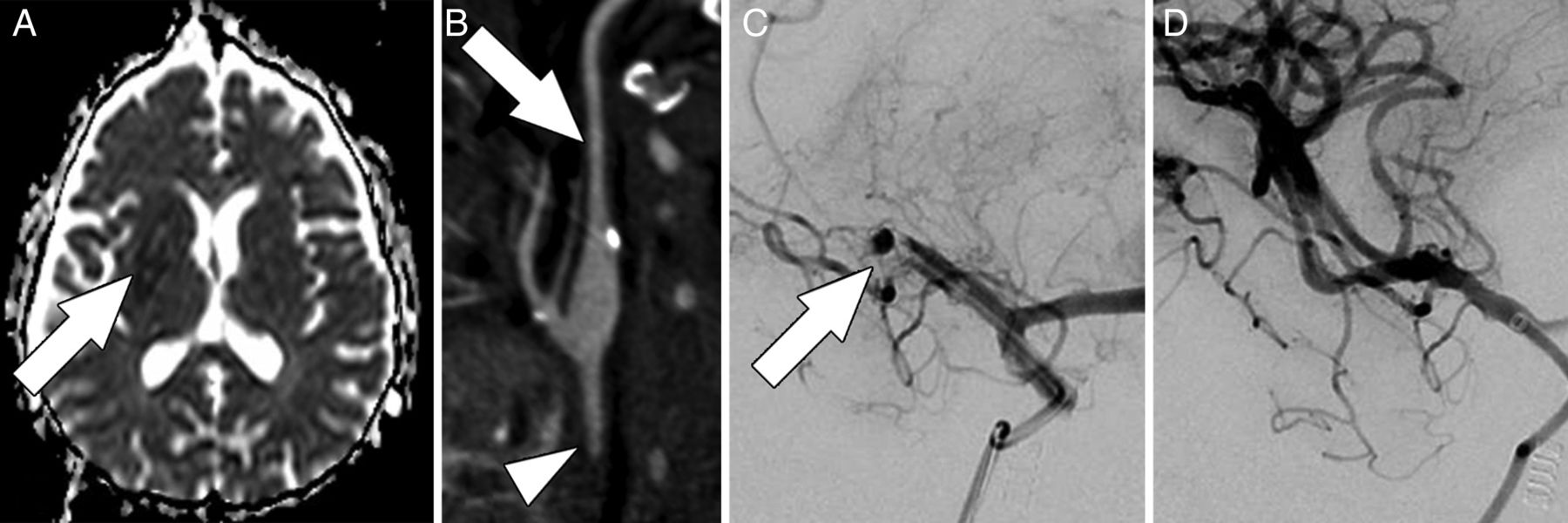
Figure 2 shows an illustrative case, in which carotid cutdown was the primary approach (figure 2).
{kind=link}
{kind=link}
Middle-aged patient who underwent surgery of the aortic arch after a Stanford type A dissection 2 weeks earlier and who presented with a fluctuating left-sided hemiparesis (case 2). There is infarction of the right basal ganglia on initial MRI (A: arrow). CT angiography (curved maximum intensity projection) shows a thin internal carotid artery (B: arrow), occlusion of the common carotid artery (CCA) (B: arrowhead), and occlusion of the distal middle cerebral artery. With regards to the recent surgery and under the assumption that CCA occlusion resulted from chronic CCA stenosis (thin internal carotid artery), an interdisciplinary consensus in favor of a primary carotid cutdown is established. After surgical carotid access was established, DSA shows occlusion of the distal middle cerebral artery and three of its branches (C: arrow) (thrombolysis in cerebral infarction, TICI 0). Complete recanalization (TICI 3) was achieved after two passes with a Trevo ProVue device and distal aspiration through a Navien catheter (D).
Discussion
The transfemoral approach is the most common approach for endovascular stroke treatment.6 ,9 Difficult anatomical situations or significant stenoses of cervical vessels, however, may be associated with prolonged times until catheterization of the target vessel, thereby negatively affecting clinical outcome.4–7 Jadhav et al6 reported that 20–90 min of procedural time were spent unsuccessfully while trying to access the occlusion site via the transfemoral approach before switching to percutaneous puncture of the carotid artery. Similarly, Ribo et al7 showed that failure of transfemoral catheterization occurred in up to 5% of patients and that this was associated with a delay of more than 30 min until vessel recanalization, thereby worsening clinical outcome. In cases where femoral puncture fails a transbrachial access route may be considered as well.10 However, there is an increased risk of arterial injury and postoperative arterial occlusion due to the smaller diameter of the brachial and radial arteries.11 Furthermore, smaller devices (ie, 6F sheath) are usually being used for transbrachial catheterization, which may reduce the efficacy of thrombectomy, unless distal access catheters with distal aspiration are used.12
Percutaneous carotid puncture
Difficult access routes due to complicated aortic arch anatomy and tortuous vessels may be circumvented by a direct carotid approach. Jadhav et al reported a series of seven cases and Mokin et al reported two cases in which a direct percutaneous carotid approach was used for subsequent endovascular stroke treatment, with favorable results.6 ,13 Carotid access was achieved within 9.6±3.6 min on average.6 Recanalization (≥TICI 2a) was attained in seven of nine patients within 25±14 min after achieving carotid access.6 ,13 Seven of eight patients for whom clinical outcomes were reported further improved during follow-up.6 ,13 Another advantage of a direct carotid approach is that the aortic arch does not need to be instrumented, thereby reducing the risk of embolization into other vascular territories.14 ,15 Overall, puncture of the carotid artery appears to be a valuable alternative whenever a transfemoral access route is impossible or may prolong procedure times.
Closure of the carotid puncture site remains an unsolved problem, as none of the available occlusion devices has been approved for carotid occlusion.6 ,9 Manual and bandage compression as used for the femoral arteries cannot be applied to the carotid artery. Carotid occlusion using the Angio-Seal device (St Jude Medical, St Paul, USA) has been reported in eight cases.13 ,16–18 Nevertheless, we would strongly discourage the use of the Angio-Seal device in the carotid artery, given that the absorbable intraluminal anchor may cause embolism. In one of two patients who received carotid closure via the StarClose device (Abbott Vascular, Abbott Park, USA) during acute stroke treatment a large cervical hematoma occurred.13 The authors suspected that the StarClose system became entangled with the platysma muscle, thereby reducing the system’s efficacy. In addition, Jadhav et al6 reported complications (one large hematoma and one pseudoaneurysm) in both cases of closure with the Mynx device (AccessClosure, Mountain View, USA), whereas no complications were seen when manual compression was applied. While some authors advocate manual compression of the carotid puncture site,6 ,16 ,19 ,20 other authors point out a considerable risk for cervical hematoma, especially when double platelet inhibition or aggressive heparin treatment is needed.9 ,15 ,21 Altogether, local puncture-related complications (dissections and local hematomas) after percutaneous carotid puncture have been reported in 2.4–10.7% of cases in large series.21
Surgical access
Surgical access to the carotid artery, also known as carotid cutdown, is the oldest technique for neurovascular catheterization.22 ,23 In the past two decades this almost forgotten access has been extensively used for CAS with operative flow reversal.24–28 Recently, Dorfer et al19 who treated eight patients with ruptured and unruptured cerebral aneurysms, cerebral arteriovenous malformations, and a carotid cavernous fistula via a surgical carotid access, reported no access-related complications. Larrazabal et al15 reported no access-related complications in three patients with coiling of intracranial aneurysms and one patient with retrograde placement of a stent in the CCA. Ross and Luzardo who reported having treated many patients described two uncomplicated illustrative cases with coiling of intracranial aneurysms.9 Samaniego et al29 reported on one patient who received an intracranial stent for stenosis of the middle carotid artery via surgical carotid access. In summary, data from the literature suggest that surgical carotid access in (semi-)elective settings is a safe technique: considering 1005 cases reported in the five largest series of the past 7 years, carotid dissection and cervical hematoma occurred in 0.8% (eight cases) and 1.9% (19 cases), respectively.24–28
The major disadvantage of direct surgical carotid access is its limited availability, especially for acute stroke. Optimization of workflow may considerably reduce procedure times. There was a subjective learning process, reflected in our last case, in which we needed a minimum of 27 min for carotid cutdown and 15 min for interventional treatment. Nevertheless, there is room for improvement, given that most of the time in our series was lost between the CT suite and the beginning of surgical procedures (table 1). Also, while carotid access was performed under general anesthesia in our series, conscious sedation, which is the preferred modality in some centers for endovascular stroke treatment, may also improve procedure times.1
Patient selection
Identification of patients who may benefit from primary surgical carotid access is important, since early and correct decision-making may help to significantly reduce times until thrombectomy and improve neurological prognosis. Ribo et al identified clinical factors associated with prolonged time to carotid access including: age >75 years, dyslipidaemia, hypertension, and affection of the left carotid circulation.7 Also, anatomical variants associated with technically challenging carotid access have been reported. Such variants include any of the following: bovine arch; type II and especially type III arch; tortuosity, severe angulation, or loops of the CCA; and CCA ostial stenosis.13 Taken together, it may be possible to predict cases with prolonged access times based on clinical and CTA findings.
Surgical access versus direct percutaneous puncture
Considering the advantages of a direct surgical approach, invasiveness may as well speak in favor of surgical carotid access. Papanagiotou et al30 reported that 6% (22 of 367) of patients who underwent endovascular stroke treatment required CAS to gain access to the intracranial occlusion site. If passage through a high-grade stenosis is not possible there is always the possibility of emergency eCEA. Thereby, the need for subsequent double platelet inhibition after CAS is eliminated, and the risk of hemorrhagic complications following successful revascularization is reduced. An invasive approach may also facilitate placement of the sheath: Mokin et al13 reported that percutaneous puncture of the carotid artery without sight resulted in perpendicular placement of the sheath into the carotid artery causing kinking of the sheath. In our series, percutaneous puncture of the carotid artery resulted in a small rupture at the puncture site with extravasation of contrast agent, when a smaller sheath was to be replaced with a larger one (case 1). Given the overall smaller risk of local complications compared with percutaneous puncture, various authors strongly recommended open exposure instead of transcutaneous puncture of the carotid artery in order to reduce the risk of vessel injuries, in particular when patients have vascular fragility such as Marfan disease or Ehlers–Danlos syndrome.9 ,13 In addition, postprocedural surgical closure of the access site is more effective than closure after percutaneous carotid puncture, allowing double platelet inhibition and more aggressive heparin treatment with a lower risk for hematomas.15 ,21 ,24–28
If surgical and endovascular procedures are properly interlinked, there are many arguments in favor of surgical carotid access when conventional approaches either fail or potentially prolong procedure times. Even though there is room for improvement, the results of our series are favorable: clinical symptoms improved considerably in five of six patients during follow-up and there was only one procedure-related complication—namely, a cervical hematoma that was caused by oozing in the operation site and which was removed by a second small surgical procedure. In summary, it is not rare that transfemoral access to the carotid artery is impossible or takes so long that the neurological outcome of patients scheduled for endovascular stroke treatment is negatively affected. Based on clinical and CTA data it may be possible to select these patients before the start of the interventional treatment. Surgical access to the carotid artery has been shown to be an effective alternative for these patients. Available data may justify selection of this as a secondary approach when transfemoral access has failed, or even as the primary approach in a carefully selected subset of patients with stroke. A priori selection of patients might then reduce procedural times considerably.
Conclusions
Surgical carotid access for endovascular stroke treatment is feasible, with considerable advantages in patients with expected problems of access or for whom transfemoral endovascular carotid access has failed.
References
Footnotes
Contributors Conception and design, acquisition of data, analysis and interpretation of data, drafting and critically revising the article: all authors.
Competing interests None declared.
Ethics approval The local ethics committee approved this study.
Provenance and peer review Not commissioned; externally peer reviewed.