Article Text

Abstract
Background Liquid embolic agents are the preferred embolic material in endovascular treatment of pial and brain arteriovenous malformations and dural arteriovenous fistulas (DAVFs). There is little choice available in interventional neuroradiology practice other than two of the most commonly used liquid embolic agents—n-butyl cyanoacrylate and the Onyx liquid embolic system (ev3 Neurovascular, Irvine, California, USA). PHIL (Precipitating Hydrophobic Injectable Liquid) (Microvention, Inc California, USA) is a new liquid embolic agent, CE marked and available for clinical use in Europe.
Objective To present our preliminary experience using PHIL in treating cranial and spinal DAVFs.
Methods Between September 2014 and January 2015, eight patients, with five cranial DAVFs and three spinal DAVFs were treated with PHIL as the sole embolic agent used with intent to cure. Clinical presentation, location of DAVF, Borden type, fluoroscopic time, radiation dose, procedural time, injecting microcatheter used, volume of PHIL injected, complications, immediate angiographic data, premorbid and discharge modified Rankin Scale score, and any neurologic deficits were included in the analysis.
Results Seven patients were successfully treated with complete angiographic exclusion of the fistula in a single sitting. Treatment failed in one patient where only suboptimal microcatheter positioning could be achieved and PHIL failed to penetrate the fistula's nidus. Venous penetration was achieved in all other patients except one with a small fistula, but with adequate fistula penetration by the embolic material. No other technical complication or neurologic deterioration occurred in any of the patients.
Conclusions PHIL liquid embolic agent appears to be an excellent alternative embolic material with certain advantages compared with other available liquid embolic agents. Further studies are required to fully evaluate its safety and efficacy.
- Fistula
- Liquid Embolic Material
- Intervention
Statistics from Altmetric.com
Introduction
Liquid embolic agents have been widely used in interventional neuroradiology for treating arteriovenous malformations and dural arteriovenous fistulas (DAVFs). n-Butyl cyanoacrylate (n-BCA), otherwise commonly referred to as glue, had been the sole liquid embolic agent available for use in these applications until the introduction of the Onyx liquid embolic system in 2005. Each of these agents has its merits, problems, and technical idiosyncrasies; in-depth comparison and discussion of these is beyond the aims of this article.
The new liquid embolic agent PHIL (Precipitating Hydrophobic Injectable Liquid) is a non-adhesive agent comprising a copolymer dissolved in dimethyl sulfoxide (DMSO). An iodine component is chemically bonded to the copolymer to provide radio-opacity for fluoroscopic visualization. The PHIL liquid embolic system consists of a sterile, prefilled, 1.0 mL syringe of PHIL liquid embolic agent, a sterile, prefilled 1.0 mL syringe of DMSO, and microcatheter hub adaptors. A DMSO-compatible delivery microcatheter that is indicated for use in the neurovascular or peripheral vasculature is used to access the embolization target site. PHIL is delivered by slow, controlled injection through the microcatheter into the vascular malformation under fluoroscopic control. The DMSO solvent dissipates into the blood, causing the copolymer to precipitate forming an embolus. PHIL polymerizes from the outside to the inside, while penetrating distally in the vascular lesion. Final solidification of the injected agent occurs within 5 min according to the manufacturer.
The potential perceived advantages of PHIL include good forward flow with less reflux, together with the capability for repeated injections allowing for controlled target embolization. Because PHIL is iodine based and chemically bonded to the copolymer, concern about tantalum sedimentation with potential for non-visualization of the embolic agent and non-target embolization is eliminated. PHIL, lacking tantalum, produces fewer artifacts on CT than Onyx. Other possible advantages considered were reduced fluoroscopy times and, consequently, reduced radiation doses. It was decided to use PHIL in our patients in view of these potential advantages with the option to use the more conventional embolic agents if warranted. We report our preliminary experience with PHIL in treating DAVFs.
Methods and materials
Eight patients with DAVFs, five cranial and three spinal, were treated in a single center by two individual operators between September 2014 and January 2015. Clinical, procedural, and angiographic data were retrospectively collected and subsequently analyzed. Clinical details collected included presenting symptoms, location of the DAVF, Borden type, in-patient stay duration, and premorbid and discharge modified Rankin Scale (mRS) score. The procedural details collected included fluoroscopic time, radiation dose, procedural time, volume of PHIL injected, microcatheter used, and tip detachment, if applicable. The procedure time was taken as the time difference between the first and last angiogram obtained.
Though PHIL is available in different formulations—namely, PHIL 25%, PHIL 30%, and PHIL 35%, only PHIL 25% was used in this series. All PHIL injections were done by a senior interventional neuroradiologists (SL or AT). None of the patients required injection of another embolic agent.
For two patients, one patient with a spinal DAVF and the other a cranial DAVF, diagnostic angiograms were obtained before embolization in a separate sitting. All procedures were done under general anesthesia. Diagnostic angiograms were also obtained under general anesthesia immediately before embolization in the cases with no previous angiograms. No antiplatelet therapy or anticoagulation was used during or after the procedures for the patients with cranial DAVFs. The patients with spinal DAVFs were prescribed prophylactic doses of low molecular weight heparin for 7 days after the procedure upon successful treatment.
The patients were assessed by the neurosurgical team after the procedure and evaluated before discharge for any new neurologic deficits. Differences between the premorbid and discharge mRS score and any new neurologic deficit were noted as a clinical outcome.
Results
Mean patient age was 58; three patients were female. Clinical presentation, location of DAVF, Borden type, inpatient stay duration, premorbid, and discharge mRS score are summarized in table 1. The procedure details collected are summarized in table 2. The cases are illustrated in figures 1⇓⇓⇓⇓⇓⇓–8.
Clinical features before and after the procedure
Procedural details
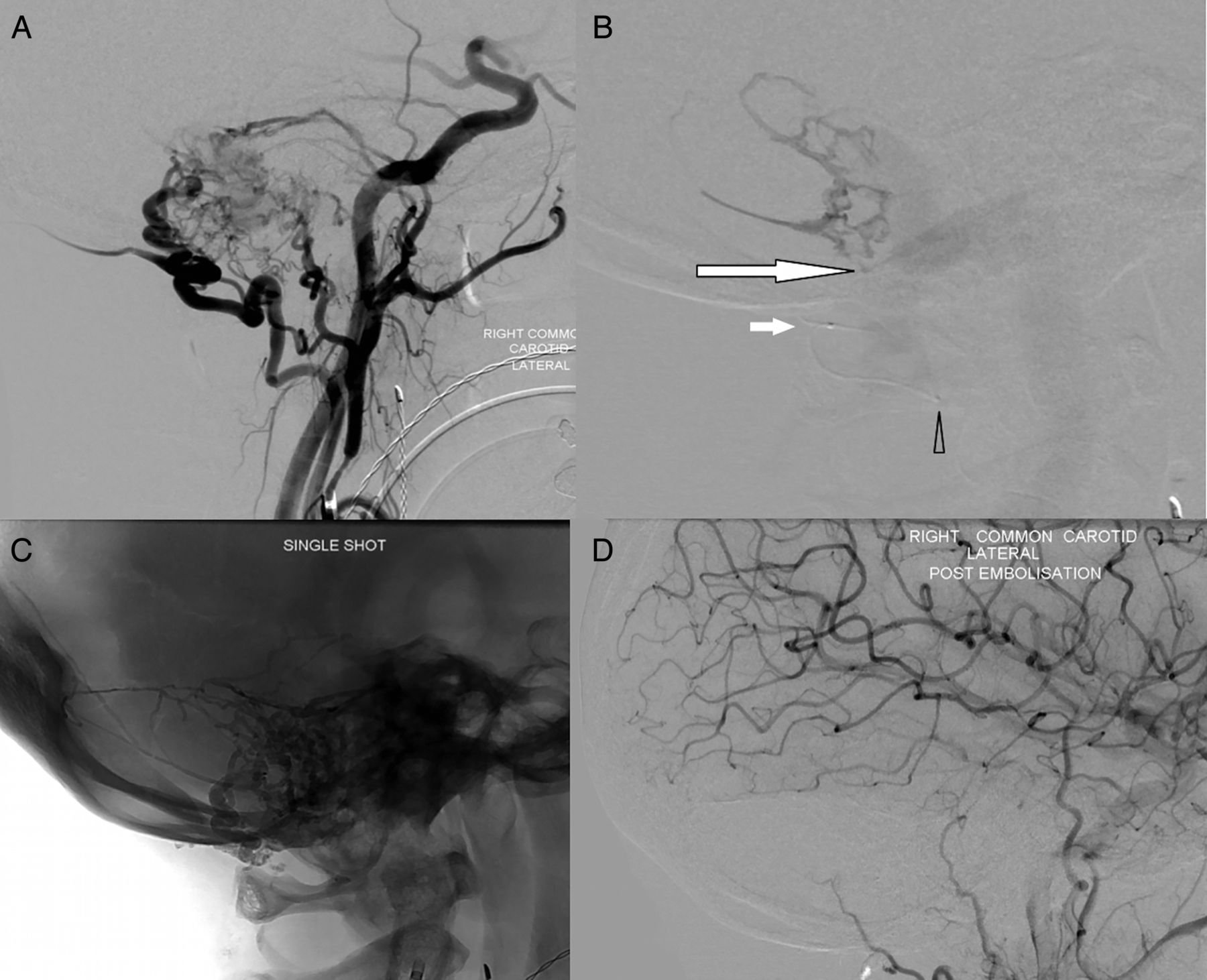
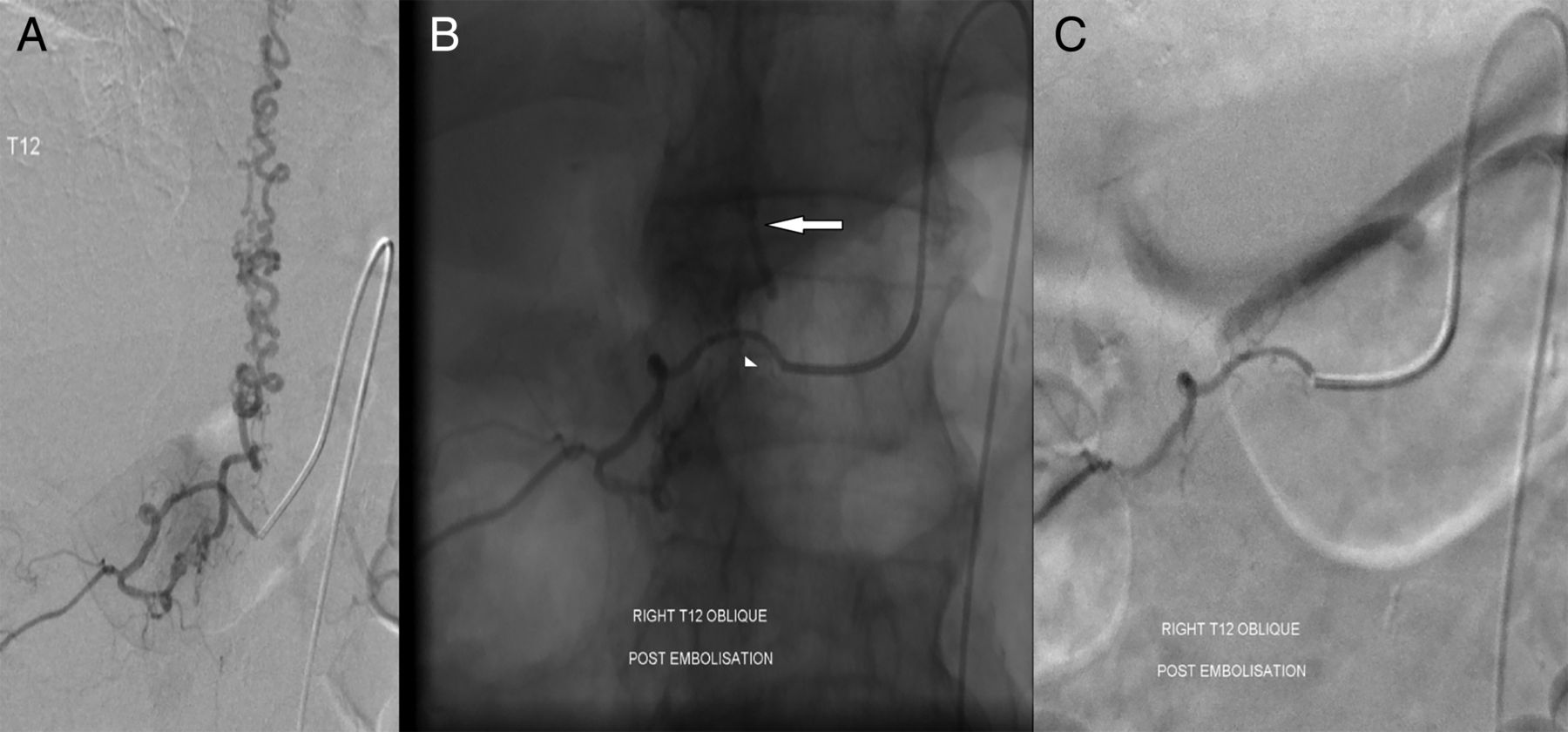
(A) Initial DSA showing the sigmoid dural arteriovenous fistula (DAVF) fed by branches of the occipital, posterior auricular, and middle meningeal arteries. (B) Selective run through the microcatheter showing distal position of the catheter tip (large white arrow), the detachable tip marker (smaller white arrow), and the guide catheter tip (black arrow head). (C) Plain single shot X-ray picture showing the cast of PHIL (Precipitating Hydrophobic Injectable Liquid) with retrograde filling of the posterior auricular feeders, middle meningeal feeders, and posterior meningeal feeder (not visualized on the carotid angiogram). (D) Late arterial phase common carotid DSA showing no residual DAVF.
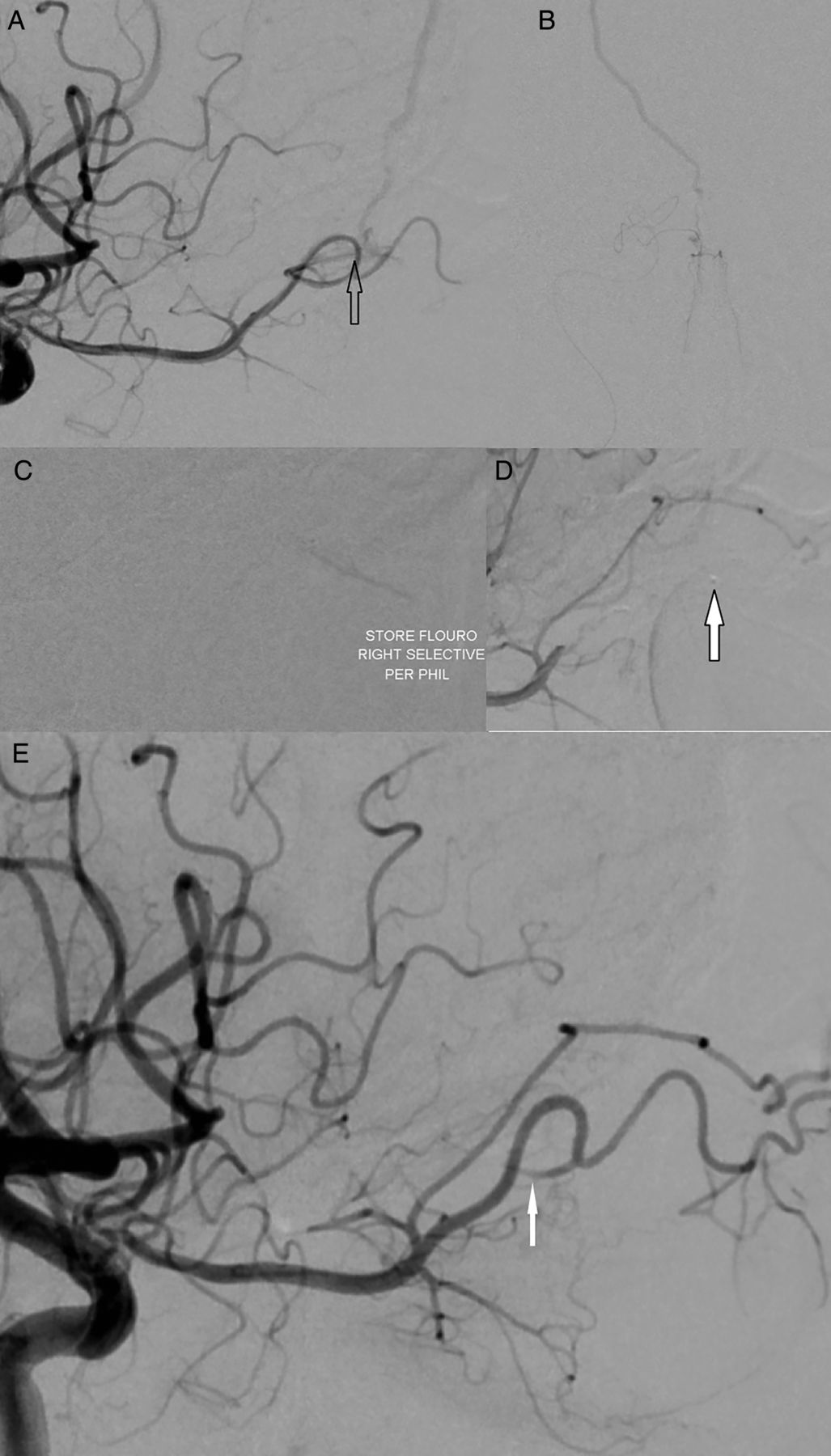
(A) Run through the internal carotid artery with the microcatheter in ethmoidal branch of the ophthalmic artery and microcatheter tip at the fistulous point (black arrow). (B) Selective run through the microcatheter confirming distal placement of the catheter tip with some antegrade filling of the nasal vessels (Townes view). (C) Fluoroscopic image during injection of PHIL (Precipitating Hydrophobic Injectable Liquid) with PHIL in the fistulous nidus. (D) Spasm and contrast stasis in the ophthalmic artery requiring microcatheter withdrawal. Microcatheter tip is shown by the white arrow. (E) Spasm had completely reversed upon withdrawal of the microcatheter with occlusion of the feeding branch (white arrow).

(A) Initial DSA showing a parietal dural arteriovenous fistula (DAVF) fed by the middle meningeal artery (MMA) and superficial temporal artery branches. (B) Selective run through the Scepter balloon in the MMA to exclude orbital supply. (C) Cast of PHIL (Precipitating Hydrophobic Injectable Liquid) in the draining vein, MMA, and other feeders filled in a retrograde manner. (D) Late arterial common run showing no residual DAVF.
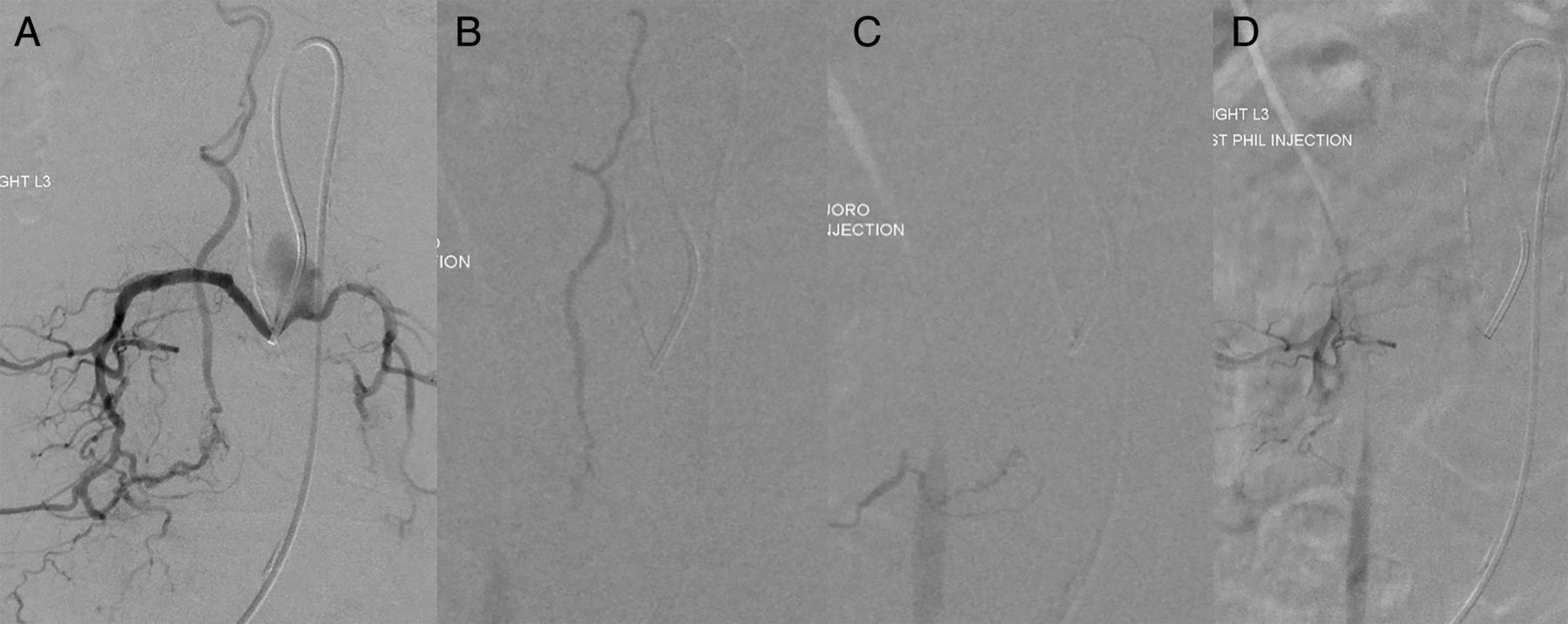
(A) Run through a 5 Fr catheter showing the spinal dural arteriovenous fistula (DAVF). (B) Injection of PHIL (Precipitating Hydrophobic Injectable Liquid) showing penetration of the draining vein. (C) Injection of PHIL showing penetration of the fistulous portion. (D) End of procedure run showing angiographic exclusion of the DAVF.

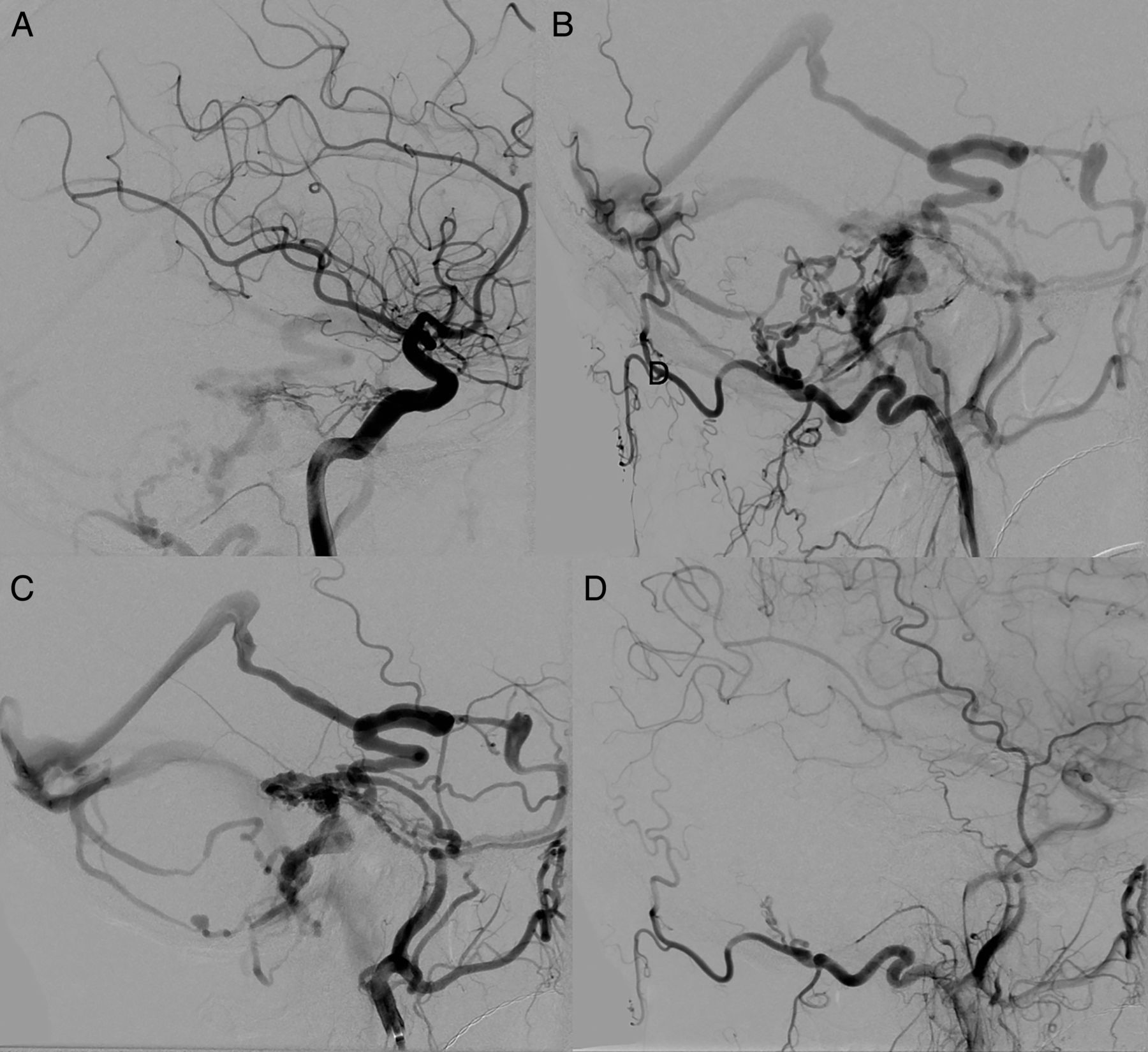
(A) Internal carotid run showing the meningohypophyseal feeders. (B) Selective run through the occipital artery showing the transosseous feeders. (C) Selective internal maxillary run showing prominent middle meningeal feeders. The middle meningeal artery was catheterized and used for embolizing the fistula. (D) End of procedure run showing angiographic exclusion of the dural arteriovenous fistula.
(A) Pre-embolization angiogram showing the feeding vessel, fistula, and draining vein. (B) Unsubtracted image from the postembolization angiogram showing the PHIL (Precipitating Hydrophobic Injectable Liquid) cast in the fistula (arrow head) and draining vein (arrow). (C) Postembolization angiogram showing angiographic exclusion of the fistula.

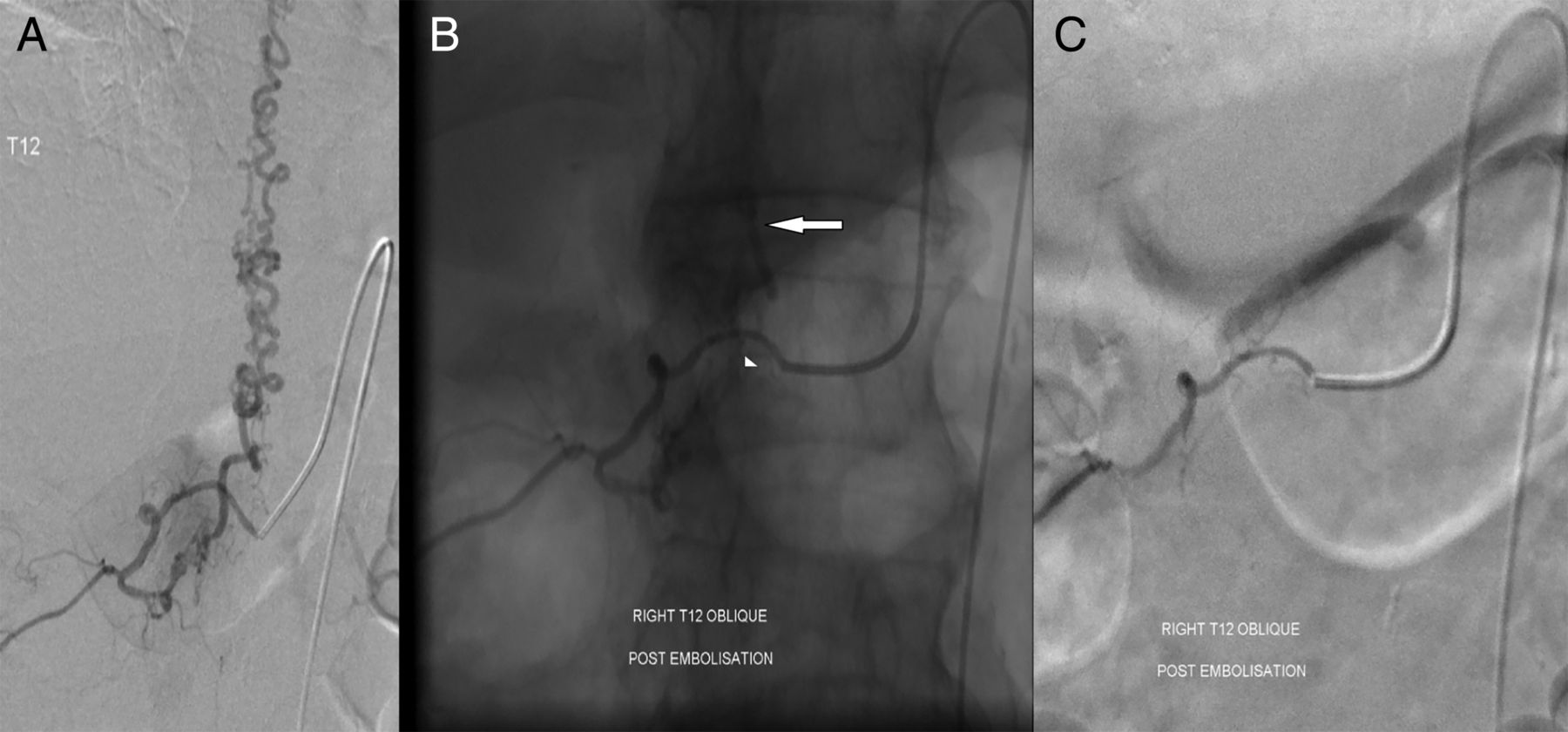
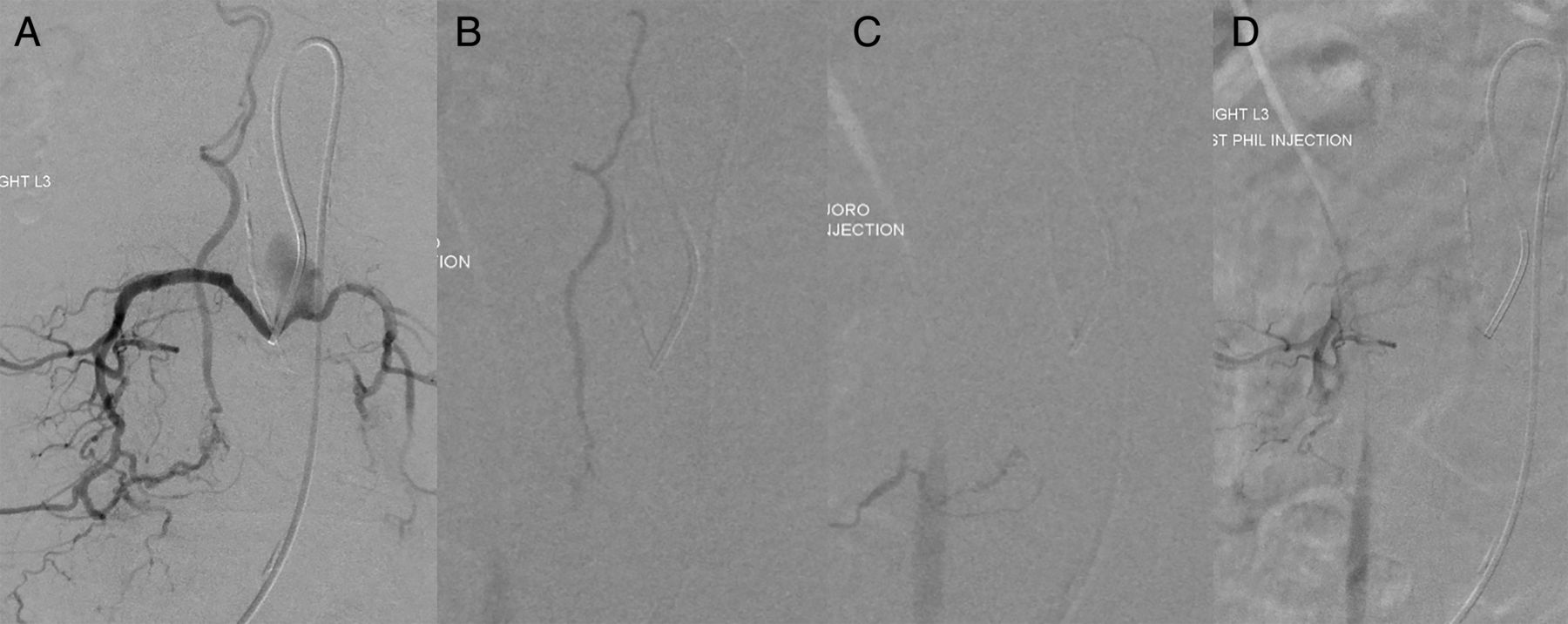
(A) Pre-embolization DSA showing the spinal dural arteriovenous fistula with the fistula being fed by the tortuous feeding branch. (B) PHIL (Precipitating Hydrophobic Injectable Liquid) cast in the radicular vessel, intercostal branch, and the proximal tortuous feeding branch (arrow), but no penetration of the fistula itself or the draining vein.

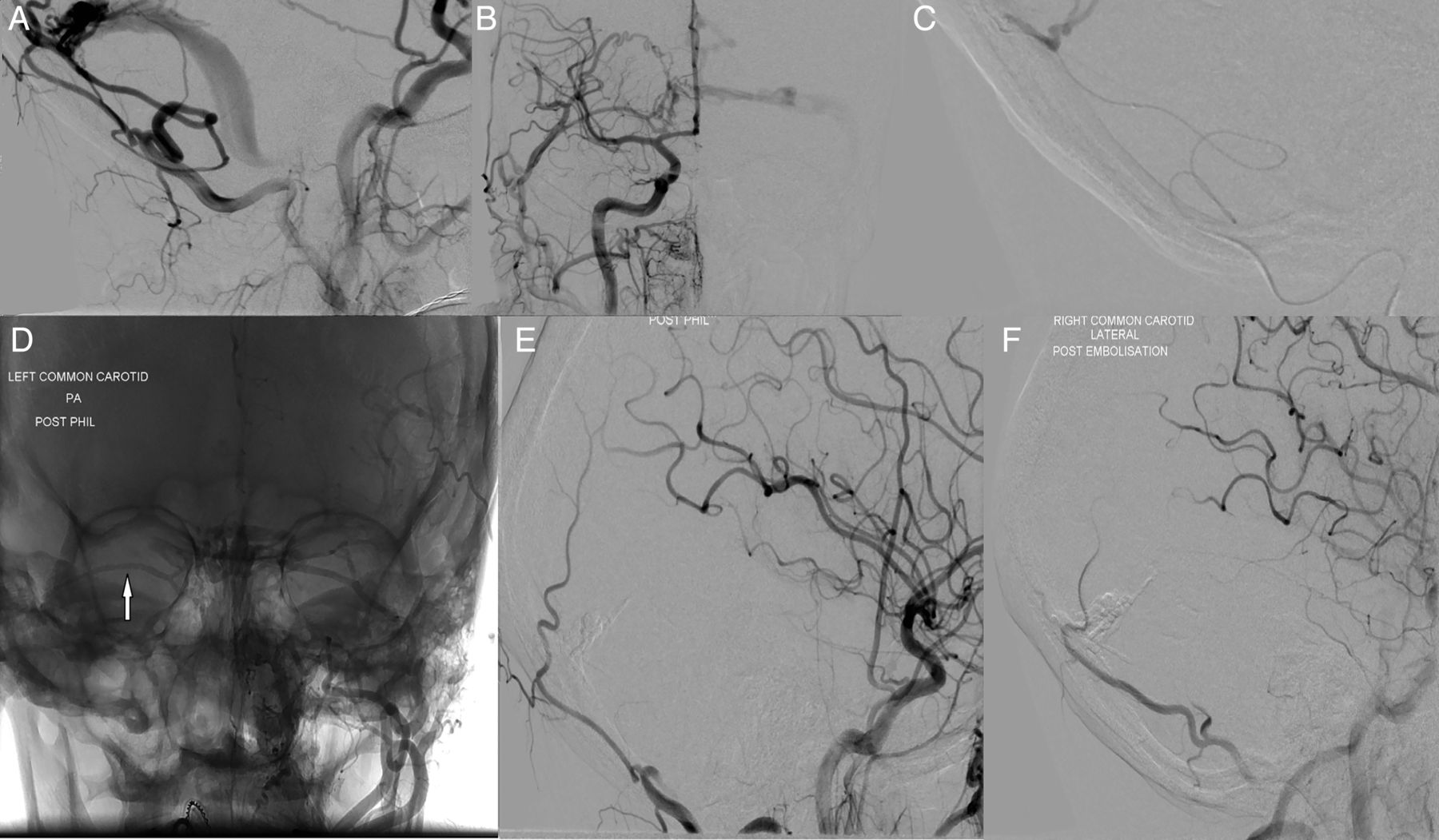
(A) Left common carotid run showing the left-sided fistula primarily fed by branches of the left occipital artery. (B) Right common carotid run showing feeders from the right side. (C) Microcatheter has been navigated through the transosseous feeding vessel arising from the left occipital artery. (D) Unsubtracted image showing the PHIL (Precipitating Hydrophobic Injectable Liquid) cast with retrograde filling of the right-sided feeders (arrow). (E) Postembolization left common carotid run showing exclusion of the fistula. (F) Postembolization right common carotid run showing exclusion of the fistula.
All the DAVFs were successfully treated with single pedicle injections achieving complete angiographic exclusion of the DAVFs and therefore angiographic cure at the time of embolization, except for one spinal DAVF where embolization failed. Both patients successfully treated for spinal DAVFs showed improvement in lower leg power after the procedure. Apart from the intended breakage of the tip of the detachable tip microcatheters, no microcatheter breakage or retention occurred in this series. This included catheters with non-detachable tips used in three of the patients. No adverse physiologic changes were seen during the injections. There was no vessel injury, microcatheter rupture, or cranial nerve deficits in our series.
Some filling of the DAVF nidus was seen with the first or second injection of PHIL in all of the technically successful cases. When reflux was seen, waiting for seconds to a minute was only necessary before forward flow or flow into another DAVF feeding branch occurred. With progressive intermittent injections, it was possible to achieve venous penetration and retrograde flow of the embolic material into other vessels feeding the DAVFs to achieve complete obliteration of DAVFs. The only unwanted embolization that occurred was in one patient with the failed spinal dural fistula embolization, where reflux of embolic material into the intercostal artery was allowed in a controlled manner by the operator in the hope of achieving penetration of the fistula, with no clinical sequelae.
Venous penetration of the fistula was achieved in all of the technically successful DAVFs except in one small ethmoidal fistula where there was adequate penetration of the DAVF nidus by the embolic material. Pre-embolization runs confirmed the distal position of the detachable tip catheter with some antegrade filling of the nasal vessels. Though filling of the DAVF nidus was seen with PHIL injection, no venous penetration occurred in this case. There was spasm and contrast stasis in the ophthalmic artery requiring microcatheter withdrawal. The spasm had completely reversed with occlusion of the feeding branch and no further embolization was attempted in this case (figure 2).
In the one case a Scepter C balloon was used, kept inflated during the whole period of embolization, allowing no reflux of PHIL. The Scepter C balloon was easily deflated after the PHIL injection and retrieved with no difficulty.
In one of the cases, breakaway and minimal but rapid forward migration of the solidifying PHIL cast within the draining vein was seen (figure 9). Also, in the same patient minimal forward migration of a smaller cast fragment was identified (figure 9).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Unsubtracted image at the beginning of the embolization with minimal venous penetration of the embolic agent. (B) Note the emerging PHIL (Precipitating Hydrophobic Injectable Liquid) cast in the proximal vein (white arrow). (C) Note that the cast has now deformed and started to migrate from the initial position (white arrow). (D) The PHIL cast has now migrated further in the draining vein (white arrow). (E) Compare the position of the small cast material in the draining vein in relation to the groove formed by meningeal vessels in the skull vault in (A) and (E), the latter image showing some migration (black arrow).
Two patients, one with a sigmoid DAVF and the other a tentorial/falx cerebelli DAVF, experienced headache after the procedure, which was controlled with analgesia. A CT scan was done in one of these patients owing to the severity of headache, which excluded any intracranial hemorrhage or parenchymal ischemia. One patient with spinal DAVF had post-anesthetic urinary retention, which fully resolved within 48 h. No other complication occurred in any of the patients.
Discussion
Both n-BCA and Onyx have been used for endovascular treatment of DAVFs with good results.1–3 There are marked differences between the two agents in injection techniques, and operator familiarity is key with both agents. A detailed comparison of the physical and technical properties of these agents is beyond the scope of this article.
In a histologic analysis of resected brain arteriovenous malformations, penetration of Onyx was seen in vessels up to 5 µm in comparison with 20 µm with n-BCA with equal incidence of inflammatory changes in both groups.4 Therefore, given the properties of PHIL, it is likely to achieve deeper penetration like Onyx. PHIL differs from other liquid embolic agents in that it uses iodinated contrast to provide radio-opacity, while it is still a DMSO-based agent like Onyx. Lack of suspended tantalum obviates the need for prior agitation, unlike Onyx. Being a DMSO-based occlusive non-adhesive agent, repeated injections can still be done with PHIL through the same microcatheter like Onyx and unlike n-BCA.
Though n-BCA and Onyx have been used in treating DAVFs, both agents have their own limitations. Advantages with n-BCA are high thrombogenicity, and therefore only a minimal volume of n-BCA is required to achieve occlusion with less screening time and therefore, radiation. However n-BCA injection is difficult to control and requires immediate microcatheter withdrawal, therefore it is much less controllable than Onyx. Cure rates are variable with n-BCA with an immediate angiographic obliteration rate of 56% reported in a recent series of intracranial DAVFs and 60% in spinal DAVFs.5 ,6 The main limitation with Onyx is the difficulty in achieving forward flow and therefore penetration of the fistula and the draining vein, compromising further attempts at embolization and limiting chances of anatomic cure with endovascular treatment. This probably accounts for the suboptimal cure rates reported with Onyx in DAVFs in some series.7
Forward flow was unchallenging to achieve with PHIL, with at least some DAVF nidal filling seen in all our technically successful cases with the first or second injection of PHIL, if reflux with the first injection of PHIL warranted it being paused. Though filling of the fistulous nidus was often incomplete with the first or second injection, only minimal waiting was required before further injections to achieve progressive DAVF nidal, venous, and retrograde filling of other DAVF feeders could be achieved. In the one technical failure in the series, tortuous anatomy prevented distal navigation of the microcatheter to enable the embolic material to penetrate the fistula. The operators felt that it was much easier to achieve forward flow of PHIL with only minimal waiting time required in between injections to achieve progressive embolization. Venous penetration of the embolic material is key to achieving DAVF cure.6 ,7 Venous penetration was achieved in all but one of our successful cases where the fistula was too small and adequate penetration of the fistulous nidus was achieved (figure 2).
Being an iodinated contrast-based embolic material, radio-opacity with PHIL was less than would have been expected with Onyx (figure 9). This was not a limitation in any of our cases, including the spinal DAVFs. PHIL was easy to visualize on a non-contrasted road map, aiding the operator's confidence to proceed with further injection. No unrecognized non-target embolization occurred in our series.
The cast migration seen in case 3 occurred early in the procedure. PHIL reaching the draining vein would not have completely solidified at this stage and migration of the cast was aided by the flow in the draining vein. The observed migration was only minimal and did not limit the embolization procedure. Forward flow of the unsolidified embolic agent is to be expected in any liquid embolic injection with high flow and the operator should be prepared to deal with the situation.
The use of dual lumen DMSO compatible balloons is well described for Onyx injection.8 ,9 In the one case where the Scepter C balloon was used, excellent distal flow of PHIL was obtained through the tortuous elongated middle meningeal artery to achieve venous penetration and retrograde filling of the other DAVF feeders (figure 3). No balloon adherence was encountered upon retrieval of the Scepter C.
We acknowledge that this series has only a limited number of patients from which to draw any clinical conclusions. From this limited series, PHIL met the authors’ expectations and seems to be a promising liquid embolic agent in treating DAVFs given its relative ease in achieving forward flow, progressive embolization, and retrograde filling of other fistula feeders with good results. Procedure times may be quicker with PHIL than with Onyx with benefits of reduced radiation exposure, but more studies are needed before any conclusions can be drawn.
Conclusion
Our limited experience with PHIL seems positive and potentially has advantages with good forward flow and penetration of the embolic target. Reflux, though encountered, appeared to be less of a limitation, as was radio-opacity. Larger multicenter series are needed to confirm the safety and efficacy of this new embolic material.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online table 1
- Data supplement 2 - Online table 2
Footnotes
Contributors JJL drafted the manuscript. SC, AT, and SL revised and approved the final version of the document.
Competing interests SL does proctoring for Microvention.
Patient consent Obtained.
Ethics approval Obtained from the Research and Development Department at University Hospitals Birmingham NHS Foundation Trust.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors commit to making the relevant anonymized patient data available on reasonable request.