Article Text

Abstract
Background and purpose Many studies demonstrate that both kyphoplasty and vertebroplasty are superior to conservative therapy in the treatment of osteoporotic vertebral body compression fractures. We performed a systematic review and meta-analysis of studies comparing the outcomes of vertebroplasty and kyphoplasty, which included prospective non-randomized, retrospective comparative, and randomized studies.
Materials and methods We searched MEDLINE, EMBASE, and the Web of Science databases for studies of kyphoplasty versus vertebroplasty from 1 January 1990 to 30 November 2014 and compared the following outcomes: procedure characteristics, pain and disability improvement, complications and anatomic outcomes. A subgroup analysis was performed comparing pain outcomes based on the risk of bias.
Results 29 studies enrolling 2838 patients (1384 kyphoplasty and 1454 vertebroplasty) were included. 16 prospective non-randomized studies, 10 retrospective comparative studies, and 3 randomized controlled studies were included. No significant differences were found in mean pain scores between the two groups postoperatively (2.9±1.5 kyphoplasty vs 2.9±1.7 vertebroplasty, p=0.39) and at 12 months (2.7±1.8 kyphoplasty vs 3.2±1.8 vertebroplasty, p=0.64). No significant differences were found in disability postoperatively (34.7±7.1 kyphoplasty group vs 36.3±7.8 vertebroplasty group, p=0.74) or at 12 months (28.3±16 kyphoplasty group vs 29.6±13.9 vertebroplasty group, p=0.70). Kyphoplasty was associated with lower odds of new fractures (p=0.06), less extraosseous cement leakage (p<0.01), and greater reduction in kyphotic angle (p<0.01).
Conclusions No significant difference was found between vertebroplasty and kyphoplasty in short- and long-term pain and disability outcomes. Further studies are needed to better determine if any particular subgroups of patients would benefit more from vertebroplasty or kyphoplasty in the treatment of vertebral body compression fractures.
- Spine
Statistics from Altmetric.com
Introduction
Osteoporotic vertebral body compression fractures are a significant cause of disability worldwide resulting in pain, spinal deformity, impaired mobility, reduced pulmonary function, and clinical depression.1 While some patients are treated conservatively with activity modification, analgesics and bracing, vertebroplasty or kyphoplasty are alternative interventions for those patients with severe and refractory pain. Many studies have demonstrated that both kyphoplasty and vertebroplasty are superior to conservative therapy in the treatment of osteoporotic vertebral body compression fractures.2–6 As such, the utilization of both of these interventions has increased in the past 10 years.7
While only three prospective randomized trials have been published comparing the safety and efficacy of these two interventions,8–10 various non-randomized trials and meta-analyses have been published. These meta-analyses have been limited in the number of studies or outcomes included and compared. Some of these meta-analyses compared only complications while others compared only pain improvement. In addition, some included lower quality studies and did not include the most current randomized controlled trials (RCTs). The goal of our study was to perform a comprehensive meta-analysis of the existing literature—including data from three RCTs—that directly compares the outcomes of vertebroplasty and kyphoplasty including procedure characteristics, pain improvement, disability improvement, complications, and anatomic outcomes. We hypothesized that kyphoplasty and vertebroplasty would have similar improvements in pain and disability.
Methods
Literature search
To identify comparative studies of kyphoplasty versus vertebroplasty, three databases were searched from 1 January 1990 to 30 November 2014: MEDLINE, EMBASE, and the Web of Science. MEDLINE and EMBASE use controlled vocabulary. Web of Science is text word-based, but tends to be more current and multidisciplinary. The search terms were kyphoplasty and vertebroplasty. We also searched references from multiple articles to find any additional studies on vertebroplasty versus kyphoplasty outcomes not found in the initial literature search. A search of clinicaltrials.gov was performed to identify any completed or ongoing RCTs of vertebroplasty versus kyphoplasty. Authors of any completed clinical trials were contacted to see if they would be able to share any data for purposes of this meta-analysis.
Identified studies from the literature search were then further evaluated for inclusion in the meta-analysis. Inclusion criteria included any retrospective, prospective, non-randomized, or randomized studies with separate arms comparing outcomes of vertebroplasty and kyphoplasty. Exclusion criteria included: (1) case reports; (2) studies not separating outcomes by intervention type (ie, studies that grouped kyphoplasty and vertebroplasty into one treatment group); (3) non-comparative studies (ie, studies with only one group—kyphoplasty or vertebroplasty); and (4) studies which included the treatment of pathologic and non-osteoporotic vertebral body compression fractures (ie, fractures due to cancer or other bone pathology). Two authors reviewed the manuscripts for inclusion. Following selection of the articles, the data were abstracted by two authors.
Risk of bias assessment
We used the Cochrane risk of bias tool for randomized trials and the Newcastle Ottawa Scale for non-randomized trials.11 For randomized trials we evaluated the adequacy of randomization, allocation concealment, loss to follow-up, and blinding. For non-randomized studies we evaluated the selection of the study groups, the comparability of the study groups, and ascertainment of the outcome of interest.11
Outcome variables
Outcomes in this study included: (1) procedure characteristics including mean cement volume injected and mean operation time; (2) pain improvement as reported by the visual analog pain scale (VAS); (3) disability improvement as reported by the Oswestry Disability Index (ODI); (4) complications including adjacent level fracture, overall extraosseous cement leakage, symptomatic extraosseous cement leakage, new vertebral fractures and refractures; and (5) anatomic outcomes including compression ratio, kyphotic angle, and vertebral body height (anterior, middle and posterior body heights). The reporting of pain was grouped into eight time frames: initial, postoperative, 3–14 days, 15–30 days, 1–3 months, 4–6 months, 7–12 months and 12+ months. The reporting of ODI was grouped into seven time frames: initial, postoperative, 15–30 days, 1–3 months, 4–6 months, 7–12 months and 12+ months.
Statistical methods
We considered the experimental approach to be the kyphoplasty group; thus, OR <1 means lower risk of the outcome with kyphoplasty compared to vertebroplasty. For each study we extracted a 2×2 table for binary outcomes and the mean, group sample size, and a measure of variability for continuous outcomes. A random effects model was used for pooling across studies.12 The I2 statistic was used to express the proportion of inconsistency that is not attributable to chance.13 Meta-analysis results were expressed as OR for binary outcomes and weighted mean difference (WMD) for continuous outcomes with respective 95% CIs. Heterogeneity was explored by conducting subgroup analysis based on the risk of bias (RCT vs low risk of bias observational study vs high risk of bias observational study). The outcome of interest for this subgroup analysis was improvement in pain as this was the primary outcome of interest in our study.
We planned to explore the impact of publication bias by constructing funnel plots and testing their symmetry if a sufficient number of studies (>20) was available. Meta-analysis was conducted using Comprehensive Meta-analysis V.2.2, Englewood, New Jersey, USA.
Results
Literature search
A total of 996 articles were found on the initial literature search. Of these, 961 (96.5%) were excluded after abstract review because they included irrelevant content or did not have separate arms directly comparing kyphoplasty and vertebroplasty. Of the remaining 35 articles, six (17.1%) were excluded because they were review articles or used novel devices not fitting the description of vertebroplasty or kyphoplasty. In total, 29 articles (2.9%) with 2838 patients (1384 kyphoplasty and 1454 vertebroplasty) were included in this study. The results of the search are shown in the flow diagram in figure 1. Four studies randomized patients to either vertebroplasty or kyphoplasty, three of which were published and one of which was under review at the time of the meta-analysis.8–10 One of the published randomized trials was excluded due to the use of a novel cement-constraining device.10 One of the randomized trials provided data on complications and anatomic outcomes and did not provide data on pain while the other three included data on pain improvement. The largest study included in our meta-analysis had 381 patients (190 vertebroplasty and 191 kyphoplasty) and the smallest study had 21 patients (10 vertebroplasty and 11 kyphoplasty). In total, 16 prospective non-randomized studies, 10 retrospective comparative studies, and three randomized studies were included. A summary of included studies is provided in table 1.
Studies included in meta-analysis

Process of study selection.
Outcomes
Procedure characteristics
There was no significant difference in the amount of cement injected between the kyphoplasty group and the vertebroplasty group (mean 3.8±0.9 mL vs 3.5±1.2 mL; p=0.49). The mean procedure time was longer for the kyphoplasty group than the vertebroplasty group (39.5±11.5 min vs 32.0±11.8 min; p=0.02).
Pain and disability
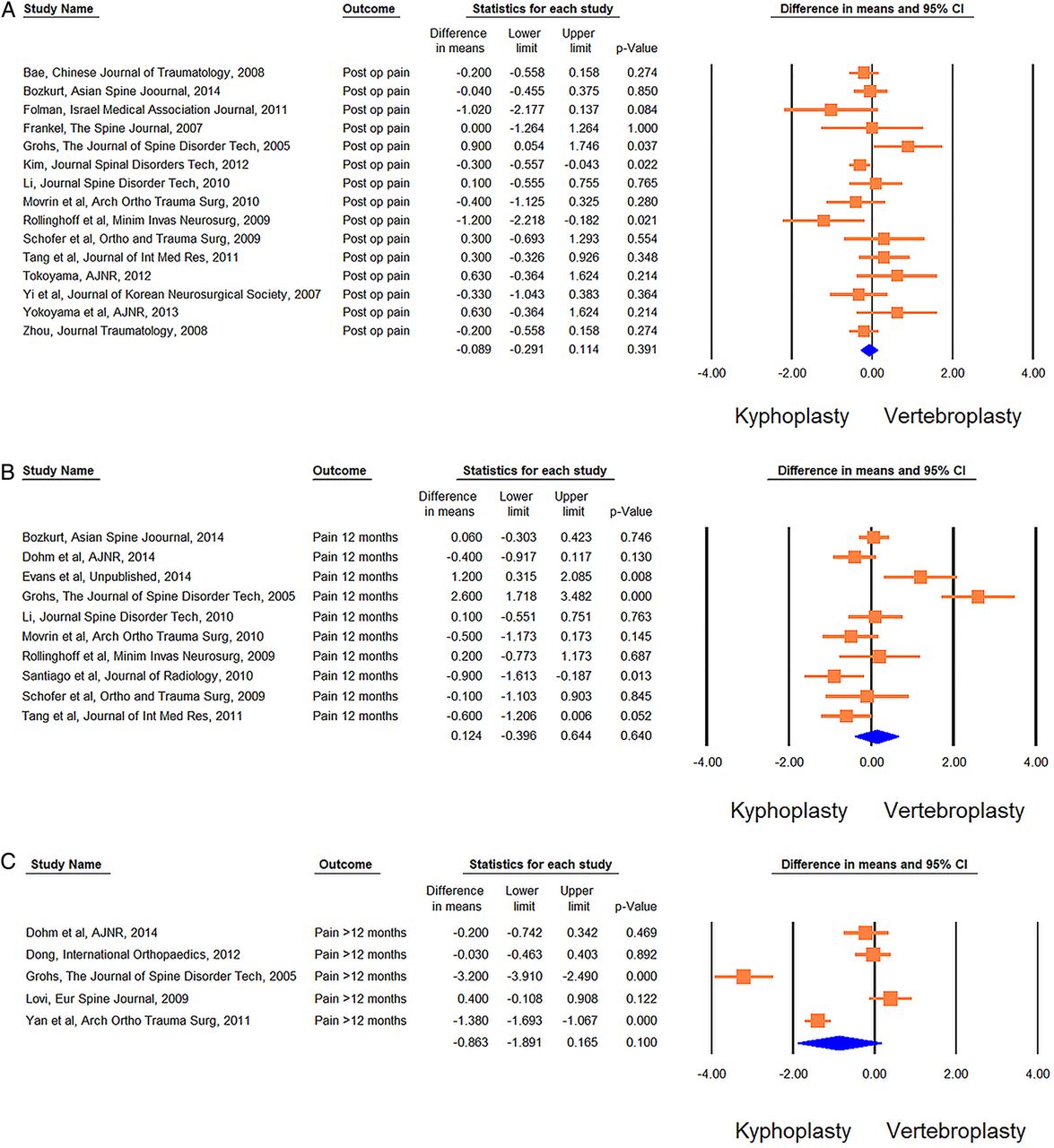
There were no significant differences in pain scores at any time point between vertebroplasty and kyphoplasty in our meta-analysis including all studies. Baseline pain in both groups was 8.0±1.5 and decreased to 2.9±1.5 in the kyphoplasty group in the immediate postoperative phase and to 2.9±1.7 in the vertebroplasty group (p=0.39). At 12 months postoperatively, mean pain in the kyphoplasty group was 2.7±1.8 and 3.2±1.8 in the vertebroplasty group (p=0.64). These data are summarized in figure 2A. Our subgroup analysis of RCTs demonstrated similar results. Mean baseline pain was 7.7±1.5 in the kyphoplasty group and 7.8±1.5 in the vertebroplasty group, mean pain 3–14 days post-procedure was 3.6±2.1 in the kyphoplasty group and 3.3±2.0 in the vertebroplasty group, and mean pain at 12 months was 3.1±2.9 in the kyphoplasty group and 2.9±2.8 in the vertebroplasty group. These data are summarized in figure 2B. Forest plots for pain outcomes in the immediate postoperative period, at 12 months, and at >12 months are provided in figure 3A–C.
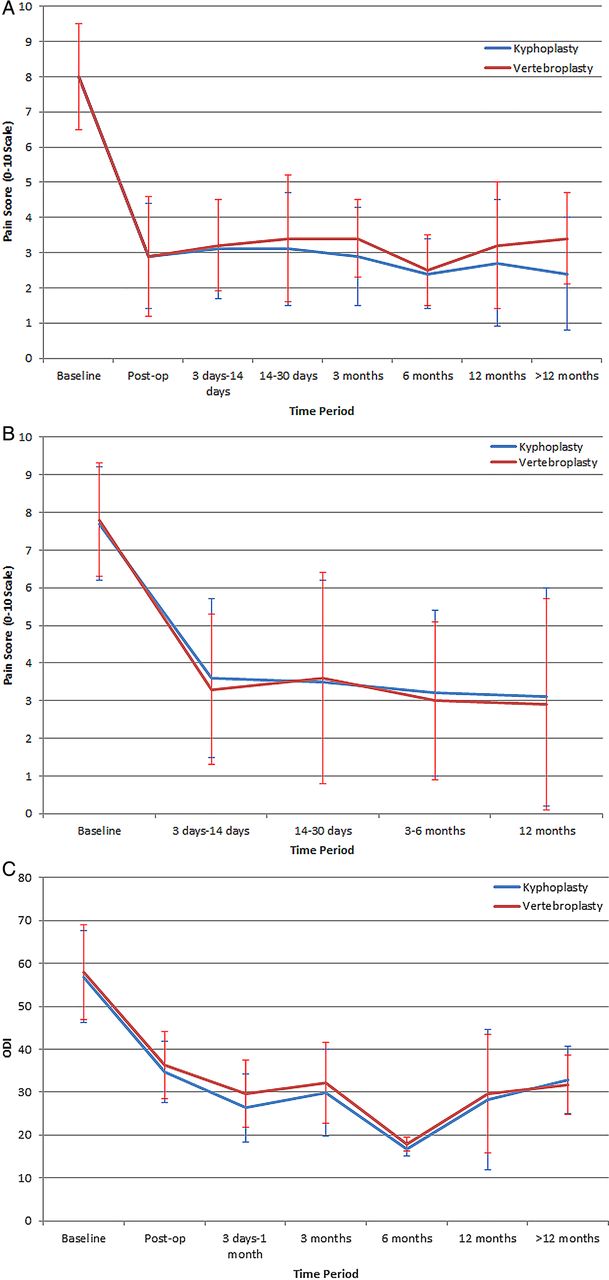
Pain improvement (A) vertebroplasty versus kyphoplasty, all studies, (B) vertebroplasty versus kyphoplasty, randomized controlled trials and (C) disability improvement of vertebroplasty versus kyphoplasty, all studies. ODI, Oswestry Disability Index.
{kind=link}
{kind=link}
{kind=link}
Forest chart pain outcomes in (A) immediate postoperative period, (B) at 12 months and (C) at >12 months.
For disability measured using the ODI scale, there were no significant differences in scores at any time point between vertebroplasty and kyphoplasty. Baseline ODI was 56.9±10.8 in the kyphoplasty group and 58.0±11.0 in the vertebroplasty group. Immediately postoperatively, ODI was 34.7±7.1 in the kyphoplasty group and 36.3±7.8 in the vertebroplasty group (p=0.74). ODI at 12 months was 28.3±16.4 in the kyphoplasty group and 29.6±13.9 in the vertebroplasty group (p=0.70). These data are summarized in figure 2C. Data on WMDs and their 95% CIs for pain and ODI at each time point are provided in online supplementary table 1.
Subgroup analysis
In subgroup analysis comparing pain at the longest point of follow-up based on the type of study design (prospective and non-randomized, retrospective and non-randomized, or RCT), we found that non-controlled and retrospective studies, which are more prone to selection bias, demonstrated higher rates of pain reduction in the kyphoplasty group than controlled prospective studies (RCT: WMD=−0.20, lower limit (LL)=−0.74, upper limit (UL)=0.34; prospective non-randomized studies: WMD=−0.92, LL=−2.78, UL=0.94; retrospective non-randomized studies: WMD=−1.38, LL=−1.69, LL=−1.07; p for difference=0.01).
Anatomic outcomes
Kyphoplasty was associated with a significantly greater reduction in kyphotic angle (initial mean 17.1±6.8° vs postoperative mean 10.8±5.7°) than vertebroplasty (initial mean 15.2±6.6° vs postoperative mean 12.6±5.9°) (p<0.01). There was no significant difference in anterior vertebral body height (p=0.76), middle vertebral height (p=0.69), posterior vertebral height (p=0.93), or compression ratio (p=0.09) between the kyphoplasty and vertebroplasty groups. These findings are summarized in table 2.
Meta-analysis results (anatomical and procedure-related continuous outcomes)
Complications
Extraosseous cement leakage occurred significantly more often in the vertebroplasty group (37.3%) than in the kyphoplasty group (23.3%) (OR 0.40, 95% CI 0.28 to 0.57, p<0.01); however, no significant difference was found in the odds of symptomatic leakage (OR 0.54, 95% CI 0.12 to 2.47, p=0.42). There was no significant difference in the odds of adjacent level fracture (OR 1.04, 95% CI 0.60 to 1.80, p=0.89). Kyphoplasty was associated with a significantly lower odds of new fractures (OR 0.73, 95% CI 0.53 to 1.01, p=0.04). The rate of refracture was similar between the two groups (OR 0.29, 95% CI 0.12 to 71, p=0.01). These findings are summarized in table 3.
Meta-analysis results: complications
Study heterogeneity
For several outcomes, the results were consistent across studies. I2 values were less than 50% for the following outcomes: postoperative pain (I2=38%), postoperative ODI (I2=0%), ODI at 4–6 months (I2=0%), ODI at 7–12 months (I2=0%), ODI at 12+ months (I2=0%), adjacent level fracture (I2=0%), extraosseous cement leakage (I2=43%), symptomatic extraosseous cement leakage (I2=0%), new fractures (I2=0%), and refractures (I2=0%).
On the other hand, I2 values were greater than 50% (indicating substantial heterogeneity) for the following outcomes: pain at 3–14 days (I2=91%), pain at 15–30 days (I2=80%), pain at 1–3 months (I2=94%), pain at 4–6 months (I2=54%), pain at 7–12 months (I2=85%), pain at 12+ months (I2=72%), ODI at 15–30 days (I2=61%), ODI at 1–3 months (I2=80%), anterior vertebral body height (I2=97%), middle vertebral body height (I2=99%), posterior vertebral body height (I2=72%), compression ratio (I2=94%), kyphotic angle (I2=76%), cement volume (I2=97%), and operation time (I2=89%). Therefore, the pooled summary estimates for these outcomes are less reliable.
Publication bias
Egger’s regression test for publication bias did not reveal such bias (p=0.98). However, the analysis for publication bias and construction of funnel plots was not reliable due to the small number of included studies.14
Discussion
This systematic review and meta-analysis demonstrated no significant difference in the postoperative pain and disability characteristics of vertebroplasty and kyphoplasty measured by VAS and ODI at any of the time points studied. This is despite the fact that patients who underwent kyphoplasty had better anatomic outcomes (improvement in kyphotic angle) than those who underwent vertebroplasty. Subgroup analysis of the four RCTs also demonstrated no significant difference in postoperative pain at any time point. These findings, especially those from the subgroup analysis of RCTs, strongly suggest that vertebroplasty and kyphoplasty are therapeutically equivalent in providing pain relief and improving disability of patients with vertebral body compression fractures.
Previous meta-analyses have relied primarily on including non-RCTs and retrospective studies in their meta-analyses. Major limitations of these types of studies include selection and publication bias, respectively. Thus, many previously published meta-analyses are limited by the risk of bias. Our study found that the risk of bias was associated with increased relative pain improvement with kyphoplasty. These findings are similar to a previous systematic review which demonstrated that observational clinical studies showed that kyphoplasty was superior to vertebroplasty in improving short- and long-term pain and disability outcomes; however, prospective controlled clinical trials found no difference in outcomes.9 ,15
In terms of complications, no significant difference was found in the odds of symptomatic extraosseous cement leakage. Patients treated with kyphoplasty had lower odds of new fractures in levels not adjacent to the treated levels and refractures of treated vertebral bodies. Despite the higher rates of new fractures and refractures in patients treated by vertebroplasty, long-term pain and disability outcomes were similar. One potential drawback of the higher rates of refractures and new fractures in the vertebroplasty group would be the added costs of retreatment. Unfortunately, however, very few studies in our analysis examined retreatment rates between groups.
We did not perform any comparison of procedural and long-term care-related costs in our study as these data were not available. While a number of previously published studies have demonstrated decreased inpatient and outpatient procedural costs for vertebroplasty compared with kyphoplasty, long-term cost-effectiveness studies have suggested that kyphoplasty may in fact be more cost-effective.16 ,17 Using data from the FREE and VERTOS II RCTs, Svedbom et al18 found that kyphoplasty was more cost-effective than vertebroplasty, with much of the benefit related to reduced mortality in patients treated by kyphoplasty. Ong et al19 found that, despite higher initial treatment costs of kyphoplasty, vertebroplasty was less cost-effective due to increased utilization of medical resources (partly due to retreatment) in the postoperative period over the 2 years after surgery. Edidin et al20 found that kyphoplasty was cost-effective—and perhaps even cost-saving—compared with vertebroplasty using Medicare claims data. Again, these cost-effectiveness analysis studies are from non-randomized populations and are subject to significant selection bias. These findings highlight the importance of long-term cost and mortality data from future prospective studies and RCTs.
Limitations
Our study has limitations. The majority of the studies comparing vertebroplasty and kyphoplasty published in the current literature and included in our meta-analysis are non-RCTs or retrospective studies and are limited by selection and publication biases. At the time of our literature review, data from only four RCTs comparing vertebroplasty and kyphoplasty were available. This lack of RCTs may explain the high degree of heterogeneity in our results. Our study is also limited by the variable reporting of pain and disability. By including studies which reported pain using the VAS scale and disability using the ODI scale, we excluded studies that did not use these scales which may have altered our results. The range of follow-up data reported varied between studies, and our attempt to use standardized time frames may not be a true representation of the reported VAS values. We were unable to reliably evaluate for publication bias. Finally, our literature search included only published English articles which can result in the exclusion of relevant non-English articles and selection and publication bias.
Conclusions
This systematic review and meta-analysis demonstrated no significant differences between vertebroplasty and kyphoplasty in short- and long-term pain and disability outcomes. While kyphoplasty was associated with improved anatomic outcomes and lower odds of new fracture, both had similar pain and disability outcomes. Further studies are needed to better determine if any particular subgroups of patients would benefit more from vertebroplasty or kyphoplasty in the treatment of vertebral body compression fractures.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors CNG and WB helped design the data collection tools, monitored data collection for the study, cleaned and analyzed the data, and drafted and revised the paper. AJE monitored data collection for the study, cleaned and analyzed the data, and drafted and revised the paper. MHM wrote the statistical analysis plan and drafted and revised the paper. DFK monitored data collection for the whole trial, cleaned and analyzed the data, and drafted and revised the paper.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Our review includes data from an unpublished randomized controlled trial which we have submitted as a supporting document.