Article Text

Abstract
Background Rapid delivery of IV tissue plasminogen activator (tPA) in qualifying patients leads to better clinical outcomes. The American Heart Association has reduced target door-to-needle (DTN) times from 60 to 45 min in the hopes of continued process improvements across institutions.
Objective To start a quality improvement project called CODE FAST in order to reduce DTN times at our institution.
Materials and methods We retrospectively reviewed data from our internally maintained database of patients treated with intravenous tPA before and after implementation of the CODE FAST protocol. We assessed demographic information, time of day and times of arrival to first image and delivery of tPA in patients from February 2014 to February 2015. Outcomes were assessed based on discharge to home. Univariate analysis was performed to assess for improvement in DTN times before and after implementation of the protocol.
Results A total of 93 patients (41 pre-CODE FAST and 52 post-CODE FAST) received IV tPA during the study period. Patients were equally matched between the two groups except that in the pre-CODE FAST era patients receiving tPA were younger and more likely to be men. There was a substantial reduction in door-to-imaging time from a median of 16 to 8 min (p<0.0001) and DTN time with a reduction in the median from 62 to 25 min (p<0.0001). In logistic regression modeling, there was a trend towards more discharges to home in patients treated during the CODE FAST era.
Conclusions We present a quality improvement project that has been overwhelmingly successful in reducing DTN time to <30 min. The template we present may be helpful to other institutions looking to reduce their DTN times and may also reduce costs as we note a trend towards more discharges to home.
- Stroke
- Thrombolysis
Statistics from Altmetric.com
The use of IV tissue plasminogen activator (tPA) for acute ischemic stroke can reduce disability in a significant proportion of patients if delivered in a timely manner. The number needed to treat to prevent one disability at 3 months is 1 in 5 if the drug is delivered within 90 min from symptom onset and increases to 1 in 14 at 4.5 h.1 The impact of time on outcomes has led the American Heart Association to develop Target Stroke with the intervention focused on reducing door-to-needle (DTN) times to <60 min in 2010.2 Interestingly, before the initiative it is estimated that <30% of patients were treated within this time window in the Get With the Guidelines Database. After the initiative, the rate increased to 53.3% in 2013.3 This improvement in times coincided with a reduction of in-hospital mortality rates and discharges to home. Reducing times from onset of symptoms to delivery of tPA is the ultimate goal, but processes at the prehospital and in-hospital phases can be addressed with the potential to reduce DTN time to 20 min.4
Given the importance of timely delivery of tPA to patients with acute ischemic stroke, we implemented a protocol called CODE FAST in September 2014 aimed at reducing DTN times. The initiative took into account best reported practices and adjusted for what was feasible at our institution.
Methods
Our institution is a licensed 633 bed hospital serving roughly two million citizens in a seven county network. The hospital admits close to 1200 patients with ischemic stroke and transient ischemic attack annually and was primary stroke certified in 2010. Since then, the institution has been accredited as a Comprehensive Stroke Center by the Joint Commission. Recently, our institution developed the infrastructure for a comprehensive stroke center and hired vascular neurology neurohospitalists, neuro-critical care and neuroendovascular specialists. In September 2014 a new process for delivery of IV tPA was coined CODE FAST.
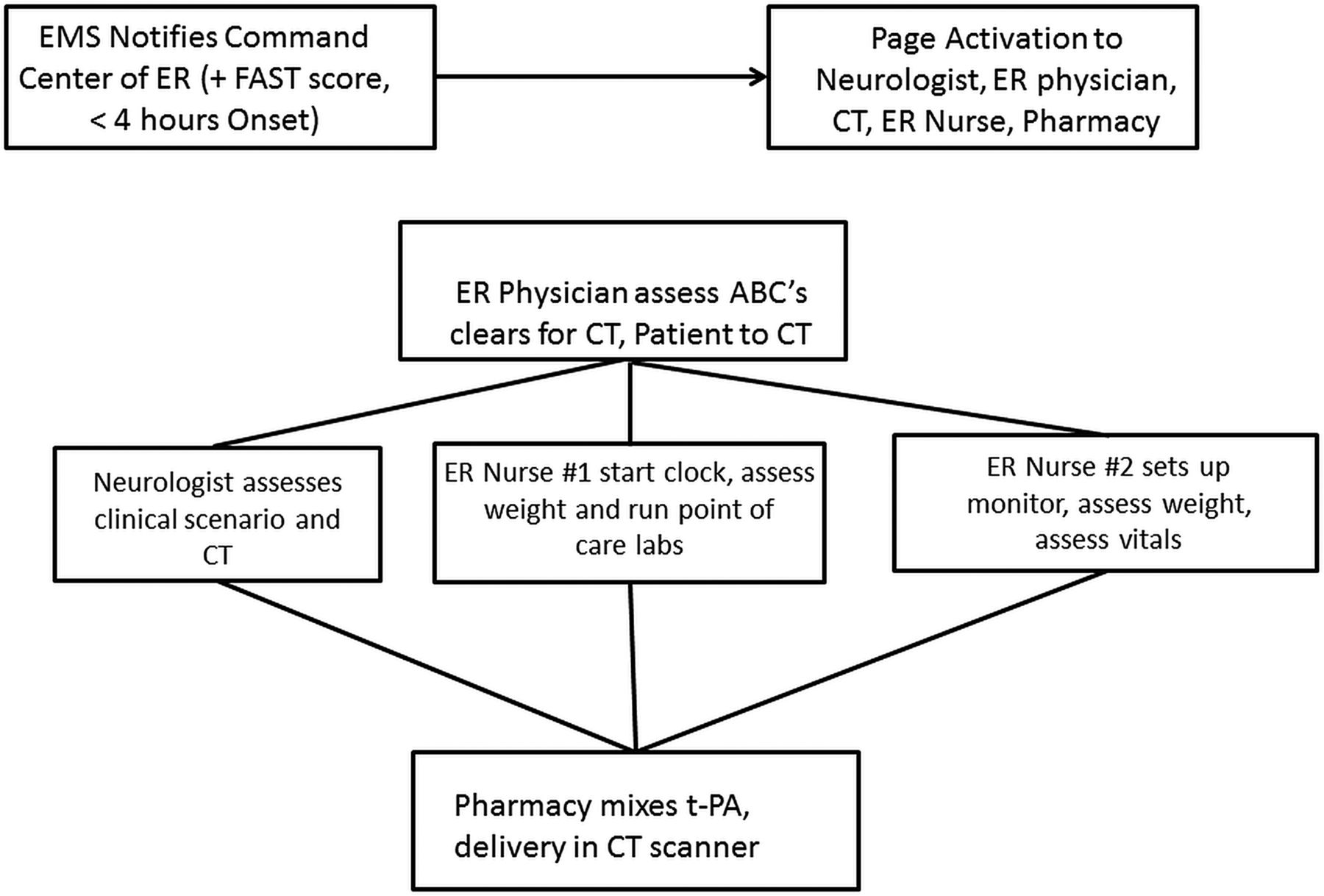
Before the development of CODE FAST patients were brought in by the emergency medical services (EMS) to an emergency room bed without pre-notification. The emergency room physician would evaluate the patient and obtain a CT scan and contact the neurologist on call. It was recognized that the process could be improved with parallel processing and thus the CODE FAST initiative was developed in conjunction with EMS (prehospital providers), the emergency room nursing staff and physicians, emergency department (ED) command center technicians, stroke neurohospitalists, pharmacy, radiology, neurocritical care, and radiology technicians (figure 1). If a patient was noted to have a positive facial drooping, arm weakness, speech difficulties and time (FAST) (focused assessment with sonography in trauma) examination in the field and was under 4 h from symptom onset, the EMS team would contact the Kennestone Hospital emergency room command center to pre-notify them of the patient arrival. The command center sends a page to the core team with the time the patient was last known to be normal, specific symptoms (ie, right-sided hemiparesis), and age of the patient. Upon arrival, the patient is quickly assessed for airway and hemodynamics in the ED hallway while remaining on the EMS stretcher. After this swift evaluation the patient is taken to the CT scan directly if medically stable. Data are delivered from EMS to the neurologist while transporting to the CT scanner and a National Institutes of Health Stroke Scale (NIHSS) score is promptly obtained by the neurohospitalist. Blood is drawn by the emergency room nursing staff to assess for an i-STAT chemistry panel and international normalised ratio (INR). While the CT scan is being acquired, details of the weight of the patient are provided to the pharmacist, and the neurologist confirms the time when the patient was last known to be normal and medical history to ensure that the patient meets the criteria for IV tPA. The IV tPA is mixed by the pharmacist and delivered in the CT scanner while being monitored by the ED registered nurse for vital sign checks and neurological assessments. If additional imaging is required (ie, CT angiography and/or CT perfusion) the decision is made by the neurologist as the IV tPA is being delivered.
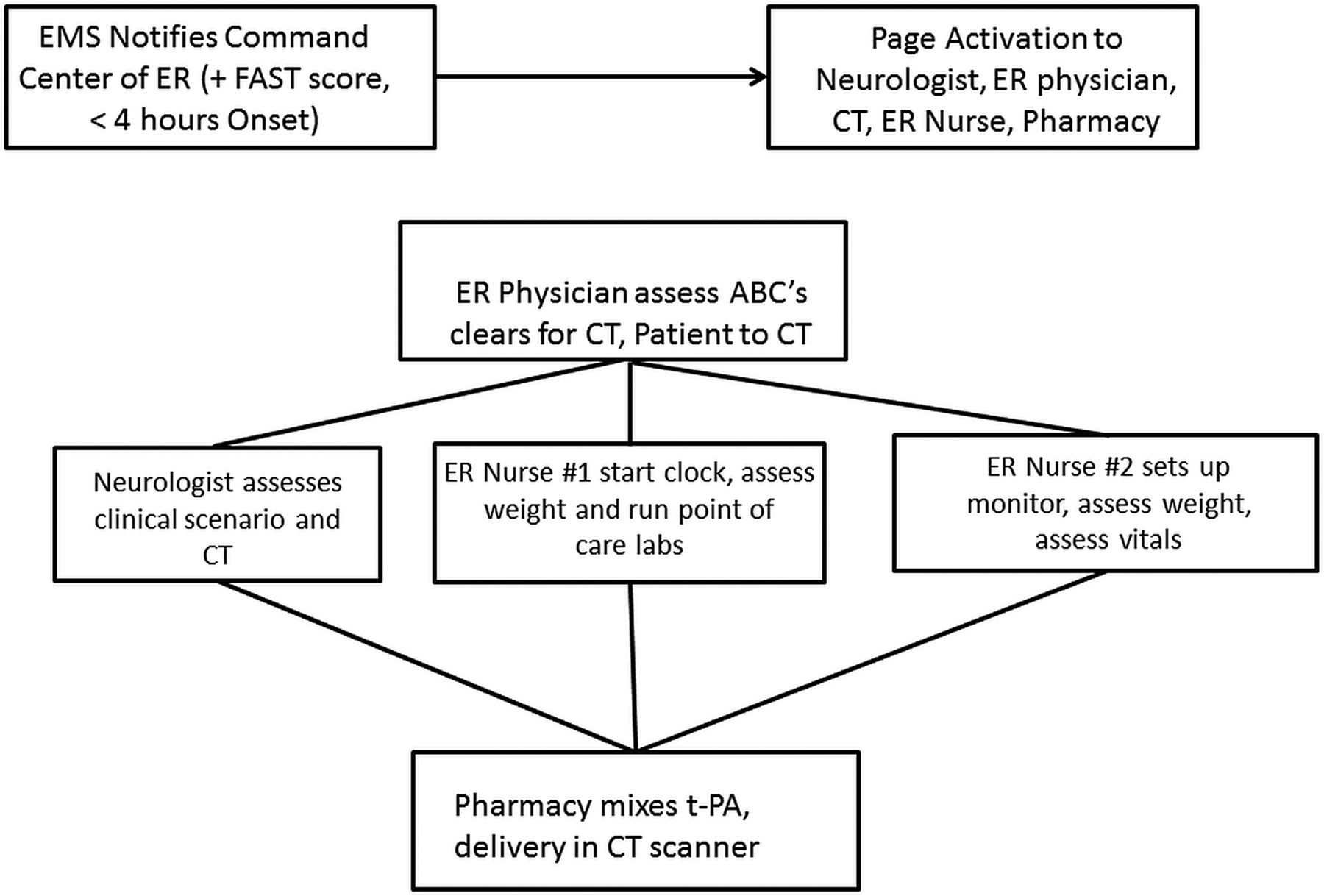
CODE FAST workflow of pre-notification activation and roles of each team member. EMS, emergency medical services; ER, emergency room; tPA, tissue plasminogen activator.
For patients we analyzed the demographic information, baseline NIHSS, number of patients in whom the CODE FAST was activated, DTN time, radiographic imaging data, and discharge destination to home versus other from February 2014 to February 2015. The CODE FAST initiative started on 8 September 2015 and patients were categorized by date as before implementation or after implementation of the CODE FAST protocol.
Statistical analysis
An analysis was performed comparing patients before implementation of CODE FAST with those after implementation. All continuous variables were analyzed using the Student t test and Mann–Whitney U test, as determined by the equality of variances and distribution. A Fisher exact test was used for categorical variables. All variables with a p value <0.20 on univariable modeling were included in a multivariable analysis. A binary logistic regression model was developed to assess for independent predictors of discharge to home.
Results
Figure 2 shows the number of patients admitted with ischemic stroke before and after institution of the CODE FAST protocol. Of note, there were 244 activations between September 2014 and February 2015 and 52 (21%) received IV tPA. A total of 93 patients in a period of 12 months received IV tPA for acute ischemic stroke at our institution. There were no instances of symptomatic intracranial hemorrhage during this time. Forty-one of the patients were treated from 1 February 2014 to 8 September 2014 and 52 patients from 9 September 2014 to 28 February 2015 after implementation of CODE FAST. Table 1 compares the baseline characteristics of patients who were treated before implementation of the protocol with those treated after. Of note, there was a substantial reduction in door-to-imaging time from a median of 16 to 8 min (p<0.0001) and door-to-puncture time with a reduction in the median from 62 to 25 min (p<0.0001). This corresponded to a trend towards more patients being discharged to home. In patients arriving after hours between 19:00 and 6:59, the mean DTN time for the pre-CODE FAST population was 67±19 min compared with 26±12 min (p<0.0002). This result shows consistency in reducing DTN times outside normal hours. We also noted, that 45/52 (87%) of patients during the CODE FAST time frame were treated under 45 min compared with 2/41 (5%) pre-CODE FAST, p<0.0001. Additionally, 18 of the 52 patients (35%) had a DTN time of <20 min.
Demographic information comparing patients treated before implementation of CODE FAST with CODE FAST treated patients with intravenous tPA

Summary of the total number of patients divided into the pre-CODE FAST period and post-CODE FAST period. tPA, tissue plasminogen activator.
Figure 3 summarizes the DTN times by month and shows the sharp decline in times after implementation of the CODE FAST initiative. Also of note, the number of patients receiving tPA increased after the initiative. Moreover, no variability was noted from month to month and the process has remained in control since implementation. Table 2 summarizes the binary logistic regression model for independent variables that are associated with discharge to home. As expected, a younger age and lower presenting NIHSS were independently associated with discharge to home. Patients treated during the months of CODE FAST had a trend towards a higher probability towards discharge to home. There was significant colinearity with DTN time and CODE FAST patients and thus both variables could not be included in the model.
Binary logistic regression model of predictor to discharge home

{kind=link}
{kind=link}
{kind=link}
Bar graph representing average door-to-needle times by month and the number of patients treated by month. tPA, tissue plasminogen activator.
Discussion
Our study shows that DTN time can be significantly reduced and maintained at <30 min with proper implementation of a multidisciplinary protocol. By reducing DTN times, we have seen an improving trend in discharges to home compared with a rehabilitation or nursing facility, which is consistent with the existing literature. This study provides a framework showing how a non-teaching hospital in the USA can reduce its DTN times dramatically.
The Helsinki protocol4 and the value stream analysis performed by the group at Washington University5 have been cited as methods that can reduce DTN times. Implementation of the Helisinki protocol at the Royal Melbourne Hospital reduced DTN times during work hours but had no effect out-of-hours.6 We also note that the coordination of care from the prehospital phase to the hospital phase is crucial in reducing DTN times. Although we were not able to capture the first medical contact in our current dataset, we are currently looking at process improvements at the field level. The early EMS notification to our command center enables coordination of care before the patient's arrival. By having a neurohospitalist at the bedside upon arrival, we have a team leader present who can help to direct decision-making in real time. Moreover, the neurologist can review the CT scan for hemorrhage and execute the tPA delivery more expeditiously as shown by roughly one-third of patients being treated in <20 min. Others have also shown that the presence of a neurohospitalist in the decision tree for tPA can reduce DTN times.7
The ability of emergency room physicians to assist in the stroke evaluation process can help to reduce target times particularly out-of-hours. Once center found that providing advanced neuroscience training to their emergency room physicians reduced their DTN times from 83 min to 35 min.8 In our protocol, we ensured that the emergency room physician was an integral part of the decision process. They perform the initial airway and hemodynamic assessment before transition by EMS to the CT scanner. After this rapid evaluation and clearance, the neurologist goes with the patient to the CT scanner. If the neurologist is delayed, the emergency room physician will accompany the patient and stay in contact with the neurologist in order to optimize tPA delivery.
A total of 244 activations of CODE FAST occurred during the study period with only 21% of patients receiving intravenous tPA. This number may raise some concerns that the system may be overused and lead to fatigue in the future. There is a challenge to balance not missing patients who should be treated with overactivation of the triage system. We are in the process of determining if the protocol can be refined to ensure that that time when the patient was last known to be normal is clear to the prehospital provider and that only patients with a FAST positive screen are activated. This will require further education but does present opportunities to refine the process.
There are several limitations to such an analysis. First, this is a single-center study and the generalizability of the results may be limited. Second, this is a recent initiative and the sustainability of the DTN times will need to be monitored. Third, there is a risk of overparameterization in binary logistic regression modeling due to the number of univariate variables we considered as potential confounders. Lastly, we did not look at analysis of 90-day modified Rankin Scores, which may be more consistent with the literature, but do believe a discharge to home is a meaningful measure of outcomes and cost assessment.
In conclusion, we have demonstrated a successful quality improvement initiative to reduce DTN time for delivery of IV tPA to <30 min. The principles of this process can be broadened to reduce treatment times for endovascular therapies. Moreover, future analysis will be performed to assess the reduced cost for patient care as fewer patients will require inpatient rehabilitation or nursing facilities with more rapid treatment.
Footnotes
Contributors LB, KO, SD, RG: conception of the research protocol and writing of the manuscript. VC, RR, CH DR: data collection and analysis. AK, JTH, RG: statistical analysis. SZ, LB, KO, RG: critical revision of the manuscript.
Competing interests RG: consultant Stryker Neurovascular, Covidien, Rapid Medical; research funding/grant support from Penumbra, Stryker Neurovascular, Covidien, Zoll and Wellstar Foundation; associate editor Journal of Neuroimaging, Journal of Neurointerventional Surgery, Interventional Neurology; royalties from UpToDate.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data from this study can be shared upon request to the corresponding author with an approved institutional review board protocol.