Article Text

Abstract
Introduction The natural history of acute ischemic stroke (AIS) due to basilar artery occlusion (BAO) is poor. Endovascular reperfusion therapy (EVT) improves recanalization rates in patients with emergent large vessel intracranial occlusion.
Objective To examine the hypothesis that good collateral patterns identified by pretreatment CT angiography (CTA) might be associated with favorable outcomes after EVT.
Methods We conducted a retrospective chart review of patients presenting with AIS due to BAO in a tertiary care stroke center during a 4-year period. BAO was diagnosed by CTA in all cases. Admission stroke severity was documented using the National Institute of Health Stroke Scale (NIHSS) score. Pretreatment collateral score for posterior circulation was defined as follows: 0, no posterior communicating artery (PCOM); 1, unilateral PCOM; 2, bilateral PCOM. Favorable outcome was defined as modified Rankin Scale score of 0–2 at 3 months.
Results A total of 21 patients with AIS due to BAO (age range 31–84 years, median admission NIHSS score: 18 points, range 2–38) underwent EVT. Eleven of 21 patients (52.4%) had bilateral PCOMs, while unilateral PCOM was seen in 3 patients (14.3%). Patients with bilateral PCOMs tended (p=0.261) to have less severe stroke at admission than those with absent/unilateral PCOM (median NIHSS score 18 vs 27 points). Neurological improvement during hospitalization (quantified by the median decrease in NIHSS score) and the rate of 3-month functional independence were greater in patients with good collaterals (16 vs 0 points (p=0.016) and 72.7% vs 0% (p=0.001)).
Conclusions The presence of bilateral PCOMs on pretreatment CTA appears to be associated with more favorable outcomes in BAO treated with EVT.
- CT Angiography
- Stroke
- Thrombectomy
- Thrombolysis
Statistics from Altmetric.com
Introduction
Acute ischemic stroke (AIS) due to basilar artery occlusion (BAO) accounts for 6–10% of all large vessel strokes.1 Acute BAO is a catastrophic disease with a mortality rate ranging from 40% to 86%.1 Several recent randomized trials have shown improved outcomes after endovascular treatment (EVT) for emergent large vessel occlusion compared with IV thrombolysis but these studies did not include patients with BAO.2–6
A recent meta-analysis showed that the recanalization of acute BAO leads to a twofold reduction in mortality and a 1.5-fold reduction in the risk of death or dependency.7 Recanalization rates are higher after EVT than with systemic thrombolysis in observational studies of BAO.8 ,9 However, the results of the BASICS (Basilar Artery International Cooperation Study) registry demonstrated that despite the higher rates of recanalization with EVT, the rate of favorable outcome did not differ significantly between patients receiving systemic thrombolysis or EVT.10 The recently completed ENDOSTROKE study showed that only 34% of patients with BAO achieved good clinical outcome despite a 79% rate of recanalization with EVT. Lower admission National Institute of Health Stroke Scale (NIHSS) scores and better collateralization status on DSA were independent predictors of good clinical outcome.11
The size of the final infarct and growth of the penumbra is influenced by the degree of collaterals. Several studies have demonstrated that good collaterals on pretreatment CT angiography (CTA) would predict favorable outcome after EVT for anterior circulation large vessel occlusion AIS.12 ,13 However, limited data exist on classification of posterior circulation collaterals on pretreatment CTA and their prognostic value after EVT for BAO. We propose a new classification system for posterior circulation collaterals on pretreatment CTA and hypothesize that good collateral patterns predict favorable outcome after EVT.
Methods
This study is a retrospective chart review of the University of Tennessee Health Science Center Acute Ischemic Stroke Database from February 2011 to July 2014 of consecutive patients who underwent EVT for the treatment of AIS due to BAO. The major inclusion criteria were the presence of BAO on pretreatment CTA and age >18 years. We identified 24 consecutive patients who presented with acute BAO and underwent EVT. Of those, we excluded three patients because of a lack of CTA. A chart review was performed to collect information on baseline characteristics, details of treatment, and determination of clinical outcome.
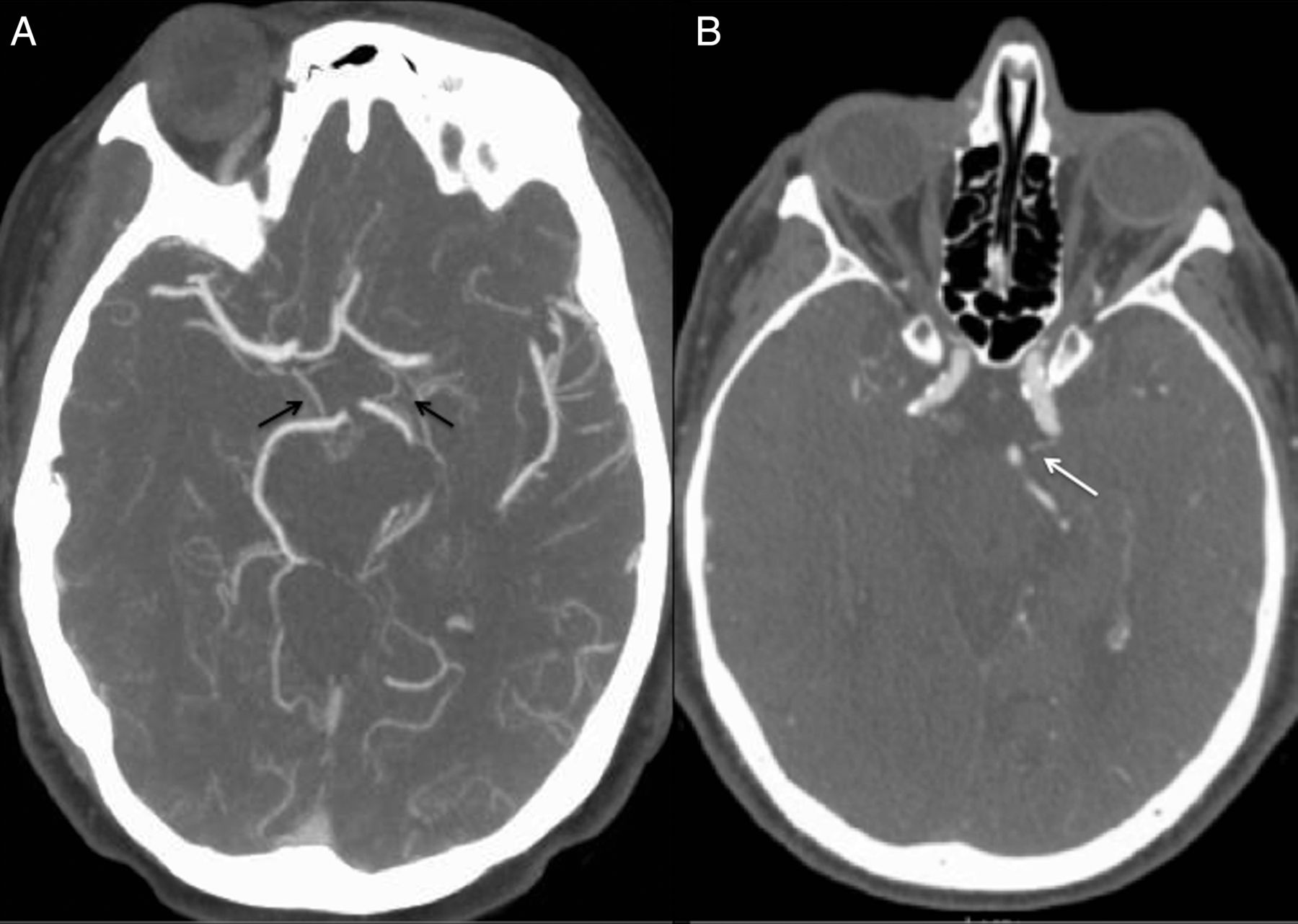
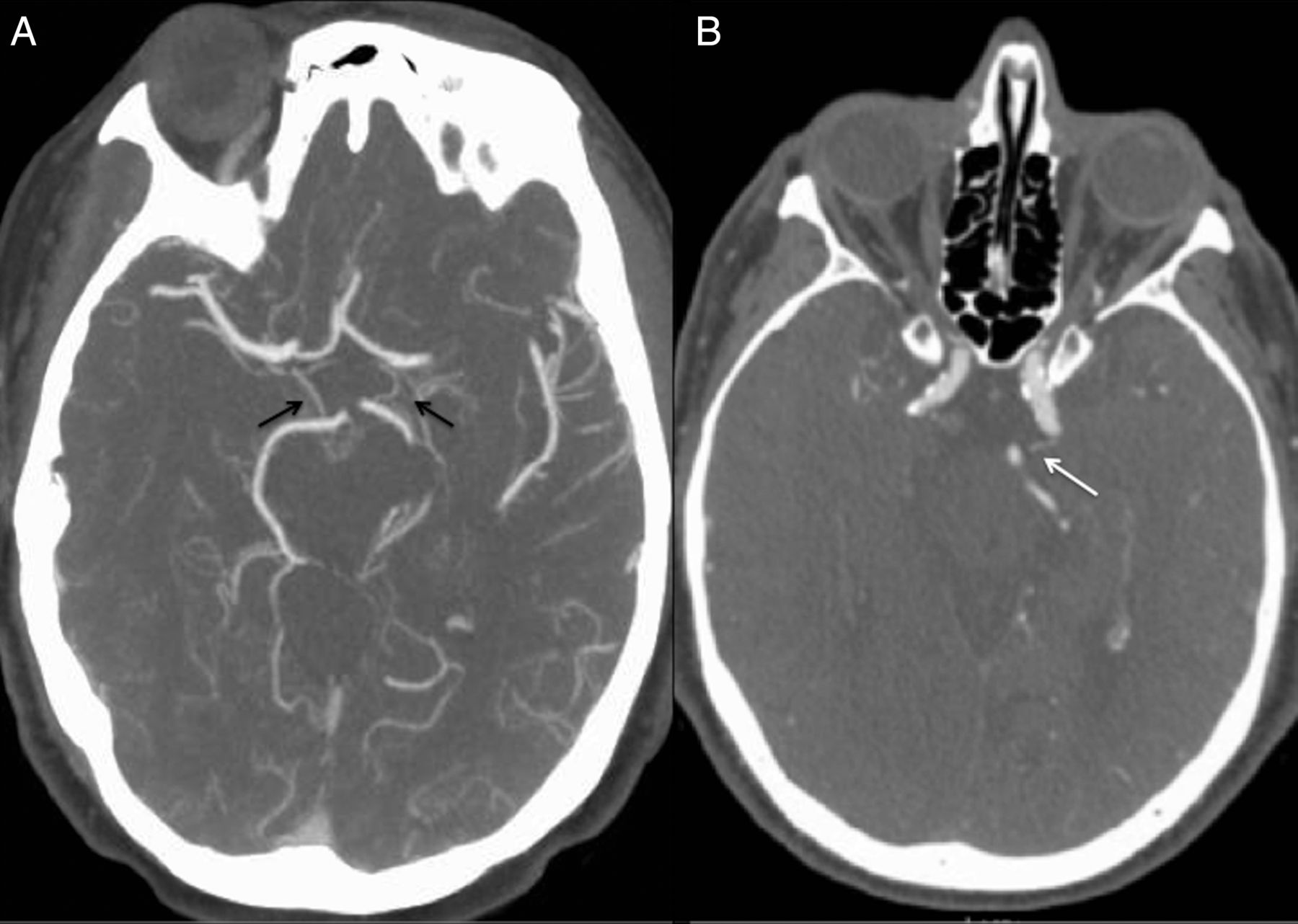
CT and CTA were performed on a 64-slice scanner. CT slice thickness was 1.25 mm with acquisitions in axial, sagittal, and coronal planes with 3D reformations. All diagnostic radiologic imaging was independently interpreted by two neurointerventionalists (LE, VTD). Admission stroke severity was documented using NIHSS score. Pretreatment collateral score (CS) for posterior circulation was defined as follows: 0—no posterior communicating artery (PCOM), 1—unilateral PCOM, 2—bilateral PCOM. Patients with good collaterals had a CS of 2, while poor collateral status was defined as CS of 0 or 1. The presence of PCOM for the purposes of this study included the presence of a P1 segment of posterior cerebral artery (PCA) that attaches to the basilar artery apex (figure 1).
{kind=link}
(A) CT angiography (CTA) image from a patient in their late 60s with basilar occlusion with good collaterals with two large posterior communicating arteries (black arrows). (B) CTA image from a patient in their mid-60s with basilar occlusion and poor posterior circulation collaterals with one small posterior communicating artery visualized on the left (white arrow).
The location of BAO was defined as proximal (proximal occlusion with an involvement of the vertebrobasilar junction to the origins of the anterior inferior cerebellar arteries (AICAs)), mid-basilar (involvement of the segment between the AICAs and the origin of the superior cerebellar arteries), or distal (involvement of segment distal to superior cerebellar arteries).14 Complete recanalization was defined by Thrombolysis in Cerebral Infarction (TICI) scores of 2b or 3.15 The primary clinical outcome was the modified Rankin score (mRS) at 3 months, which was obtained either from a post hospital discharge clinic follow-up or from a hospital visit. Functional independence at 3 months was considered a mRS score of 0–2. Institutional investigation review board approval for this study was granted based on the prospectively maintained University of Tennessee Health Sciences Center Acute Ischemic Stroke Database (10-01003-XP).
Statistical analyses
Continuous variables are presented as mean±SD (normal distribution) and as median with IQR (skewed distribution). Categorical variables are presented as percentages with their corresponding 95% CIs. Statistical comparisons of baseline characteristics and early outcomes were made for patients with good and poor collateral status on CTA. For binary outcomes, the χ2 test, or in the case of small expected frequencies, Fisher’s exact test, was used. Continuous variables were compared using the unpaired t test or Mann–Whitney U test, as indicated. Finally, the association of collateral status with functional independence at 3 months was assessed using multivariate logistic regression models adjusting for age, gender, and baseline stroke severity. The Statistical Package for Social Science (SPSS Inc, V.22.0 for Windows) was used for statistical analyses.
Results
Our study group comprised 21 patients with AIS (age range; 31–84 years, median admission NIHSS score: 18 points, range 2–38) who underwent EVT (table 1). Six patients had proximal BAO, seven had mid-basilar occlusion, and in the remaining eight occlusions were located in the distal basilar artery segment. The etiology of acute BAO was cardioembolism in 10 patients, intracranial atherosclerosis in three patients, cervical dissection with artery to artery embolus in three patients, and cryptogenic strokes in the remaining five patients. Intravenous thrombolysis was administered in eight patients (38.1%). Complete recanalization (TICI 2b or 3) was achieved in 16/21 patients (76.2%) while only 8/21 patients (38.1%) achieved favorable outcome (mRS 0–2). Eleven of 21 patients (52.4%) had bilateral PCOMs, while unilateral PCOM was seen in three patients (14.3%).
Baseline characteristics and outcomes of patients with good collateral score (n=11) versus poor collateral score (n=10)
Early CT changes were noted in 4/13 (31%) patients with poor outcome compared with 1/8 (12.5%) with good outcome; however, this association did not reach statistical significance (p=0.606). No statistically significant difference was noted in mean presenting systolic blood pressure in patients with good collaterals versus poor collaterals (mm of Hg±SD) (160±34 vs 163±26, p=0.857) or patients with good outcome versus poor outcome (148±29 vs 170±28, p=0.100). Newer generation thrombectomy devices (stent retrievers) were used in 5/8 patients with good outcome versus 7/13 patients with poor outcome. There was no difference in outcome rate noted when compared with device type (p=0.673). Conscious sedation was used in 5/8 patients with good outcome versus 7/13 patients with poor outcome (p=1.000). Intra-arterial thrombolysis was administered in three patients. None of our patients was treated with emergent stenting; however, emergent balloon angioplasty was used in three cases. There were no significant differences in the baseline characteristics between the patients with good CS (bilateral PCOM) versus poor CS (unilateral or absent PCOM) (table 1).No difference in outcome was noted when the different locations of BAO were compared. Univariate analysis demonstrated that patients with bilateral PCOMs tended (p=0.261) to have less severe stroke at admission than patients with absent/unilateral PCOM (median NIHSS score 18 vs 27 points). Patients with bilateral PCOMs tended to have higher rates of successful recanalization (90.9% vs 60%, p=0.149) and shorter mean onset to revascularization time (451 vs 676 min, p=0.091) than patients with absent/unilateral PCOM. The degree of neurological improvement during hospitalization was greater in patients with good collaterals (median decrease in NIHSS score 16 points, IQR 2–24) compared with those with poor collaterals (median decrease in NIHSS score 0 points, IQR −18 to −3; p=0.016). Good collaterals were independently (p=0.001) associated with the degree of neurological improvement during hospitalization after adjusting for age, gender, and baseline stroke severity (unadjusted linear regression coefficient 19.3; 95% CI 0.3 to 29.4). The rate of favorable outcome was higher in patients with good collateral status than in patients with poor collateral status (72.7% vs 0%; p=0.001). The association between rate of favorable outcome and collateralization did not retain its statistical significance (p>0.1) in multivariate logistic regression models adjusting for age, gender and baseline stroke severity.
Discussion
The findings of this pilot study indicate that presence of bilateral PCOMs on pretreatment CTA is associated with greater neurological improvement during hospitalization in patients with AISs due to BAO who are treated with EVT in both univariate and multivariate analysis. In addition, univariate analysis showed a higher rate of 3-month functional independence in patients with good collaterals; however, this association did not retain its statistical significance in multivariate analysis, probably owing to the small sample size.
These findings are consistent with previous studies of pretreatment CTA collaterals in patients with anterior circulation stroke successfully treated with EVT.16 Retrograde filling of the basilar artery with bilateral PCOMs provides blood flow to the penumbral tissue, resulting in a lower final infarct volume. The observations of previous transcranial Doppler studies, where patients with BAO who had reversed basilar artery flow through PCOMs had lower NIHSS scores on admission and did not experience neurological deterioration during hospitalization, further support our hypothesis.17 ,18 The presence of a unilateral PCOM also leads to retrograde filling but because of the small number of patients with unilateral PCOM (n=3) in our series its significance could not be properly evaluated. Possibly, patients with a single PCOM have other factors that determine outcome, including the size of the PCOM and the location of the occlusion along the basilar artery. Patients with bilateral PCOMs tended to have shorter onset to revascularization time than patients with absent and unilateral PCOM, which might also have contributed to improved outcome in this subgroup of patients; however, this did not reach statistical significance. The eloquent nature of the brainstem where small infarcts often result in poor mRS grades might also have precluded the ability to demonstrate an outcome difference in this small cohort of patients.
A few studies have shown that patients with distal BAO have a worse outcome, but our series did not find any correlation between the location of the BAO and outcome, similar to the results reported by the ENDOSTROKE study.11 ,19 Other investigators have described angiographic posterior circulation collaterals in patients with BAO, including Moscow and Newton who presented nine patients with BAO.20 Seven of nine patients had collaterals through PCOM and in the remaining two patients, the PCA filled in a retrograde fashion via pial anastomosis between posterior branches of the middle cerebral artery and posterior branches of the PCA. Overall, the good collateral status favored survival in their series. Cross et al19 reported that patients with BAO and collateral filling via the PCOM on DSA had a longer period of symptom tolerance and better neurological outcome after systemic thrombolysis; however, these patients did not undergo EVT.
Alqadri et al proposed a posterior circulation collateral classification based on findings on DSA as follows: grade I, retrograde filling of the basilar artery through the PCA with filling of the superior cerebellar artery; grade II, retrograde filling of the basilar artery through the PCA without filling of the superior cerebellar artery; grade III, bilateral anastomoses of cerebellar or PCAs; and grade IV, unilateral anastomoses of cerebellar arteries or PCAs. They reported that the presence of grade I collaterals appeared to be associated with a lower rate of comatose presentation and higher rates of good outcome.21 The results of Alqadri et al support the findings of our paper that the presence of collaterals is an important predictor of outcome after EVT for BAO. The ENDOSTROKE registry also reported higher rates of recanalization and better outcome after EVT for BAO associated with good collateralization status but they used CS based on American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology (ASITN/SIR) grades, which is mainly validated for anterior circulation large vessel occlusion strokes.11 ,15 Our study differs from these two earlier studies in that we evaluated collateral status using non-invasive CTA at baseline instead of invasive DSA. CTA can be performed quickly in time-sensitive emergencies and it obviates the need to perform complete DSA for evaluation of a patient's vasculature before endovascular intervention.
The limitations of our study need to be acknowledged, including the retrospective design, the limited sample size, and the unblinded assessment of collateral status as well as functional outcomes. Future prospective studies including a larger sample of patients are required to better define the potential association of CTA posterior circulation collateral status with outcome in patients with BAO undergoing endovascular reperfusion therapies.
In conclusion, this study proposes a simple non-invasive classification for posterior circulation collaterals on pretreatment CTA of patients with acute cerebral ischemia due to BAO and provides preliminary evidence for their potential association with early favorable outcomes. Future randomized trials with a large sample size are necessary to validate the results and for definitive conclusion.
References
Footnotes
Contributors NG: data collection for single-center study, drafting of the manuscript. GT: data analyses, drafting of the manuscript. CN: data collection for single-center study, editing of the manuscript. VTD: performed the literature review, contributed to editing of the manuscript. DH, AVA: contributed to editing of the manuscript. AA: performed the literature review, contributed to editing of the manuscript, drafting of the manuscript. LE: conceived the idea for the study, supervised the project.
Competing interests LE has served as a consultant for Stryker Neurovascular, Microvention, and Codman Neurovascular. DH has served as a consultant for Covidien. AA served as a consultant for Covidien, Johnson and Johnson, Siemens, Stryker, and Terumo; and received grants from Siemens and Terumo.
Ethics approval Institutional investigation review board approval for this study was granted based on the prospectively maintained University of Tennessee Health Sciences Center Acute Ischemic Stroke Database. (10-01003-XP).
Provenance and peer review Not commissioned; externally peer reviewed.