Article Text

Abstract
We present our initial patient experience with an innovative temporary bridging device, the Comaneci (Rapid Medical, Israel), to assist in the coiling of cerebral aneurysms. The Comaneci device confers the same benefits as balloon remodeling but without the risks of parent artery occlusion. This alleviates time pressure on the clinician, and could reduce the risk of parent artery thrombosis. Three patients were treated with the Comaneci device. Two patients had acute ruptured posterior communicating aneurysms and one patient was treated electively for a carotico-ophthalmic aneurysm. Excellent occlusion of all three aneurysms was obtained. One patient developed a distal middle cerebral artery clot, that was treated with intravenous aspirin, with minor neurological consequences. These early results show that the Comaneci device can be used to achieve good cerebral aneurysm occlusion. Vessel patency is maintained throughout the procedure with potential advantages over conventional balloon assisted coiling.
- Aneurysm
- Brain
- Angiography
- Intervention
- Device
Statistics from Altmetric.com
Background
Coiling has become the mainstay treatment for cerebral aneurysms since the International Subarachnoid Aneurysm Trial (ISAT) trial in 2002, particularly in the UK and Europe.1 Balloon remodeling has revolutionized coiling by widening the applicability of the technique to difficult aneurysms (specifically wide neck and bifurcation aneurysms).2 This paper presents three cases using the new Comaneci (Rapid Medical, Israel) device for coiling of cerebral aneurysms. This temporary bridging device (figures 1 and 2) has a compliant neck bridge and allows for continuous diameter and radial force adaptation. The user can control the amount of pressure applied on the neck, allowing variable expansion. The wire outer diameter is 80 µm. The metal coverage of the device is variable, however in a straight 3 mm vessel, it will be about 7.5%, with a cell size under these conditions of 1.44 mm2. The Comaneci device provides similar benefits to balloon remodeling while alleviating the associated time constraints.

The Comaneci device.
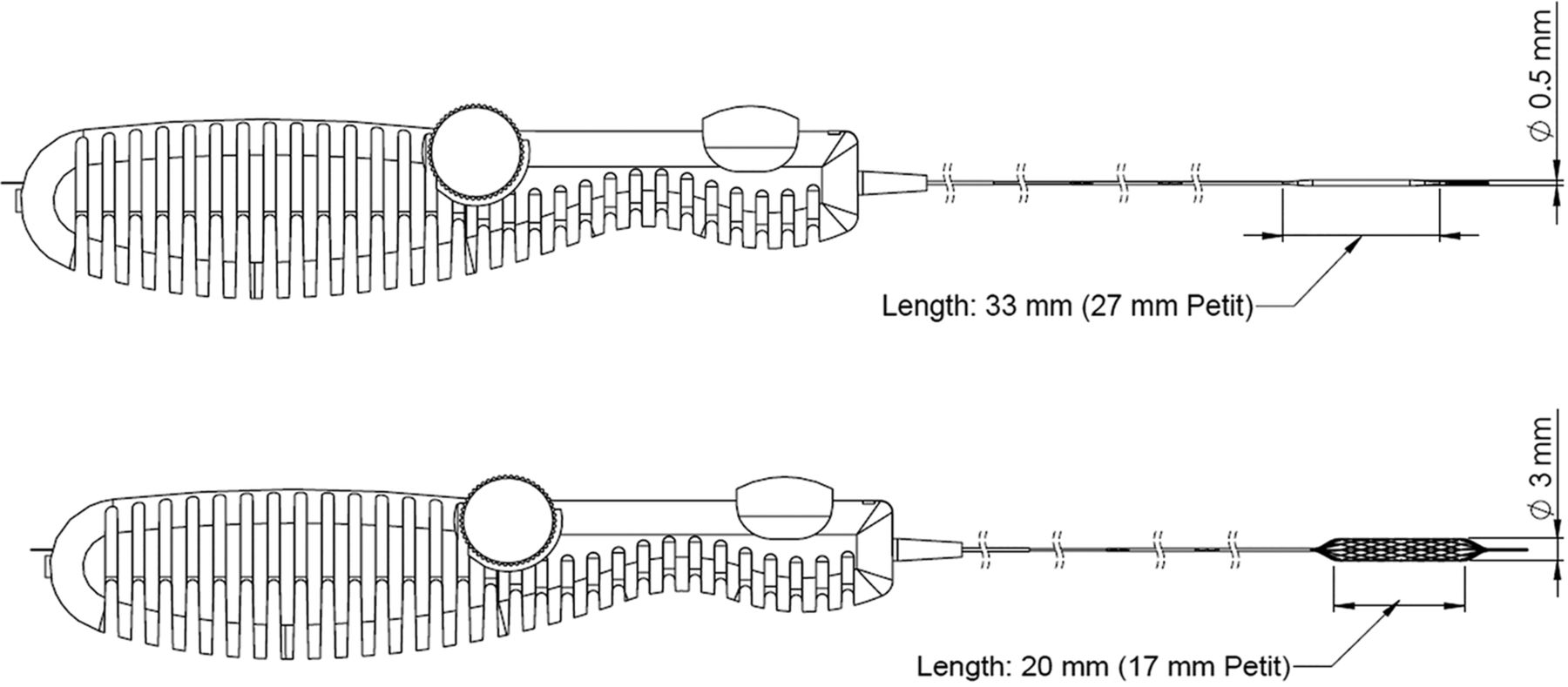
Illustration showing the Comaneci before (top) and after (bottom) deployment. Image used from Rapid Medical (Israel), with permission.
This is the first clinical report on the use of the Comaneci device for the treatment of cerebral aneurysms. Consequently, this experience is invaluable to future practice in the field.
Case presentation
Case No 1
A 50-year-old woman presented with a Word Federation of Neurosurgical Societies (WFNS) grade 1,3 Fisher grade 44 acute subarachnoid hemorrhage. This was secondary to a 7 mm wide necked right posterior communicating artery aneurysm.
Case No 2
A 52-year-old woman presented with an acute WFNS grade 1, Fisher grade 2 subarachnoid hemorrhage secondary to a wide necked 7 mm posterior communicating aneurysm.
Case No 3
A 32-year-old man presented electively with recurrence from a previously treated carotico-ophthalmic aneurysm. The aneurysm had ruptured 3 months previously causing a subarachnoid hemorrhage.
Treatment
Case No 1
A 6 F Benchmark (Penumbra Inc, USA) guide catheter was used for access. Heparin (5000 units) was administered. A Headway 17 microcatheter (Terumo, Tokyo) was used to navigate to the aneurysm. A Headway 21 microcatheter (Terumo) was navigated beyond the aneurysm neck over a Traxcess 14 Ex wire (Terumo). The Comaneci device was partly unsheathed causing advantageous bulging of the mesh into the neck. Ten coils were deployed into the posterior communicating aneurysm (figure 3). The patient developed a distal post central middle cerebral artery (M3) clot during the procedure. This rapidly dissolved with the administration of 500 mg intravenous aspirin. The Comaneci device was inflated for a total of 20 min.

Case No 1. Angiographic images during the coiling procedure of the posterior communicating artery aneurysm using the Comaneci device.
Case No 2
A Benchmark 6 F was used for access. Heparin (5000 units) was administered. A Headway 17 microcatheter (Terumo) was used to access the aneurysm. A Headway 21 microcatheter (Terumo) was used to place the Comaneci device with a Traxcess 14 Ex wire (Terumo). The Comaneci was deployed for 30 min during insertion of 8 coils into the posterior communicating aneurysm (figure 4). A single loop of coil prolapsed into the parent vessel after deflation of the Comaneci device at the end of the procedure. Aspirin 500 mg was administered intravenously at the end of the procedure.

Case No 2. Angiographic images during the coiling of the posterior communicating aneurysm using the Comaneci device.
Case No 3
A 6 F neuron MAX catheter (Penumbra) and 6 F Navien 115 cm catheter (Covidien, USA) was used for access. Heparin (5000 units) was administered. An Echelon 10 microcatheter (Covidien) was used to navigate to the aneurysm and a Reverse 21 Microcatheter (Reverse Medical, USA) was used for deployment of the Comaneci device. The Comaneci device was deployed for 15 min during deployment of five coils into the aneurysm (figure 5). A pipeline device (Covidien), 3.75 mm×14 mm, was also placed through a Marksman to prevent further future aneurysm recurrence.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Case No 3. Angiographic images during the coiling of the carotico-ophthalmic aneurysm using the Comaneci device.
Outcome and follow-up
Good aneurysm occlusion was demonstrated in all three cases. Case No 1 had a post procedure MRI scan that showed a few scattered foci of restricted diffusion in the territory of the middle cerebral artery. There was no area of cortical infarction. At discharge, no significant motor neurological deficits were reported. On review in clinic at 3 months, the patient was found to have mild left-sided weakness (affecting the leg more than the arm). On examination, the Medical Research Council power grade was at worst 4/5. Case Nos 2 and 3 had no neurological symptoms.
Discussion
Currently, the only published literature regarding the Comaneci device, accessed by PubMed, is an animal study by Gupta et al.5 This concludes that the Comaneci device does not cause endothelial injury.5 The benefits of the Comaneci device are that it is a temporary bridging device with no occlusion to distal flow for both sidewall and bifurcation aneurysms. The Comaneci device is compatible with a 0.021 microcatheter and is constructed of radio-opaque nitinol. It is operator controlled by way of a handheld device (figure 2). There are two sizes of the Comaneci device available (table 1).
Comparison between the Comaneci and Comaneci Petit
One of our three cases exhibited a thromboembolic phenomenon. This resolved with intraprocedural intravenous aspirin although the patient had a minor postoperative neurological deficit at follow-up. The source of the distal middle cerebral artery clot is unclear. It may have been from the Comaneci device as the anticoagulation was suboptimal with an activated clotting time of 152 (from 133) after administration of heparin at the start of the procedure. However, there was no clot seen within the device during or after bridging time. Hence a guide catheter or access related thromboembolic cause is also possible.
The present limitations for the device are that a comparatively large microcatheter is needed (0.021) which requires a 0.070 inch minimum internal diameter guiding catheter to allow additional placement of a microcatheter to deliver coils. A smaller delivery catheter for the device could be useful in the future. The shortening of the device once deployed can be minimized, and more sizes could be useful. Nevertheless, this device may prove to be an important addition to the neurointerventionist's armamentarium in successfully treating cerebral aneurysms.
Footnotes
Republished with permission from BMJ Case Reports Published 29 June 2015; doi:10.1136/bcr-2015-011726
Contributors We confirm that all authors meet the criteria for authorship.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.