Article Text

Abstract
Background Mechanical thrombectomy with stent retriever devices is associated with significantly better outcomes than thrombolysis alone in the treatment of acute ischemic stroke. Thrombus aspiration achieves high patency rates, but clinical outcomes are variable. The aim of this study was to examine the effect of different suction conditions on perfusate flow during aspiration thrombectomy.
Methods A computational fluid dynamics model of an aspiration device within a patent and occluded blood vessel was used to simulate flow characteristics using fluid flow solver software. A physical particulate flow model of a patent vessel and a vessel occluded by thrombus was then used to visualize flow direction and measure flow rates with the aspiration catheter placed 1–10 mm proximal of the thrombus, and recorded on video.
Results The mathematical model predicted that, in a patent vessel, perfusate is drawn from upstream of the catheter tip while, in an occluded system, perfusate is drawn from the vessel proximal to the device tip with no traction on the occlusion distal of the tip. The in vitro experiments confirmed the predictions of this model. In the occluded vessel aspiration had no effect on the thrombus unless the tip of the catheter was in direct contact with the thrombus.
Conclusions These experiments suggest that aspiration is only effective if the catheter tip is in direct contact with the thrombus. If the catheter tip is not in contact with the thrombus, aspirate is drawn from the vessels proximal of the occlusion. This could affect collateral flow in vivo.
- Stroke
- Thrombectomy
- Blood Flow
- Catheter
Statistics from Altmetric.com
Introduction
Early restoration of blood flow to the ischemic brain is pivotal to good recovery and improved outcomes in patients with ischemic stroke.1 Recanalization rates with intravenous thrombolysis are poor in patients with occlusion of a large intracerebral artery (30% in basilar artery occlusions, 30% in proximal middle cerebral artery (MCA) occlusions, and 6% in terminal internal carotid artery occlusions).2 Endovascular treatment (EVT) is associated with considerably higher recanalization rates than intravenous thrombolysis.1 The most commonly used methods for EVT are mechanical thrombectomy using a stent retriever device and thrombus aspiration. Recently presented randomized controlled trials have shown significantly better outcomes for mechanical thrombectomy compared with control when stent retrievers were used.3–7 Aspiration devices achieve consistently high recanalization rates (68–100%) but clinical outcomes with aspiration are variable,8 with very poor recovery rates in four studies9–12 and good outcomes in others.13–17 Recanalization alone may not ensure good outcomes if reperfusion is not achieved.18
In vitro experiments can be a useful tool for the study of specific attributes of device performance. Experiments in an in vitro model have previously shown that suction thrombectomy is considerably faster than thrombectomy using a stent retriever device, but is associated with a higher incidence of thrombus fragmentation.19
The aim of this study was to examine perfusate flow patterns during aspiration thrombectomy in an in vitro system to investigate the effects of different suction conditions (flow rate, suction pressure, and distance from the thrombus) on flow in a model of occluded and unoccluded cerebral arteries.
Methods
A mathematical model of blood flow in a blocked cerebral blood vessel was developed. A physical flow model of suction thrombectomy in an occluded and unoccluded vessel was then set up to visualize flow patterns and to assess the effects of different aspiration conditions in vitro.
The mathematical model
A computational fluid dynamics (CFD) model was used to simulate the fluid flow characteristics of a typical catheter used for our experiments. A model of a cylinder within a cylinder was chosen to represent a plain catheter within an artery. The dimensions of the catheter cylinder were based on diameters of the catheters used (see below); approximately 1.4 mm outer diameter and 0.89 mm inner diameter. The artery cylinder was approximately 3 mm in diameter and the distal surface positioned 10 mm from the distal tip of the catheter cylinder. This model assumed laminar flow based on calculated Reynolds numbers that were in the order of thousands. Geometries of the fluid flow system were created, meshed, and run using the fluid flow solver OpenFOAM (OpenCFD Ltd).
The physical flow model
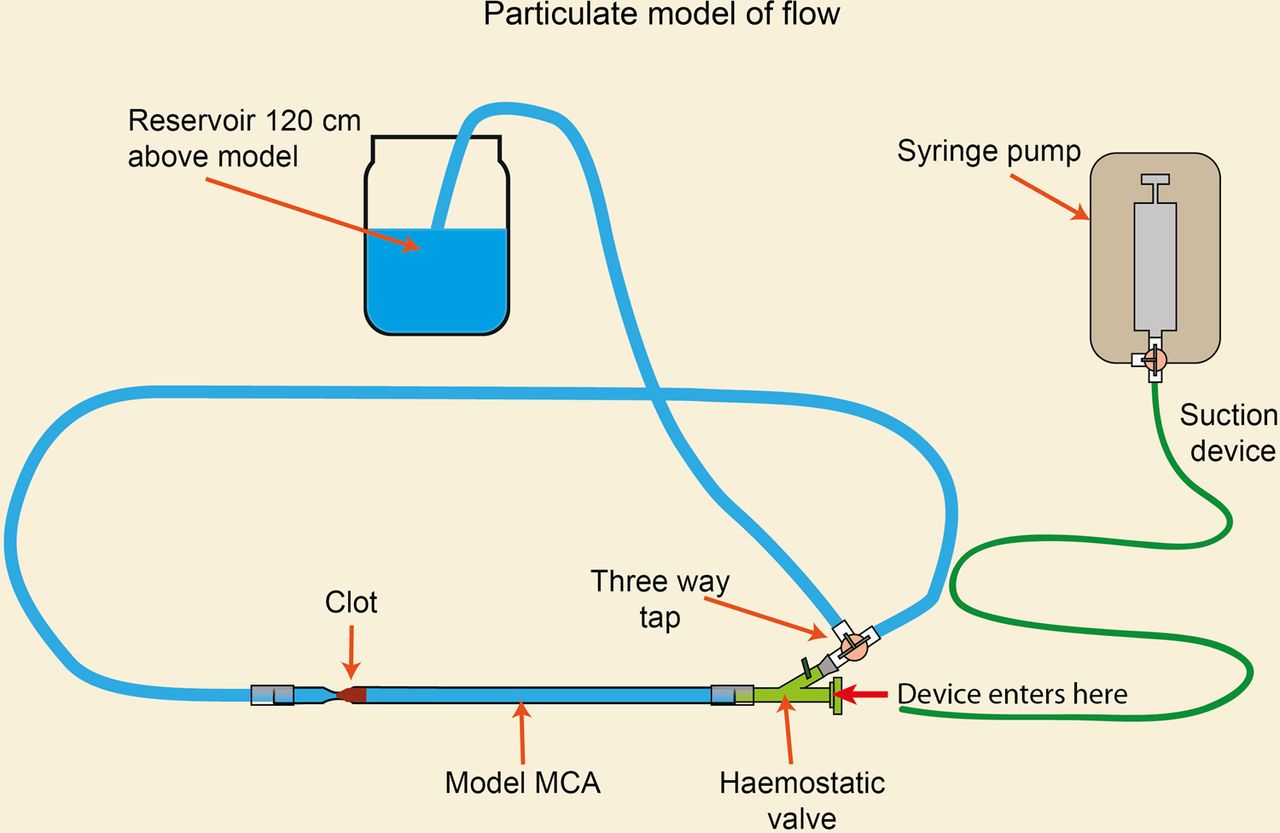
The model was set up as in figure 1 incorporating a glass model of the MCA with an internal diameter of 2.4 mm and a downstream pinch point diameter of 2 mm where the thrombus was placed. A hemostatic valve proximal to the glass model was used to introduce catheters into the system. The system was adapted from a model described previously19 and primed at a mean arterial pressure of 90 mm Hg by elevating the fluid reservoir 122 cm above the model. Two devices were used to create suction within the system: a syringe pump (Fusion 200 Touch syringe pump, KR Analytical Ltd, UK) was used for generating low flow rates and a vacuum pump (Welch Vacuum Technology 2546B-01) for higher flow rates.

Diagrammatic view of particulate system incorporating a glass model of the middle cerebral artery (MCA) with a pinch point for thrombus. The system was primed at a mean arterial pressure of 90 mm Hg by elevating the fluid reservoir 122 cm above the model.
The system was primed with perfusate containing hematoxylin particles to allow visualization of flow patterns. This was prepared as follows: 1 mL of hematoxylin solution (Gill no 3 GHS316, Sigma Aldrich) was added to 800 mL of water and left for 1 h to produce clumps. The solution was stirred and allowed to settle for 30 min repeatedly to obtain a suspension containing smaller particles. This produced a particulate that behaved like a colloid over the time periods of the experiments without significant settling and allowed even small movements of flow to be observed.
Thrombus production
Fresh sheep's blood was obtained from a local abattoir in a closed container. The blood was allowed to clot naturally. After clotting, the blood was cut into small pieces and snap-frozen in liquid nitrogen before being placed in a freezer at −20°C. Thrombi were taken from the freezer in small quantities and allowed to thaw gradually in physiological saline solution at 4°C. On thawing the thrombus was cut down with a scalpel until it weighed 12–14 g after drying on a paper towel. This weight had been arrived at experientially and provided a clot of a size that engaged well within the model system. Once primed, the clot was introduced into the system and pushed to the stricture point using brief flow from the pump. The model was then flushed with perfusate to remove solubilized blood from around the clot to allow accurate visualization.
Flow observation in a blocked system
A catheter was introduced into the system via the hemostatic valve, with the tip at a distance of 1, 2, 2.5, and 10 mm from the clot. Air was removed from the system and the particulate was allowed to equilibrate. At an appropriate point the pump was switched on and the flow in the area of the catheter tip and clot was observed over a minimum of 30 s using a video camera (Samsung, 42X INTELLI-ZOOM, 24 fps). Flow rates used ranged from 5 to 40 kPa using the vacuum pump and 2, 5, and 8 mL/min using the syringe pump. The flow rates were calculated by analysis of video data from the closed system. Fifteen particles were randomly selected and the time taken for each particle to travel 2 cm was timed using a stopwatch.
Catheters
Two catheters were used, a general purpose 4 Fr MC 0.035 inch (0.89 mm) (Kimal, Uxbridge, UK) and a NeuroSlider*17 (0.42 mm) microcatheter (Acandis, Pforzheim, Germany). The size of the catheter was chosen to match the size of the target vessel (2.4 mm) using recommendations for catheter size for currently used catheters in vivo.20 ,21
Results
Mathematical model of suction thrombectomy
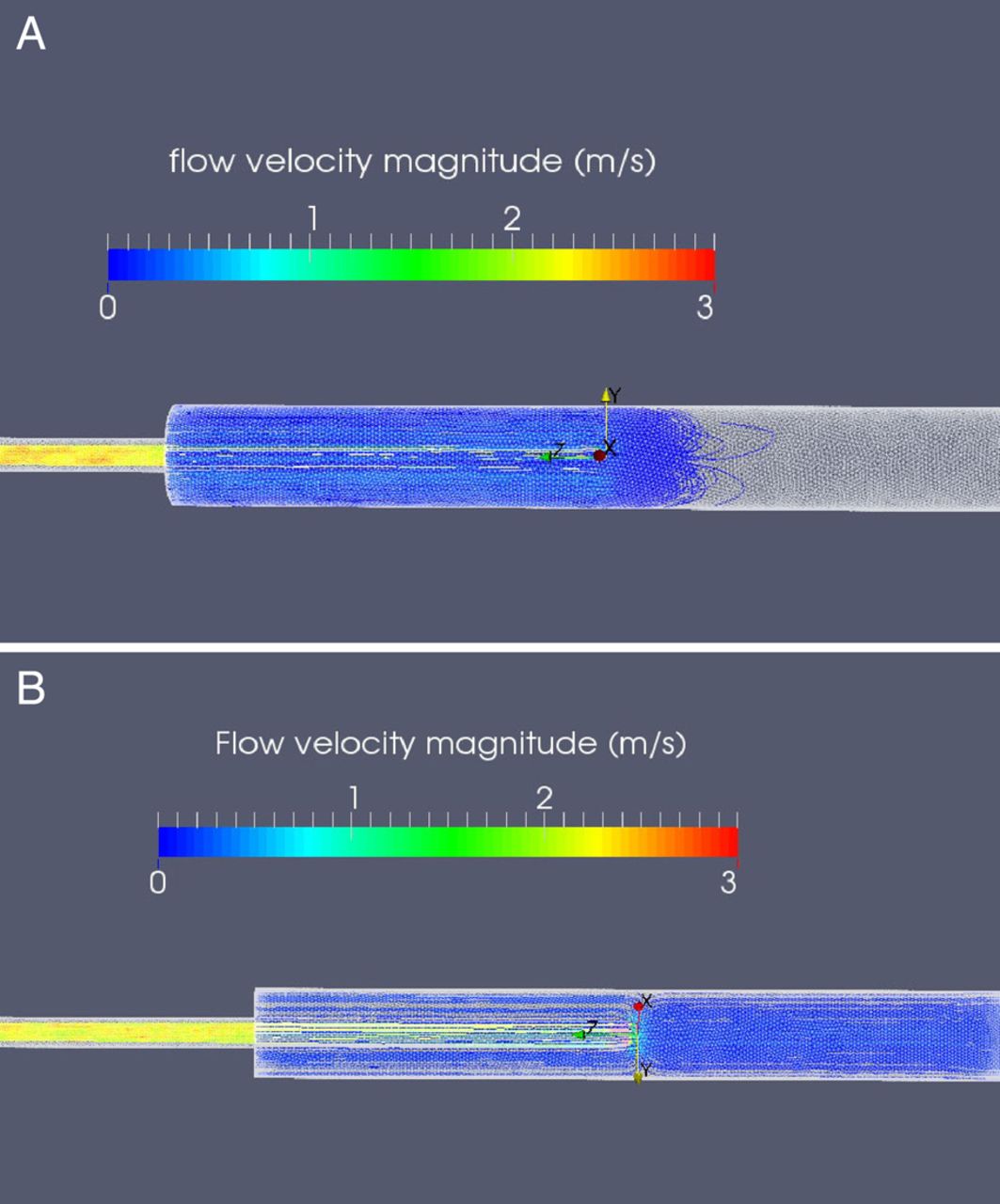
The results of the modeling showed that, in an unobstructed system (cerebral artery not occluded by a thrombus), flow is drawn from upstream of the tip of a device when suction is applied. In an occluded system (cerebral artery obstructed by a thrombus) the mathematical model showed that flow came from behind the tip of the device when suction was applied, and that there was no traction effect on flow distal of the tip. The scaled-up stream tracer plots of an occluded model in figure 2A show torsional movement downstream of the catheter tip but no visible torsional movement from seed points 3 mm upstream of the catheter tip. The only x- and y-direction flow pattern is seen as the fluid flows past the outside of the catheter in the negative z-direction, bending around the distal end of the catheter tip toward the inside of the device. The tracer plots in figure 2B, which come from the unoccluded mathematical model, show clear flow from the same 3 mm seed points upstream of the catheter tip as well as flow from the negative z-direction.

(A) Output from mathematical model showing torsional movement downstream of catheter tip but no torsional movement upstream of the catheter tip. (B) An unoccluded model with clear flow from the same seed points upstream of the catheter tip as well as flow from the negative z-direction.
Physical model
At all flow rates and separation distances, fluid was clearly drawn from behind the catheter as predicted by the mathematical model (figure 2) and not from in front when a clot was present, which is illustrated in figure 3A. As the flow became steady, an area of turbulence was observed in front of the catheter tip and this area of turbulence increased with increasing flow rates (figure 3B). The turbulence had no effect on clot removal at any distance from the catheter; the catheter needed to be touching the clot before suction had any effect. At further separation distances, no clot movement or engagement with the suction catheter was observed in any of the experiments.

(A) Graphical representation of flow as shown in the mathematical model. (B) Area of turbulence in an occluded model seen at all flow rates and separation distances. The turbulence increased with increasing flow rates and did not engage the clot at any distance from the catheter.
When suction was applied to the devices in an occluded model, flow only occurred from behind the tip of the device (figure 4A). When suction was applied to the devices in the absence of a thrombus, flow from the front of the device was restored but there was still a clear but less dominant flow present from behind the catheter tip (figure 4B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Flow only occurred from behind the tip of the device when suction was applied to devices in an occluded model. (B) In an unoccluded model the main flow came from in front of the catheter tip but there was still a clear although less dominant flow present from behind the catheter tip.
Discussion
Mathematical modeling of blood flow in an occluded vessel during suction through a catheter showed an area of turbulence between the clot and the catheter tip with blood drawn from the vessel segment proximal to the catheter tip and no effect of the suction on the clot or on the vessel segment distal to the clot. These findings from our mathematical model are confirmed by in vitro experiments performed in a flow model.
The key finding of this in vitro research is that catheter-based suction only engaged the thrombus if the tip of the catheter was in direct contact with the thrombus. When the thrombus was not engaged in the tip of the suction catheter, suction removed only perfusate and produced no traction forces on the thrombus. Perfusate removed by suction came from behind, for example, the vessel section proximal to the catheter tip. This has potentially significant implications for clinical practice.
After occlusion of a large artery, the ensuing drop in perfusion pressure distally generates a pressure gradient between neighboring arterial fields, resulting in changes in flow direction and rate; collateral flow changes occur almost immediately, within 1–4 s.22 In our experimental model we observed that non-engagement of the suction catheter with the thrombus results in removal of the perfusate proximal of the catheter tip. In a clinical scenario this could lead to flow reversal in the proximal/collateral vessels, leading to a decrease in the perfusion pressure within the ischemic penumbra. This in turn would produce a vicious cycle of further reduction of blood flow in other collateral vessels, thereby incorporating a significant proportion of the salvageable penumbra into the ischemic core. Such flow reductions could be particularly relevant during aspiration in the small-caliber M2 segment of the MCA or in the basilar artery. Placement of the aspiration catheter within the distal M1/proximal M2 could cause flow reversal within the other viable MCA branches including the lateral and medial lenticulostriate perforator vessels. This in turn can cause significant cut-off to the collateral blood supply and pose a particular risk of immediate ischemia to the ganglionic structures supplied by the perforator vessels. In large M1 segment MCA occlusions, a non-engaged suction catheter within the terminal ICA/proximal M1 MCA segment could cause flow reversal within the collaterals supplied by the anterior cerebral artery and enhance the prospect of worsening the ischemia.8
We hypothesize that differences in clinical outcomes of aspiration thrombectomy in published case series may be due to variations in technique between operators. If suction is discontinued and the device repositioned, little or no blood will be removed from the collaterals/cerebral circulation. However, if suction is continued in the same place with continued flow in the suction catheter when the clot is not engaged in the catheter tip, there is no aspiration force on the clot and collaterals may be put at risk. The amount of blood aspirated is limited by the volume of the syringes (30–50 mL) with manual suction. However, if a pump is used, larger volumes of blood can be removed. This may be particularly significant for aspiration in the M1 and basilar artery, as in these areas collaterals are in close proximity to the suction tip and could be put at risk by a reversal in flow.
Our conclusions and the resulting hypothesis are based on mathematical modeling and in vitro experiments in a glass model of the cerebral circulation. Our findings need to be confirmed by in vivo experiments and by observation of clinical scenarios.
The 4 Fr catheter used in these experiments is at the lower range of sizes used for intracranial suction thrombectomy (internal diameter 0.89–1.63 mm) in clinical practice,20 ,23 ,24 but appropriate for the size of the experimental vessel. The diameter of the catheter has no bearing on the conclusions of this work as the results are qualitative rather than quantitative. However, as flow rates increase exponentially with increasing catheter diameter, the observed effects on flow would be expected to be greater with larger bore devices unless the devices are so large as to restrict flow in the vessel.
In vitro simulations and experiments provide explanatory data which can help to optimize interventional technique. Our results suggest that, for aspiration thrombectomy to be effective, the catheter must be in direct contact with the thrombus. Until there is clear evidence that flow reversal by suction is not a problem in vivo, the suction catheter should not be kept in one location for a prolonged period of time during aspiration when there is constant flow as there may be a risk of reducing pressure and flow in the collateral vessels. We would also recommend close monitoring of pump suction to limit the amount of blood removal to an absolute minimum during one suction episode. This may not be relevant in large vessel occlusions without collaterals nearby. Use of wider bore aspiration catheters, which occlude the vessel lumen proximally, could also reduce the risk of affecting collateral flow. This has recently been described as the ADAPT FAST technique.17
Acknowledgments
The authors gratefully acknowledge the support of Dr David Roffe who has helped in editing and proof reading the manuscript and thank Dr G Pearce for the use of the vacuum pump (Welch Vacuum Technology 2546B-01) used in some experiments.
References
Footnotes
Contributors FL: substantial contributions to the conception or design of the work; acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. MS, YY, JM, SN: acquisition, analysis, and interpretation of data for the work; drafting the work for important intellectual content; final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. TW, SN, CJ, IG, CR: interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.