Article Text

Abstract
We describe the process by which we developed a statewide field destination protocol to transport patients with suspected emergent large vessel occlusion to a comprehensive stroke center.
- Stroke
- Political
Statistics from Altmetric.com
Introduction
Embolectomy is now the standard of care for anterior circulation strokes caused by emergent large vessel occlusion (ELVO), and therefore systems of care need to be redesigned to ensure all ELVO patients are offered this highly effective therapy in a timely manner. In Rhode Island, we developed a diversion protocol through a collaborative approach. We summarize our methodology and lessons learned, which may be useful to other regions that are trying to achieve this same goal.
Background
The next revolution in stroke treatment is here. With the results of five positive trials, embolectomy has been established as the standard of care for patients with ELVO in the anterior circulation.1–6 However, the effect of time cannot be understated. The likelihood of a good outcome decreases by at least 10% for every 30 min delay in recanalization.7 ,8 In order to best serve a population, all eligible patients with ELVO need to be transported to a comprehensive level stroke center for embolectomy as soon as is feasible.
Historical context
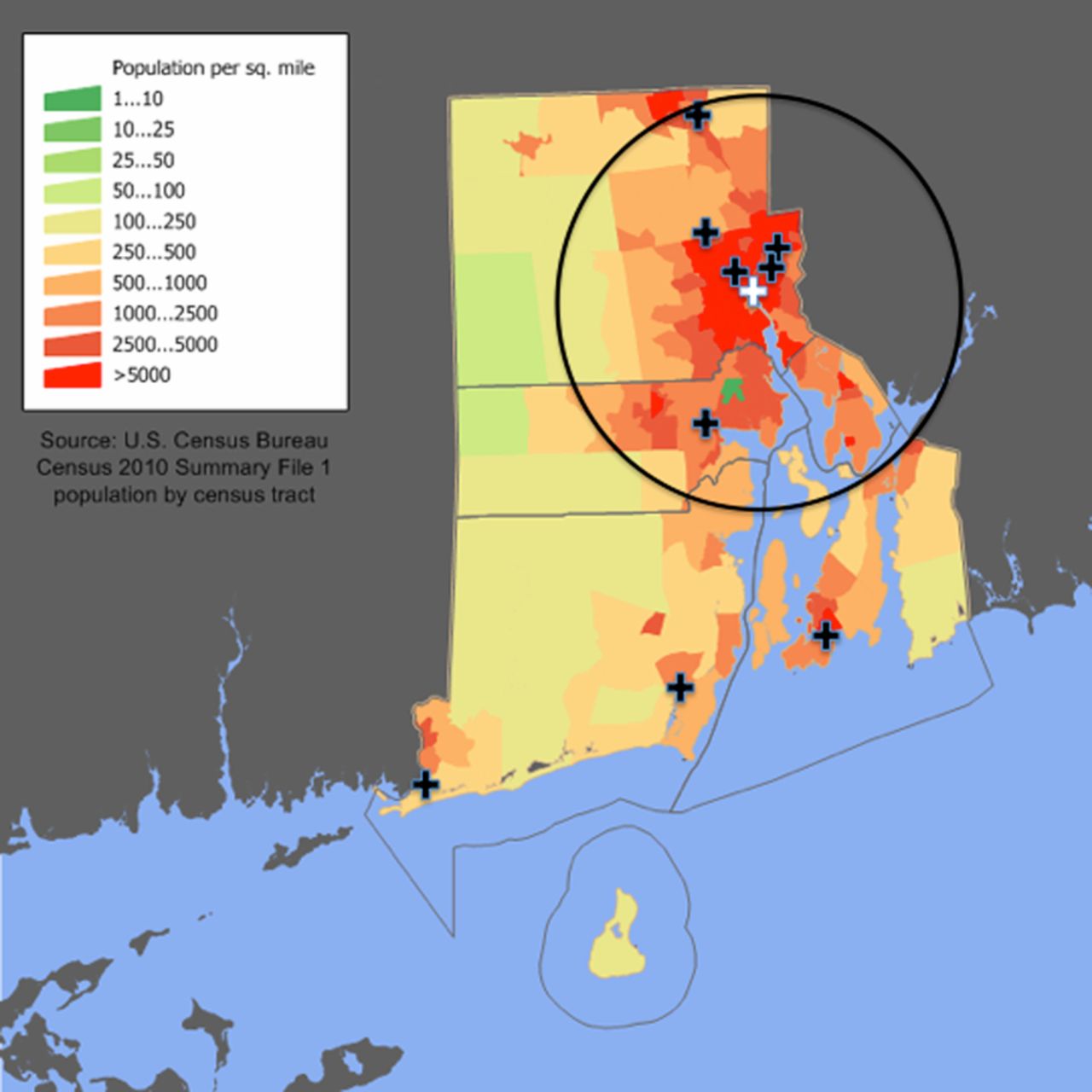
The state of Rhode Island and Providence Plantations is the smallest state in the USA, with an area of just 1212 square miles. However, with a population of 1 055 000, it is second in population density in the USA. There are a total of 11 hospitals with emergency rooms in the state, shown geographically in figure 1. There is one Joint Commission certified comprehensive stroke center (CSC), eight certified primary stroke centers (PSC), and three acute care hospitals which are not certified. The CSC is the only hospital in the state offering 24/7 neurointerventional coverage.
{kind=link}
A map of the state of Rhode Island, with the population density and stroke centers superimposed. The locations of the primary stroke centers (black) and the comprehensive stroke center (white) are noted. In addition, an approximate 30 min drive radius around the comprehensive stroke center has been drawn (circle). Two additional acute care hospitals which are not certified are not shown on the figure.
Emergency medical services (EMS) in Rhode Island are provided by a total of 95 agencies and 4200 licensed providers. The majority of agencies are fire based (52) or third service (16) municipal departments, with the remainder being private or college/university based. The Rhode Island Department of Health, Center for EMS, oversees all 95 agencies and providers. There is a single set of statewide EMS protocols which all providers must adhere to.
In conjunction with the Rhode Island Department of Health, the Rhode Island Stroke Task Force (RISTF) was established in 2004. The task force encouraged and welcomed representation from all acute care hospitals in the state. The goal was to work together to share protocols, data, and improve the care for all patients in the state with ischemic stroke. In April 2008, the RISTF completed and submitted its ‘Report and recommendations to the general assembly’. Subsequently, the task force, working in collaboration with American Heart Association/American Stroke Association staff, drafted a legislative proposal. A lead sponsor from among the House of Representatives was identified. RISTF leaders participated in meetings with legislators and stakeholders, testified on the bill, hosted a stroke roundtable discussion at the State House, and worked through several amendments to the bill language. Stroke survivors were also involved throughout the process, educating legislative leaders and testifying before key committees.
In 2009, the Stroke Prevention and Treatment act was enacted, which mandated that EMS personnel rapidly transported patients with symptoms suggestive of stroke to a PSC.9 This could include bypass of a non-PSC hospital if transport time was within 30 min. The updated EMS protocol reflecting the legislative changes took effect in 2011. This was consistent with the trauma protocol, which had been in place for many years, requiring the transport of serious trauma patients to a certified level 1 trauma center if within 30 min driving distance. The ST segment elevation myocardial infarction (STEMI) protocol, which had a similar provision added in 2010, requires transport to hospitals capable of performing percutaneous coronary intervention if within 30 min transport time.
Changing times
In January 2015, after the results of the Multicenter Randomized Clinical trial of Endovascular treatment for Acute ischemic stroke in the Netherlands (MR CLEAN) were published, a working group from the RISTF met to discuss how to incorporate these new data into the care of stroke patients. Shortly after the February 2015 International Stroke Conference, where results of Endovascular Treatment for Small Core and Proximal Occlusion Ischemic Stroke (ESCAPE), Solitaire With the Intention For Thrombectomy as Primary Endovascular Treatment (SWIFT PRIME), and Extending the Time for Thrombolysis in Emergency Neurological Deficits-Intra-Arterial (EXTEND-IA) were made available, the group again met with the goal of developing a statewide plan to identify ELVO patients and ensure equal access to embolectomy for all. We realized there were two pieces of statewide protocol that needed to be changed:
Update the legislation to recognize differences between PSCs and CSCs.
Update EMS protocols to facilitate getting ELVO patients to CSCs in an expeditious manner.
Legislative change
In order to reflect the changing landscape of stroke care, we amended the original act to incorporate, among others, two key changes:10
Acknowledge there are both PSCs and CSCs, and that certain clinical services (namely dedicated 24/7 coverage with vascular neurology, neurointerventional radiology, neurosurgery and neurocritical care) were only available at CSCs.
Recognize that EMS may transport to the nearest PSC or CSC, as defined by EMS destination protocols.
EMS protocol changes: focus on field diversion
A key component of the changes was the recognition that in Rhode Island, CSCs and PSCs differed in their ability to offer neurointerventional services. As such, the RISTF decided to move forward with a plan to divert patients recognized as having severe stroke in the field to a CSC. It is clear that a ‘drip and ship’ model results in longer treatment times than those transported directly to a CSC, as was shown in the Interventional Management of Stroke 3 (IMS-3) study.11 In keeping with state standards for transport of level 1 trauma patients, stroke patients (to a PSC), and STEMI patients, 30 min drive time was chosen as the cutoff. Patients within 30 min of the CSC would be transported to the CSC, assuming they met a prespecified field severity screen. A major aspect of this was the leadership of the RISTF chair, who recognized that political and economic issues related to disparate healthcare systems needed to be set aside to ensure the best possible care for all patients.
The next step was to decide on which field severity screen to use. The available literature was reviewed, including assessment of the Los Angeles Motor Scale (LAMS), Rapid Arterial oCclusion Evaluation (RACE), and Recognition of Stroke in the Emergency Room (ROSIER).12 ,13 The working group felt that while RACE might have superior sensitivity for cortical signs such as aphasia, neglect, and gaze preference, the simplicity and universal applicability of LAMS made it the most preferable. A LAMS cutoff of ≥4 was designated as a positive field severity screen.12 Patients who had a LAMS score of ≥4 would be transported to the CSC, if within 30 min transport time. It is understood that with time, the prehospital protocol may be modified to use a different scale. The specific scale chosen may be less important than the paradigm that some field severity assessment should be done to screen for possible ELVO.
Since this level of field assessment was new for our EMS providers, we plan to hold an education event shortly after these changes become active. Archived online video based training is also planned. Laminated cards with a description of how to score LAMS have been distributed to most of the EMS units in the state. An important aspect of this education was to ensure that the message to EMS was to screen, rather than simply transport, all strokes to the CSC. Doing so would potentially overwhelm the capabilities of the CSC.
In conjunction with the field assessment of LAMS, we modified the EMS protocol to pre-notify destination hospitals with the patient's last known normal time and LAMS in the field. At the CSC, all patients go directly to CT from the ambulance, and for those with LAMS 4+, CT and CT angiography (CTA) are routinely obtained on the initial trip to the CT scanner, in order to identify ELVO.
For those patients who were more than 30 min transport time from the CSC, or those who were inadvertently transported to a PSC, if they have a LAMS of ≥4, they will receive vessel imaging (preferably with CTA) immediately on arrival to the PSC. We have also suggested that the CSC be notified as soon as ELVO is suspected based on the initial clinical assessment (ie, National Institutes of Health Stroke Scale score of ≥6; or LAMS ≥4), so that transportation can be arranged as the CTA is being obtained. Transport can be canceled if the CTA shows no LVO. A benchmark of 30 min from arrival at the PSC to notification of the CSC has been set.
One final piece was modifying the EMS protocol to facilitate transport of patients currently receiving intravenous tissue plasminogen activator. Previously, the Rhode Island EMS protocol had not allowed such patients to be transported via standard advanced life support ambulances, but instead required either a nurse or physician to accompany the patient. This limitation has now been removed, and allows transport of stroke patients with intravenous tissue plasminogen activator running with a paramedic level transport.
Summary
We have achieved a statewide protocol for rapid identification and transport of potential ELVO patients directly to a CSC. This included several key components:
Collaboration among physicians from different hospitals and healthcare systems.
Establishing a field severity screen for ‘high risk’ ELVO patients.
Having EMS transport ‘high risk’ patients directly to a CSC if within 30 min transport time.
Ensuring that patients who are ‘high risk’ and arrive at a PSC receive vessel imaging rapidly on arrival.
Facilitating the transport of patients with intravenous tissue plasminogen activator infusion to a CSC for intervention.
Similar mechanisms already exist for trauma systems of care. The enormous benefit of embolectomy for patients with ELVO should not be lost due to delayed triage. We believe some of the strategies employed here can be applied elsewhere with similar success.
Acknowledgments
We would like to sincerely thank representative Eileen Naughton, who has been a staunch supporter of the stroke legislation within the state of Rhode Island. In addition, we would like to acknowledge the tremendous assistance of Michelle Barron-Magee on this endeavor.
References
Footnotes
Twitter Follow Matthew Siket at @SiketMD
Contributors All authors were responsible for all of the following: substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of the data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.