Article Text

Abstract
Background and purpose Embolization of thrombus fragments in a new vascular territory is a potential adverse event in neurothrombectomy. This study was performed to evaluate the safety and feasibility of a novel approach combining proximal balloon occlusion and distal aspiration to prevent distal thrombembolic complications.
Methods Patients with ischemic stroke meeting the following inclusion criteria were eligible: occlusion in the anterior circulation, neurothrombectomy using a balloon catheter for proximal flow arrest, and an intermediate catheter for distal aspiration. Pre- and post-interventional Thrombolysis In Cerebral Infarction (TICI) scores were assessed. Clinical presentation at admission and discharge and after 3 months was also evaluated and complications (particularly new thrombembolic events) were recorded.
Results We retrospectively identified 31 patients from our prospectively collected stroke database who met the inclusion criteria. In all patients the initial TICI was 0. A TICI score of ≥2b was achieved in 96.8%. No new thrombembolic complications occurred. The median NIH Stroke Scale score was 19 at admission and 4.5 at discharge. After 3 months, 51.6% of the patients had a favorable clinical outcome (modified Rankin Scale score 0–2) and 19.3% had died.
Conclusions A combination of proximal internal carotid artery occlusion using a balloon catheter and distal aspiration through an intermediate catheter represents a safe and efficient adjunct to mechanical thrombectomy with stent retrievers. In our patient cohort, no new thrombembolic complications were detected.
- Stroke
- Thrombectomy
Statistics from Altmetric.com
Introduction
Endovascular therapy has become a widely used treatment in patients with acute stroke and the clinical benefit has been proven in several studies.1–5 However, there are some issues remaining. During thrombectomy with a stent retriever, the thrombus is mobilized and thrombus fragments can migrate into a new, initially not affected vascular territory as a procedure-related adverse event. This was observed in 5–8% of cases in the TREVO and MR CLEAN trials.1 ,6 In another publication,7 new anterior cerebral artery emboli occurred in 11.4% during M1 recanalization procedures. Although attempts were made to recanalize the anterior cerebral artery, new infarcts were detected in 5.7% during follow-up.
In a recently published paper8 in which the 5 F SOFIA catheter (Soft Torqueable catheter Optimized For Intracranial Access; MicroVention, Tustin, California, USA) was used as an intermediate and aspiration catheter, we reported thrombus migration into a new vascular territory in only 2.6% of patients. This was most likely achieved by positioning of the intermediate catheter tip in the immediate vicinity of the thrombus. Thus, the unprotected stent retriever retraction distance was reduced. Furthermore, lost thrombus fragments could possibly be withdrawn by aspiration through the intermediate catheter lumen. We modified the approach of solely using a distal access catheter by adding a large lumen balloon catheter (8 F Cello balloon guide catheter; Covidien, Irvine, California, USA) for temporal flow arrest of the internal carotid artery (ICA) as a guiding catheter for the intermediate catheter. Here we present the feasibility and safety of this combined approach of simultaneous proximal flow arrest and distal thrombus aspiration.
Methods
Patients
Approval for prospective data collection of all interventional procedures reported in this study was given by the institutional review board. We selected patients with acute ischemic stroke in the anterior circulation when, in addition to the SOFIA catheter (which was used as an intermediate and aspiration catheter), the 8 F Cello balloon catheter was used as a guide catheter. A subgroup of patients (n=16) of a recently published patient series was also included.8 At admission and discharge the NIH Stroke Scale (NIHSS) and modified Rankin Scale (mRS) scores were assessed by detailed physical examination performed by an independent stroke neurologist. The mRS score at 3 months was obtained during a standardized telephone follow-up or at an outpatient visit by a neurologist not involved in the initial treatment. Initial CT scans including non-contrast enhanced CT, CT perfusion and CT angiography or multimodal stroke MRI were performed to prove vessel occlusion and to rule out hemorrhage and advanced ischemic parenchymal damage.
Catheters
As a guide catheter, the Cello balloon catheter was used. It has an outer diameter of 8 F, an inner luminal diameter of 0.075 inch, and a total length of 102 cm. At the distal end, between two radiopaque markers, the catheter has a silicone balloon for flow occlusion with a balloon length of 1 cm.
For our study it was relevant to have an intermediate catheter that can be navigated into distal vessels (eg, the M1 segment) to enable aspiration through the catheter tip in close proximity to the thrombus. We chose the SOFIA catheter, which has a length of 125 cm, an outer diameter distal to proximal of 5 F, and an inner luminal diameter of 0.055 inch.
Treatment protocol
Procedures were performed under general anesthesia or conscious sedation depending on the clinical status of the patient.
Using a transfemoral access, the 8 F Cello balloon guide catheter was placed within the proximal ICA of the affected side. In patients with high-grade ICA stenosis the Cello catheter was placed within the common carotid artery. After angiographic visualization of the thrombus, the intermediate catheter was advanced through the Cello catheter and navigated as close to the thrombus as possible. Usually this was guided by a microwire/microcatheter but, in eight cases, the intermediate catheter was advanced without microwire/microcatheter guidance to the site of the thrombus.
The thrombus was then passed with the microwire/microcatheter. The microwire was removed and a stent retriever (Solitaire FR, Covidien, Dublin, Ireland; Trevo, Stryker, Arizona, USA) was deployed by withdrawing the microcatheter. Subsequently, the Cello balloon was inflated using a 2.5 mL syringe filled with a mixture of contrast medium and normal saline. Prior to thrombectomy, aspiration was applied through the intermediate catheter lumen using a 20 mL or 60 mL syringe. Thrombectomy was then performed under continuous distal aspiration and balloon occlusion of the proximal ICA. After the thrombectomy the balloon was deflated and angiographic runs were performed to control for flow restoration. In cases of persistent occlusion, the procedure was repeated.
Usually there was no aspiration applied to the balloon catheter. Aspiration was performed only in five cases in which the intermediate catheter was occluded with thrombus and withdrawal of the intermediate catheter was required.
Image evaluation
Pre-treatment CT or MR images and post-treatment follow-up CT images 20–36 h after treatment were evaluated using the Alberta Stroke Program Early CT Score (ASPECTS).9
For angiographic evaluation, the angiographic images before thrombectomy and after the final recanalization maneuver were analyzed to determine the Thrombolysis In Cerebral Infarction (TICI) score10 by two experienced neurointerventionalists (SS, MAM) on the basis of consensus. A final recanalization result of TICI 2b or 3 was defined as successful recanalization. Time from stroke onset (if known) and time from the first diagnostic angiographic image to the final recanalization result were recorded.
Complications were also noted, especially thrombus migration into new vascular territories. This was assessed by comparing the first angiographic images visualizing the occlusion with angiographic images obtained at the end of the procedure.
Statistical analysis
Consecutive data were collected in a database and are described as mean (SD). Statistical analysis was performed by GraphPad 5.0 for OSX (San Diego, California, USA).
Results
Patients
Patients were enrolled between February 2014 and April 2015. Thirty-one patients (15 men, 16 women) fulfilled the inclusion criteria for our analysis. Their mean age was 72.3 years (range 29–87). All patients presented with occlusions of the anterior circulation (ICA terminus (n=9); ICA terminus plus middle cerebral artery (n=9); M1 segment (n=10); M2 segment (n=3)) and 18 patients received intravenous recombinant tissue plasminogen activator. The median NIHSS score at admission was 19 (range 4–35). The median time from symptom onset to the first diagnostic angiogram was 206 min (range 92–585). In six patients the exact time of symptom onset was unknown. At discharge the median NIHSS score was 4.5 (range 0–35). After 3 months, 16 patients (51.6%) had a favorable clinical outcome (mRS 0–2), 5 patients (16.1%) were mRS 3, 4 patients (12.9%) were mRS 4, and 0 patients were mRS 5. Mortality was 3% (1/31 patients) at discharge and 19.3% (6/31 patients) at 3 months.
Endovascular procedure and image evaluation
The median time from the first diagnostic angiogram to the final recanalization result was 47 min. TICI 2b/3 was achieved in 30 patients (96.8%). In one patient the final angiogram showed recanalization corresponding to TICI 2a, which was classified as insufficient.
In eight patients, additional ICA stent implantation after the thrombectomy procedure was required due to a high-grade stenosis. A carotid Wallstent with a diameter of 7 mm (Boston Scientific, Marlborough, Massachusetts, USA) was used in all cases.
Pre- and early post-treatment CT and MR images using ASPECTS revealed a median initial ASPECTS of 8 and median follow-up ASPECTS of 7. An example for a neurothrombectomy using proximal flow arrest and distal aspiration is given in figures 1⇓⇓⇓⇓–6.

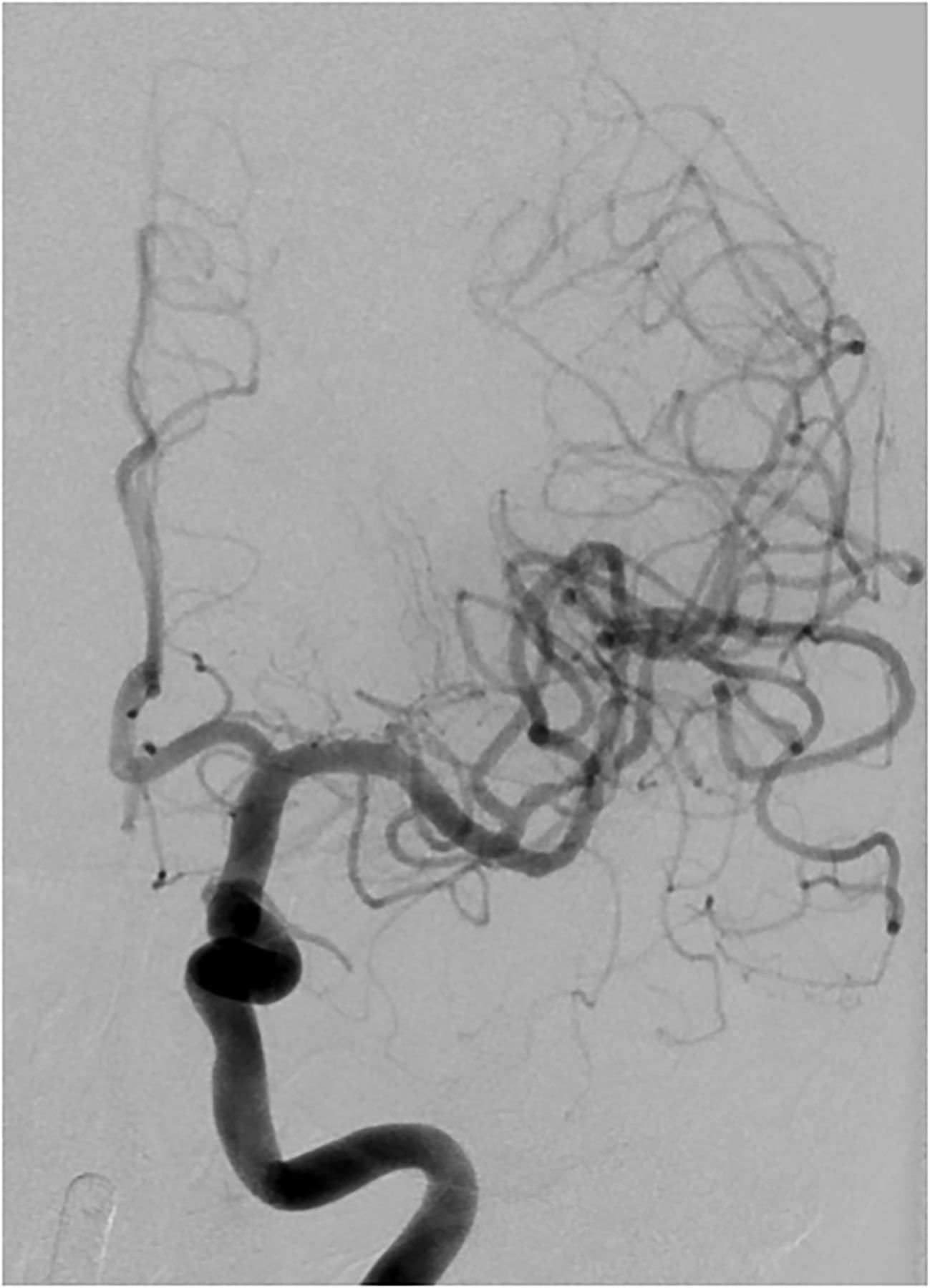
Angiogram (anteroposterior view) of a patient with NIH Stroke Scale score of 16 shows occlusion of the distal left M1 segment and M2 branches.

A Solitaire stent retriever is deployed within the left M1/M2 segment (arrow indicates distal stent markers). The intermediate catheter tip is close to the thrombus (arrowhead).

The balloon catheter is inflated to induce proximal flow arrest. The Solitaire stent retriever (arrow indicates distal markers) and the intermediate catheter (arrowhead indicates catheter tip) are in place.
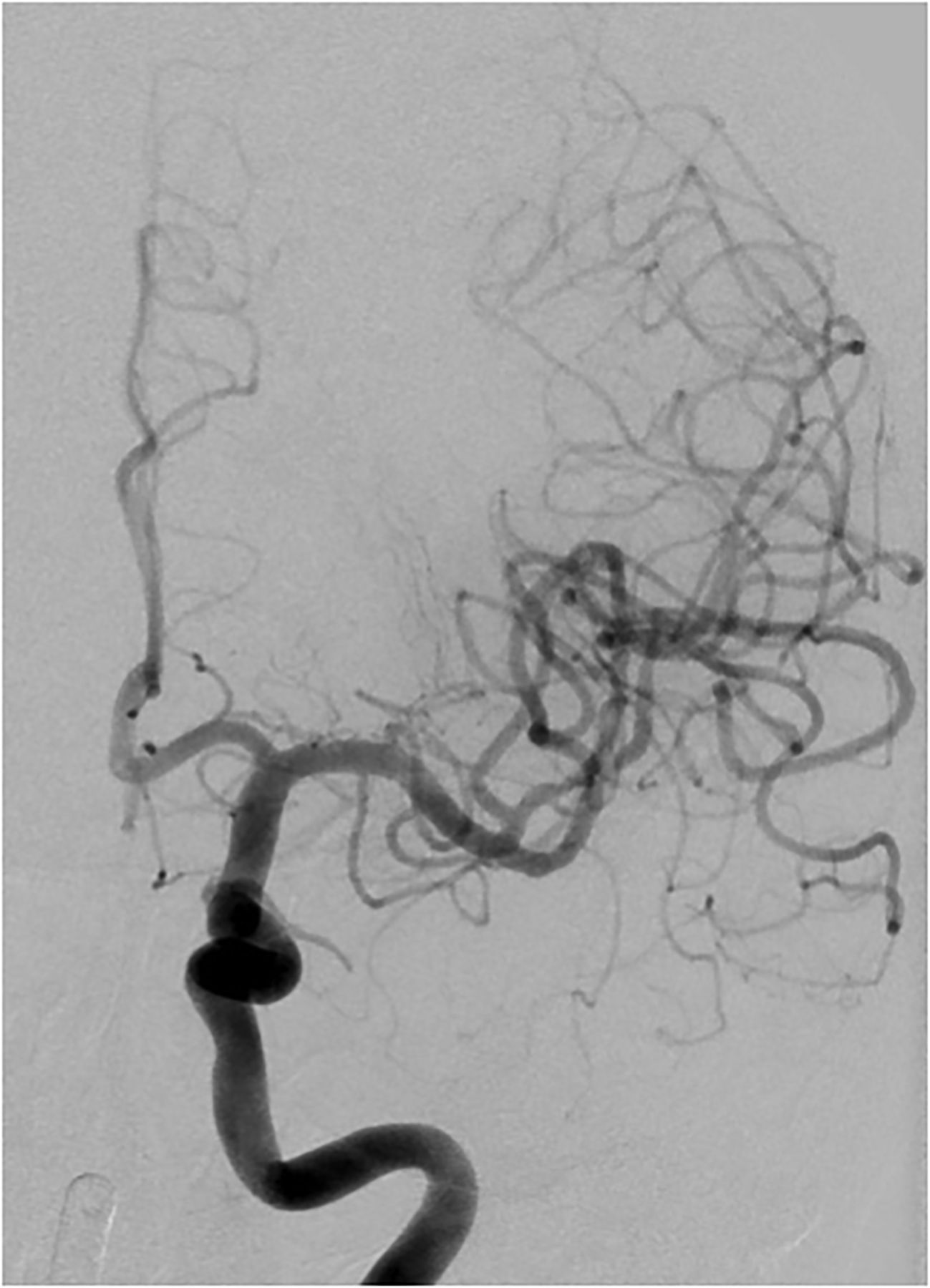
After two thrombectomy maneuvers under simultaneous distal aspiration and proximal flow arrest, the anteroposterior view demonstrates a post-interventional Thrombolysis In Cerebral Infarction score of 3.

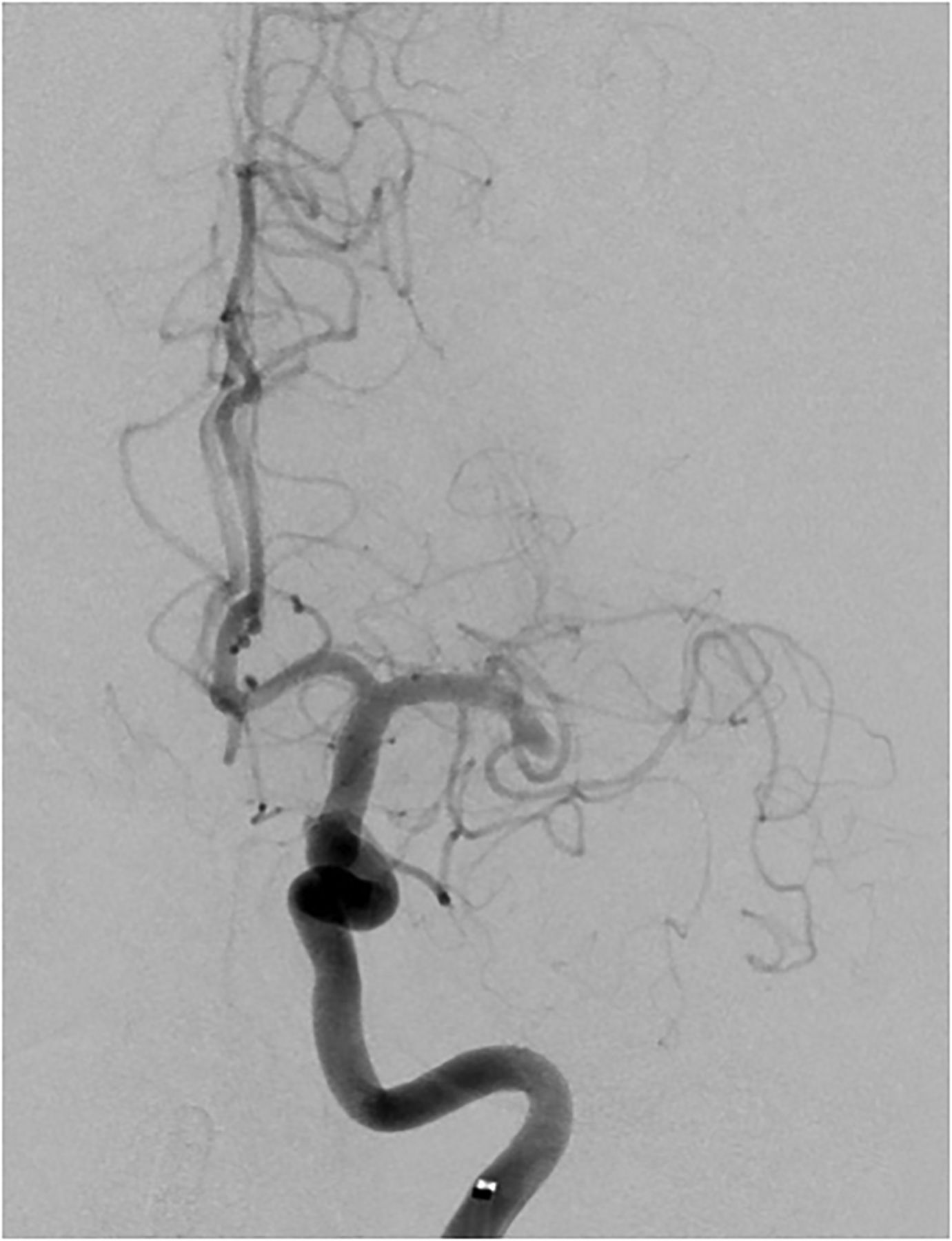
Lateral view showing post-interventional Thrombolysis In Cerebral Infarction score of 3.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Final angiogram of the internal carotid artery showing mild vasospasm but no dissection. After 3 months the patient's modified Rankin Scale score was 1.
Complications
Thrombus migration into a new vascular territory was not observed. Furthermore, there was no dissection related to the guide balloon catheter positioning or intermediate catheter positioning or to the thrombectomy procedure.
In one case the balloon catheter had a leakage and inflation was not possible. The leakage was most likely caused during insertion of the catheter through the sheath. The balloon catheter was exchanged without sequelae for the patient.
No symptomatic intracranial hemorrhage occurred.
Discussion
The clinical benefit of endovascular stroke therapy has been proven in several prospective randomized trials.1–4 However, in a relevant percentage of patients,7 mechanical thrombectomy bears the risk of causing new infarcts in initially unaffected vascular territories through thrombus fragmentation and migration of clot debris. In a study evaluating the complications of stent retrievers,11 new embolic events occurred in 12.5% of patients; 72% of these patients had clinical deterioration and 39% died (whereas the overall periprocedural mortality rate in this study was 18%). Thus, thrombus embolization represents an important adverse event of mechanical thrombectomy with a potentially crucial impact on the outcome.
Basically, stroke treatment can be performed either with a stent retriever or via direct aspiration at the site of the occlusion through a large-bore catheter (a direct aspiration first pass technique, ADAPT12). Stent retrievers can be combined with distal aspiration catheters (Solumbra technique13) and/or with balloon occlusion14 in the cervical ICA.
To perform the ADAPT technique, only navigation into the distal vasculature is required so the ADAPT technique allows fast recanalization in the majority of patients. Turk et al achieved a final TICI score of 2b/3 in 78% of all cases without additional use of a stent retriever. In ineffective cases, adjunctive devices can be used as the catheter tip is already in close proximity to the thrombus. In a recently published study15 the ADAPT technique remained unsuccessful in 29% of cases and the treatment strategy had to be changed to Solumbra as a salvage technique. Thus, an operator performing the ADAPT technique has to be prepared to change to Solumbra in up to one-third of cases.
The ADAPT technique has been reported to be associated with a significantly higher favorable outcome at 3 months than the Solumbra technique and a lower rate of symptomatic intracranial hemorrhage,15 the latter most likely due to less endothelial damage. However, emboli in uninvolved territories occurs more frequently in patients treated with the ADAPT technique. Corresponding to this finding, Turk et al12 reported that fragmentation of the embolus occurred in 10% of all cases with downstream emboli within the initially affected vascular territory. All in all, thrombus migration during endovascular stroke treatment remains an issue.
Strategies to prevent thrombus embolization include distal aspiration through an intermediate catheter and proximal flow arrest via a balloon catheter.
In a recent publication8 we described our initial experience with the SOFIA catheter as an intermediate catheter for distal aspiration. We have modified this approach by adding a large-lumen balloon catheter as a guiding catheter, thus combining the benefit of proximal occlusion and distal aspiration.
As an alternative to the SOFIA catheter, there is another widely used aspiration catheter (5 MAX ACE; Penumbra, Alameda, California, USA). However, the 5 MAX ACE catheter has a taper-shaped configuration with a larger proximal than distal outer diameter (proximal 6 F, distal 5 F). In contrast to this, the SOFIA catheter has the same diameter over the entire length and can therefore be used in combination with the 8 F Cello balloon catheter.
The Navien catheter (Covidien, Dublin, Ireland) is another intermediate catheter which would allow a combination with the 8 F Cello catheter. However, due to its more rigid character, navigation to the thrombus site could be limited.
In the literature there are only studies on either proximal flow arrest or distal aspiration (table 1 provides an overview), but to our knowledge the combination of both strategies has not yet been described.
Summary of previously published studies using distal aspiration or proximal balloon occlusion and comparison with recently published randomized trials (MR CLEAN, EXTEND IA)
There are several in vitro and in vivo studies on the application of balloon catheters for proximal flow arrest to lower the rate of distal embolization.
It is anticipated that inflation of a proximal balloon provides protection against thrombus fragments which otherwise might migrate with the antegrade flow and cause additional infarcts. The theory is that flow arrest or even flow reversal can be created. One concern with the use of a balloon guide catheter might be the delayed flow restoration during the time of balloon inflation. However, using an in vitro middle cerebral artery occlusion model, Chueh et al demonstrated that collateral flow (eg, through the posterior communicating artery) immediately re-established the flow after stent deployment and at least partial flow restoration within the occluded vessel segment despite proximal balloon inflation.16 Furthermore, the risk of thrombus embolization was significantly reduced with the use of a balloon guide catheter because fewer thrombus fragments were generated. In particular, there was a significant decrease in large clot fragments with a size >1 mm.
In a subsequent in vitro study by the same authors, various treatment strategies during mechanical thrombectomy with a stent retriever were compared to assess the reduction of emboli.17 Reduced embolization was found in the balloon guide catheter group and the group with a 5 F distal access catheter for aspiration at the proximal aspect of the clot in the middle cerebral artery. The balloon guide catheter was the best approach to prevent fragmentation of soft elastic clots, and aspiration through the distal access catheter was the most efficient method for reduction of hard clot fragmentation. However, no study group has combined both approaches. The authors concluded that a distal access catheter for aspiration in combination with a balloon guide catheter may be considered for comprehensive reduction of thrombus embolization.
A study by Nguyen et al14 evaluated the influence of a balloon guide catheter on clinical outcome, recanalization success, and reduction of distal emboli when used in combination with stent retrievers. They found that the procedure time was significantly shorter with a balloon catheter and that the rate of TICI 3 reperfusion was significantly higher in the balloon catheter group (53.7% vs 32.5%). The authors hypothesized that proximal flow arrest reduces migration of entrapped thrombus fragments and therefore better reperfusion rates are achievable. However, the rate of emboli in a new vascular territory was similar between the two groups (approximately 5%).
The second technique for prevention of distal embolization is distal aspiration during stent thrombectomy with a compliant intermediate catheter. After introduction of distal aspiration into their middle cerebral artery occlusion treatment concept, Kurre et al7 were able to reduce the frequency of embolization into the anterior cerebral artery territory from 14.6% to 3.3%. Dumont et al18 also showed that thrombus aspiration directly proximal to the occlusion site may reduce distal embolization during stent retriever thrombectomy. In a previous study using distal aspiration through the intermediate catheter lumen,8 we found that thrombus migration into a new vascular territory occurred in only 2.6%, which is lower than other stroke studies (eg, EXTEND-IA trial 6%,5 Kurre et al 11.4%7) and most likely due to the distal aspiration applied via the intermediate catheter.
Thus, both approaches to lower the risk of thrombus migration (proximal flow arrest and distal aspiration) have a proven efficacy. It therefore seemed worthwhile to combine these two promising techniques to further lower the risk of thrombus embolization into a new vascular territory. Disadvantages of combining the two techniques might be the higher complexity of the procedure with a potentially longer procedure time and possible complications caused by the balloon catheter inflation (eg, artery dissection). Furthermore, concerns of using a balloon guide catheter might be the time required to navigate the balloon guide catheter into the proximal ICA, the potentially more complicated handling of the catheter and balloon, and the patient’s tolerance to temporary flow arrest. However, in our study time to recanalization was short despite the use of a balloon catheter and there were no issues with patient tolerance to balloon inflation and flow arrest.
Although the number of patients in the subgroup with this combined approach is limited in our study, it is remarkable that there was no thrombus migration into a previously unaffected vascular territory.
However, the major limitation of our study is the relatively small number of patients and the lack of a control group. Furthermore, thrombectomy devices generate thousands of microemboli in addition to visible clot fragments.16 In our study we cannot assess the presence of angiographically undetectable microemboli which, in addition to large clot fragments, might also lead to an unfavorable clinical outcome.
Another limitation is the lack of a core laboratory in our study. All angiograms were self-adjudicated. It is known that self-adjudicated angiograms often overestimate the final TICI score so it is possible that there is some bias influencing the evaluation of the angiograms.
Conclusion
In our study of 31 patients the combination of proximal ICA occlusion via a balloon catheter and distal aspiration through the intermediate catheter was a safe and efficient complement to mechanical thrombectomy with stent retrievers. The procedure was technically successful in a large number of cases. No macroscopic thrombus migration into a new vascular territory occurred. However, the rate of favorable outcome after 3 months was not higher than 50%.
References
Footnotes
Contributors SS: study conception and design, interventions, acquisition of data, analysis and interpretation of data, drafting of the manuscript. JP: interventions, critical revision of the manuscript. CH: interventions, critical revision of the manuscript. MP: interventions, critical revision of the manuscript. SS: study conception and design, acquisition of data, critical revision of the manuscript. PAR: study conception and design, acquisition of data, critical revision of the manuscript. MB: study conception and design, interventions, critical revision of the manuscript. MAM: study conception and design, interventions, acquisition of data, analysis and interpretation of data, drafting of the manuscript.
Competing interests JP has received travel expenses from Siemens and Stryker. MP has received speaker honoraria or reimbursement of travel expenses from Penumbra, Covidien and Bayer. PAR: None regarding mechanical thrombectomy, has received speaker fee and travel compensation from Covidien, Boehringer Ingelheim, Bayer, BMS, and Daichii Sanyo. MAM has interest in speakers’ bureau or consultant from Acandis, Codman, Microvention, and Phenox.
Ethics approval Ethics approval was obtained from the Ethics Committee, University of Heidelberg.
Provenance and peer review Not commissioned; externally peer reviewed.