Article Text

Abstract
Background There is sparse literature on the natural history of blood pressure (BP) after intra-arterial therapy (IAT) for acute ischemic stroke (AIS).
Methods A retrospective analysis was performed of patients with AIS who underwent IAT without endotracheal intubation for internal carotid artery terminus (ICA-T) or M1 middle cerebral artery occlusion from January 2008 to February 2012. Systolic BP (SBP) values at the beginning (First) and end (End) of IAT and for 36 h after the procedure were collected. Successful recanalization was defined as Thrombolysis In Cerebral Infarction (TICI) 2b–3.
Results Sixty-two patients (14 (22.5%) ICA-T, 46 (74.2%) M1, 2 (3.2%) ICA-T+M1) met the study criteria and 37 (59.7%) achieved successful recanalization. The First and End SBP values were similar in the successful (Group R) and unsuccessful (Group NR) recanalization groups. Taking the whole cohort, End SBP was significantly lower than First SBP, but this decline was significant only in Group R. Subsequently, absolute SBP values in Group R were not significantly different from Group NR. However, when comparing the hourly decline of SBP with First SBP, Group R demonstrated a greater fall than Group NR and the decline was significantly different from hours 8 to 12 post-procedure. The SBP in Group NR then decreased further, and its difference from baseline was similar to Group R from hour 14 onwards. Mean SBP and SBP variability over 36 h were similar between the two groups.
Conclusions SBP falls significantly in patients with AIS with large vessel occlusion who recanalize with IAT. While SBP in non-recanalized patients also drops from baseline, it occurs to a lesser degree and stays higher only for a short period of time before falling to similar levels as in recanalized patients.
- Blood Pressure
- Stroke
- Thrombectomy
Statistics from Altmetric.com
Introduction
Arterial blood pressure (BP) is an important modifiable factor in acute ischemic stroke (AIS). There are limited data on the natural history of BP in AIS, but elevated BP after stroke onset is common. Wallace and Levy1 reported that up to 60% of patients with AIS have a systolic BP (SBP) >160 mm Hg. This can stay elevated for hours to days, but tends to normalize over 24–48 h.2 ,3 Many factors could contribute to an increased BP including pain, discomfort, or intrinsic hypertension. However, the increase in BP could be a compensatory response to maintain cerebral blood flow to the ischemic penumbra.2 ,4 This theoretic explanation would suggest that BP should decline if occluded vessels are recanalized compared with patients in whom the vessels remain occluded. Data supporting this hypothesis come from intravenous (IV) thrombolysis studies, which have demonstrated higher SBP in patients treated with IV recombinant tissue plasminogen activator (tPA) who had persistent vessel occlusion as assessed by ultrasound.5 Studies have also demonstrated a spontaneous reduction in BP after recanalization following treatment with IV tPA.6 This was also demonstrated in patients who underwent intra-arterial therapy (IAT) for AIS, where SBP remained elevated longer when recanalization failed than when it succeeded.7
There are few data on BP management after IAT for AIS. Current recommendations suggest treatment targets similar to those for post-thrombolysis patients in the immediate post-procedure period (SBP <180 mm Hg, diastolic BP <105 mm Hg), irrespective of recanalization status.8 The objective of this study was to investigate the changes in BP in patients with AIS with documented internal carotid artery (ICA) or middle cerebral artery (MCA) occlusion who underwent IAT, and to compare the results based on recanalization status in the short-term post-procedure period.
Methods
Subjects
This study was conducted after Institutional Review Board approval. Our institution's prospectively maintained database of AIS interventions was retrospectively reviewed to identify all patients who underwent IAT for AIS between January 2008 and December 2012. Subjects aged ≥18 years of age who had a pre-intervention catheter angiogram showing Thrombolysis in Cerebral Infarction (TICI) grade 0 or 1 occlusion of the ICA terminus or M1 MCA were included in the analysis. To minimize the effect of anesthesia on hemodynamics, only patients who underwent IAT without requiring endotracheal intubation were included. The decision for IAT was made based on previously published protocols from our institution,9 and included only patients with large vessel occlusion.
Demographic data including age, gender, and vascular risk factors including presence of hypertension at admission, National Institutes of Health Stroke Scale (NIHSS) scores on admission, and IV tPA use were collected. All patients who underwent IAT received an arterial line from which BP was recorded. SBP was collected just prior to the start of the procedure (First SBP), at the end of the procedure (End SBP), and then at hourly intervals for 36 h. The initial two BP readings were recorded in the neurointerventional suite and were obtained from the Anesthesia Record Keeping System. All patients who underwent thrombectomy were initially admitted to the neurological intensive care unit and then transitioned to a neurological step-down unit or regular nursing flow. BP readings were collected for 36 h post-procedure from electronic records chart review. Recanalization was graded using the TICI score and successful recanalization was defined as TICI grade 2b–3.10
For patients who received IV tPA, BP was checked every 15 min for 2 h after starting the infusion, then every 30 min for 6 h, then every 60 min until 24 h after starting IV thrombolysis. For patients who did not receive IV tPA, BP was checked every 60 min until 24 h. From 24 to 36 h, all patients had BP checked every 120 min. The BP target for patients who underwent thrombectomy was SBP ≤180 mm Hg.
Statistical analysis
Statistical analysis was performed using JMP V.10. Univariate analysis of categorical variables was performed with the Fisher' exact test and the Student t test was used for continuous variables in comparing patients who achieved recanalization (Group R) versus those with unsuccessful recanalization (Group NR). A p value of <0.05 was considered statistically significant.
Results
A total of 62 patients met the inclusion criteria. This included 14 (22.5%) patients with ICA-T occlusion, 46 (74.2%) with M1, and 2 (3.2%) patients with ICA-T and M1 occlusions with pre-intervention TICI 0/1 flow. The entire cohort consisted of 37 (59.6%) women with mean age 69.4±14.1 years and median NIHSS score 14.5 (IQR 9–19). Median admission Alberta Stroke Program Early CT Score (ASPECTS) was 8 (IQR 6–10). Twenty-four (38.7%) patients received IV tPA at a median time from symptom onset of 136 min (IQR 104.5–156). Thirty-seven (59.7%) patients achieved successful recanalization and 12/52 (23%) achieved a 30-day good outcome. Table 1 summarizes the univariate analysis comparing patients who achieved successful recanalization (Group R) with those in whom recanalization was unsuccessful (Group NR). Patients who achieved successful recanalization had a higher baseline CT ASPECTS score (8.3±1.6 vs 7.4±1.9, p=0.046), higher rate of IV tPA administration (51.5% vs 20.8%, p=0.014), and higher rates of good outcome (32.3% vs 9.5%, p=0.045). There was no difference between the two groups with regard to the remaining baseline characteristics.
Baseline demographics, treatments, and BP variables
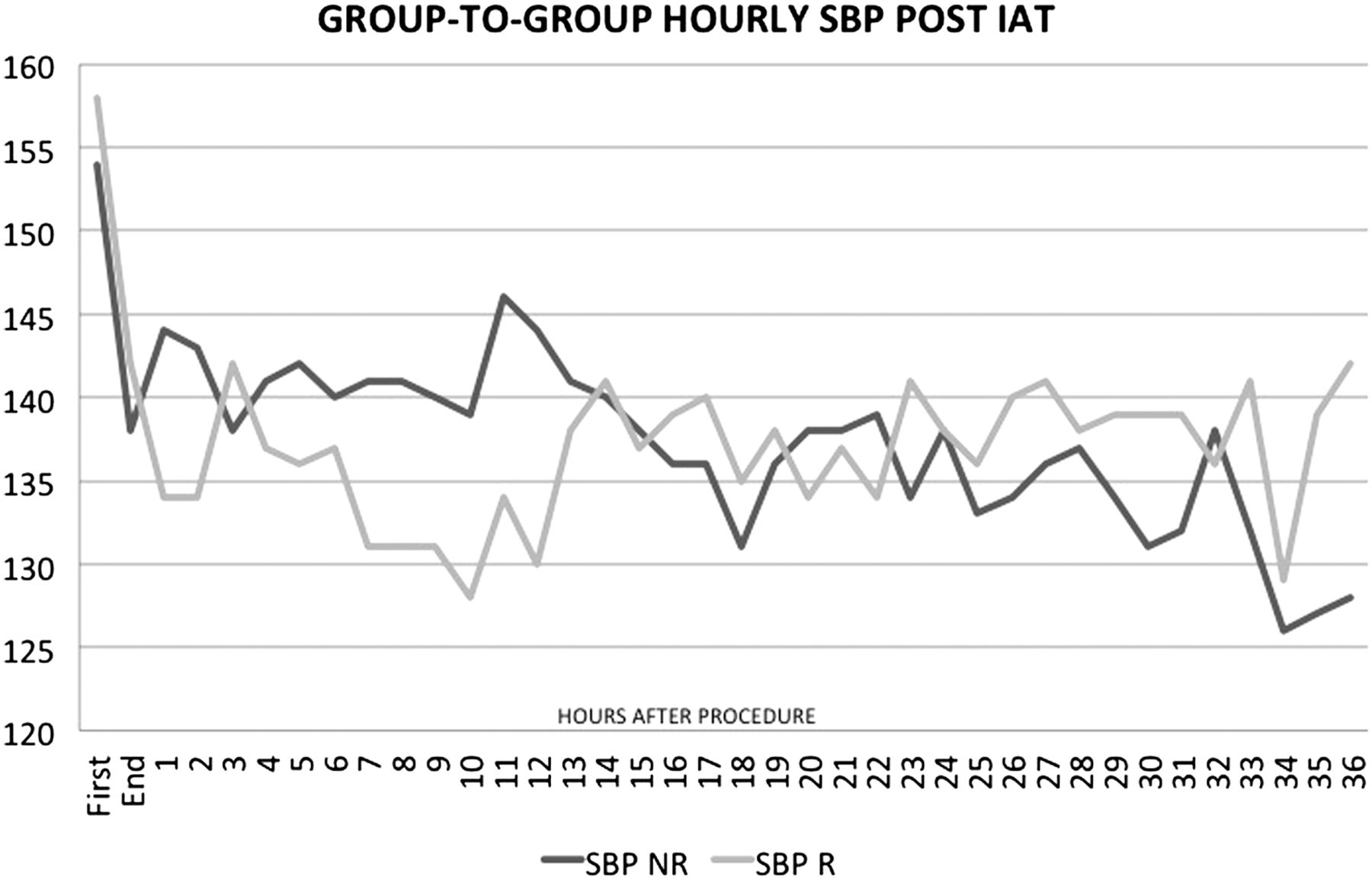
Forty-five (72.6%) patients were hypertensive (SBP >140 mm Hg) based on first measured BP in the hospital (Admission SBP), and there were a similar number of patients in both groups who were hypertensive. First SBP and End SBP were similar between the two groups. Taking the whole cohort, the SBP dropped significantly at the end of the case compared with the first SBP (156.5±24.4 to 139.9±27.9, p=0.002). Comparing groups, this decline was only significant in the recanalization group. In Group R, SBP fell from 158.4±24.6 to 142.2±22.4 (p=0.005) while, in Group NR, SBP fell from 154.3±23.8 to 138.3±35 (p=0.066). Figure 1 demonstrates the trend in hourly SBP values between groups post-procedure (see online supplementary table S1). While absolute SBP values in Group R were generally lower until hour 12, none were significantly different from Group NR except at hour 12. From hour 14 onwards the curves crossed and SBP values in both groups were similar. Figure 2 demonstrates the trend in hourly SBP difference from First SBP (ie, SBPn – First SBP, where ‘n’ is the hour post-procedure) (see online supplementary table S2). After recanalization there was greater fall in SBP from baseline compared with non-recanalized patients, and the decline was significantly different from hours 8 to 12 post-procedure. The SBP in Group NR decreased further from baseline after that, and the decrease in SBP was similar to Group R from hour 14 onwards. The mean SBP over 36 h was similar between the two groups. The SBP variability over 36 h, reflecting the within-subject SD of all recordings, was also similar between the groups.
Supplementary tables

Trend in hourly systolic blood pressure (SBP) values between Group R (Thrombolysis In Cerebral Infarction (TICI) 2b–3) and Group NR (TICI 0–2a). (x axis shows time in hours post-procedure, y axis shows SBP in mm Hg).

{kind=link}
{kind=link}
Trend in hourly systolic blood pressure (SBP) difference from First SBP (ie, SBPn – First SBP, where ‘n’ is the hour post procedure). (x axis shows time in hours post-procedure, y axis shows SBP difference in mm Hg).
Discussion
In this study we have confirmed reports of a decline in BP in patients with AIS with large vessel occlusion after recanalization.6 ,7 When comparing patients based on recanalization status, those who recanalize have a larger decrease in SBP from baseline than patients who do not recanalize. However, the SBP in patients who do no recanalize also falls from baseline, but to a lesser degree and stays higher for a short period of time before falling to similar levels as in recanalized patients.
Mattle et al7 looked at the relationship between SBP and the patency of the initially occluded vessel in AIS. Time points for BP measurement include time of admission and 1 h and 12 h after IA thrombolysis. The authors found that SBP measured at 12 h declined significantly faster when the vessel was recanalized than when recanalization failed. To the best of our knowledge, this is the only other study that has investigated the short-term relationship between BP and recanalization after IAT. Similar studies have been described with IV thrombolysis. Nagaraja et al11 analyzed 17 patients who were treated with IV tPA and had pretreatment and 24 h post-treatment MR angiography (MRA) scans, with pretreatment proximal MCA occlusion. The results showed that a decline in SBP of ≥20 mm Hg at 24 h together with a concurrent improvement in NIHSS was more likely to be associated with recanalization. However, a decline in SBP alone was not significantly associated with recanalization. Similarly, Yeo and colleagues did not find any significant association between a decline in SBP of ≥20 mm Hg and vessel recanalization on 24 h CT angiography (CTA) for patients with proximal MCA occlusion (n=90) and ICA occlusion (n=66) who were treated with IV tPA.12 Another recent study by Yan et al13 evaluated BP at shorter intervals in 161 patients with AIS who received IV tPA, with pretreatment documentation of large vessel occlusion and 24 h CTA or MRA for recanalization. BP was measured at 15 min intervals in the first 2 h after IV tPA treatment and a 'sudden drop in BP (defined as decline in SBP of ≥20 mm Hg between two continuous BP measurements) was independently associated with recanalization. This predictive ability was better in patients with ICA or MCA occlusion. In addition, the BP of all 161 patients decreased significantly from admission to 12 h after thrombolysis. The absolute decline in SBP from admission to 6, 12, 18, and 24 h after thrombolysis was larger in patients with recanalization than in those without recanalization. In an earlier report, Delgado-Mederos studied 80 patients with MCA occlusion who were treated with IV tPA, and recanalization was assessed at 6 h after symptom onset with transcranial Doppler.6 Multiple hourly SBP values were measured for 24 h. The authors reported a significant decrease in SBP level from admission to 24 h after treatment in all patients. When recanalization status was accounted for, the fall in SBP was significant in recanalized patients but not in patients with persistent occlusion.
The above studies have some important limitations. Single time point measures of BP, such as during admission and at 24 h, are likely to be inferior to continuous measurements since BP is a dynamic variable and experiences fluctuations in the immediate stroke period. Second, it is unclear in the IV thrombolysis studies the exact time at which recanalization occurred, which could have a bearing on the BP measurements. In our study, the knowledge of recanalization status at the termination of the case and serial measurements for 36 h resolves some of these limitations. However, the question continues to remain complex and the relationship between BP and recanalization is still affected by multiple factors such as arterial reocclusion, hemorrhagic transformation, failure of collaterals, or progression of ischemia and cerebral edema.
We attempted to collect details of ‘as needed’ (PRN) IV antihypertensive medication administration during the time period of the study but could not reliably collect this information and correlate it with BP changes post-procedure. However, none of the patients received continuous infusions of IV antihypertensive vasopressor medications during this period. Despite this limitation, we do not believe the BP trend in our patients was significantly affected by medications. The highest recorded SBP values in Groups R and NR were 158 mm Hg and 154 mm Hg, respectively, and it is unlikely that many patients in either group were treated with antihypertensives since these levels were well below the target SBP range of 180 mm Hg. In addition, the SBP curves after hour 14 were remarkably similar in both groups, suggesting that this represents the natural course of BP.
The findings of our study may have important clinical implications. The BP differences based on recanalization may be secondary to the body's endogenous drive to increase BP to maintain cerebral perfusion. However, these differences were early and short-lived. In non-recanalized patients it may be futile to augment BP with IV fluids or pressors beyond 12–14 h in patients who do no recanalize after IAT. The same could potentially be extrapolated for patients with large vessel occlusion treated with IV tPA who do not undergo IAT, where it may be futile to augment BP after a similar time period after treatment in presumed non-recanalized patients who do not improve clinically or demonstrate a spontaneous decline in BP.
Conclusion
The SBP falls significantly in patients with AIS from large vessel occlusion who recanalize with IAT. While the SBP in non-recanalized patients also falls from baseline, it occurs to a lesser degree and stays higher only for a short period of time before falling to similar levels as in recanalized patients.
References
Footnotes
Competing interests None declared.
Ethics approval Ethics approval was obtained from the Cleveland Clinic Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Contributors SJ, KU, MSH: conception and design, acquisition of data, analysis and interpretation of data; drafting the article or revising it critically for important intellectual content; and final approval of the version to be published. WH: acquisition of data, drafting the article or revising it critically for important intellectual content; and final approval of the version to be published.