Article Text

Abstract
Background and purpose Non-saccular aneurysms of the posterior fossa are an uncommon pathology with no clear treatment strategy. The use of flow-diverting stents (FDS) has had mixed results. We sought to evaluate our experience of FDS for the treatment of this pathology.
Methods We retrospectively reviewed our database of prospectively collected information for all patients treated only with flow diversion for an unruptured non-saccular aneurysm of the posterior circulation between February 2009 and April 2016. The aneurysms were classified as dolichoectasia, fusiform or transitional, and imaging characteristics including maximal diameter, disease vessel segment, MRI features (intra-aneurysmal thrombus, T1 hyperintensity in the aneurysmal wall, infarctions in the territory of the posterior circulation, and mass effect) were recorded alongside clinical and follow-up data.
Results We identified 56 patients (45 men) with 58 aneurysms. The average age of the patients was 63.5 years. Twenty-two patients were symptomatic from the aneurysms at presentation. The majority of the lesions were vertebrobasilar in location (44.8%) with isolated vertebral lesions representing 29.3% of aneurysms. Transitional aneurysms were the most common (48.2%). The mean maximal diameter of the aneurysms was 11 mm. Angiographic exclusion of the aneurysms was seen in 57.4% of aneurysms with follow-up (n=47). During the follow-up period nine patients died.
Conclusions Treatment of non-saccular aneurysms of the posterior fossa is technically possible. Early treatment, particularly of the fusiform and transitional subtypes, is recognized, as is treatment prior to the development of symptoms. A ‘watch and wait’ strategy with regular imaging follow-up could be employed for asymptomatic dolichoectasia.
- Aneurysm
- Stent
- Stroke
- Flow Diverter
- Posterior fossa
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
In 1922 Wells was the first to describe a non-saccular aneurysm of the basilar artery upon surgical exploration in a patient with obstructive hydrocephalus and paresis of cranial nerves VI–VIII,1 with further reports published later by Walter Dandy2 as well as Greitz and Lofstedt.3 Non-saccular aneurysms of the posterior circulation are uncommon with an incidence of less than 1%. In an autopsy series from Columbia University the incidence of aneurysms was 0.1%,4 and a similar series from a VA hospital series showed an incidence of 0.07%.5 These aneurysms can manifest with a variety of different symptoms ranging from asymptomatic and incidental findings on routing imaging, posterior circulation ischemic strokes, brainstem compression, cranial nerve palsies (most commonly V–VIII),6 obstructive hydrocephalus, and hemorrhage.7–14
The natural history of these lesions is fateful and mortality of up to 30% has been reported,14–16 with a recent review by Shapiro et al17 suggesting that mortality could be even higher at 43%. If left untreated they carry significant morbidity with growth of these aneurysms seen in 46% of patients over a median interval period of 8.5 years.6 ,10 ,18 ,19 According to the findings of Mangrum et al18 this particular phenomenon is associated with a 5.7 times increase in mortality relative to those patients with aneurysms that were stable.
It is not surprising then that the advent of endoluminal reconstruction with flow-diverting stents (FDS) was met with much fanfare and the promise of providing a potential new treatment option for a group of patients with a generally poor prognosis and few other suitable treatment options. Unfortunately, this initial optimism quickly reverted to pessimism after preliminary experiences suggested that the use of FDS in the posterior circulation would not yield similar results to those in the anterior circulation.20–25 However, more recent reports have shown promise—for example, in the paper by Phillips et al26 there were no treatment-related deaths and an overall morbidity of 9.4%, with all patients having a good functional outcome (modified Rankin Scale (mRS) score of 1), being independent, and returning to work.
In this study we present our single-center experience of the use of FDS in non-saccular posterior circulation aneurysms, which we believe is the largest series to date of non-saccular aneurysms of the posterior circulation treated with flow diverters and the first to detail the specific locations and morphological features, which have been shown to be important in prognosis.
Methods
Patient population
We retrospectively reviewed our prospectively maintained database and identified 56 patients with 58 unruptured intradural fusiform aneurysms of the posterior circulation who were admitted to our institution for endovascular treatment between September 2009 and April 2016. For each patient we recorded demographic data, clinical presentation, location of the aneurysm, therapeutic intervention, immediate angiographic and clinical result, and clinical and radiological follow-up information.
Classification of non-saccular aneurysms
All aneurysms of non-saccular appearance arising from the V3/4 segment or distally within the posterior circulation and not representing acute dissecting pseudoaneurysms were included in the analysis. This was determined through the clinical presentation and the radiological appearance. The imaging features used to exclude potential dissecting aneurysms included T1 hyperintensity on fat suppressed MRI (in those patients who underwent MRI), visualization of a dissection flap, the ‘bead and string’ sign, and narrowing of the parent artery proximal to a dilated segment.
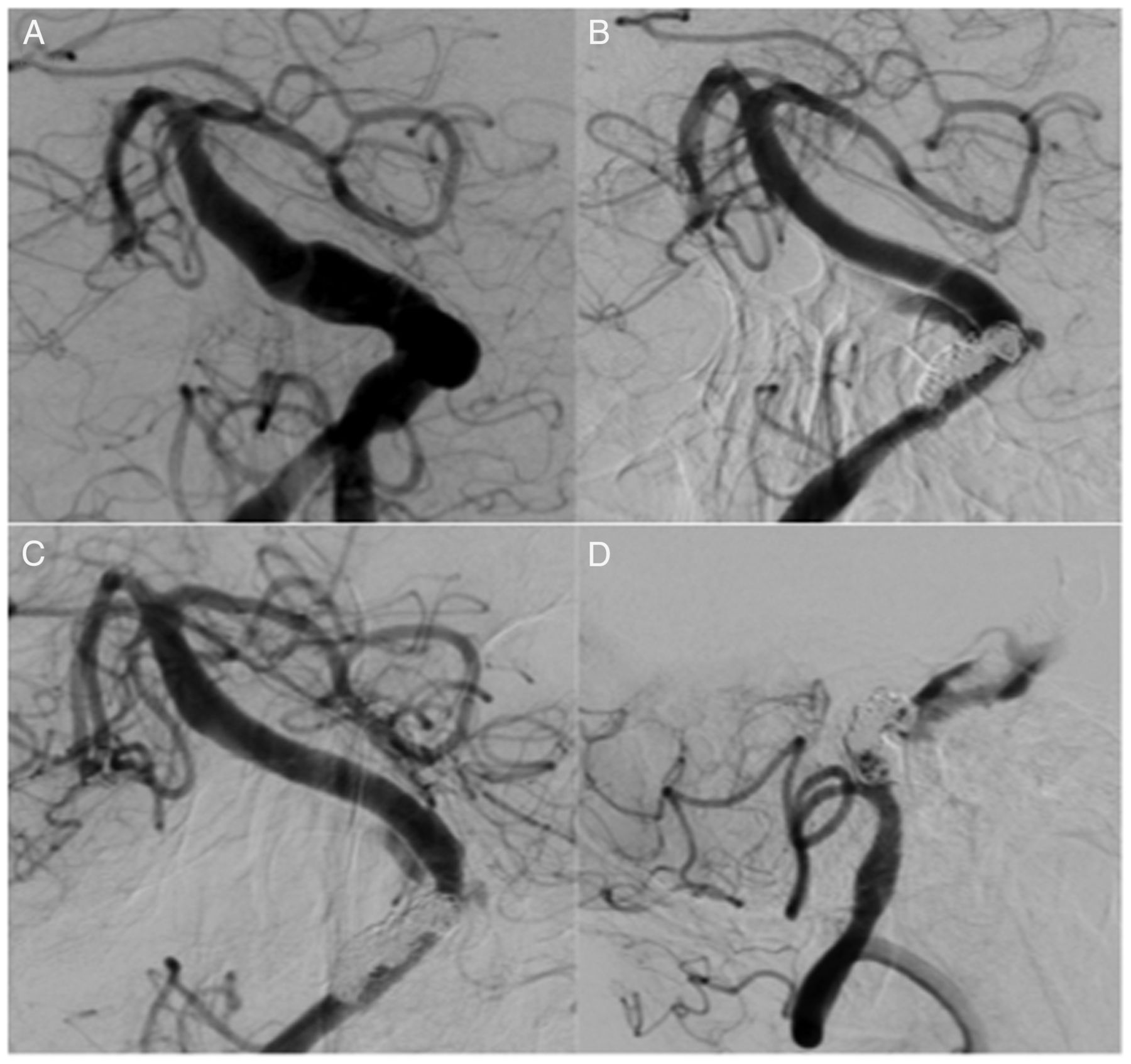
The anatomic location was determined by the extent of the lesion (where the abnormality was thought to begin and where it appeared to end) and classified into five groups: (1) vertebral only; (2) basilar only; (3) vertebrobasilar; (4) vertebrobasilar–posterior cerebral; and (5) basilar–posterior cerebral. The aneurysms were classified as either dolichoectactic, fusiform, or transitional according to the classification of Flemming et al,6 with the definition of each subtype based on the following imaging appearance (figure 1):
Fusiform: dilation >1.5 times normal involving a part of the vertebral or basilar artery, without any discernible neck and with any degree of tortuosity
Dolichoectatic: uniform dilation >1.5 times normal involving the entire basilar artery, vertebral artery, or both with any degree of tortuosity
Transitional: uniform dilation of an entire arterial segment >1.5 times normal involving the vertebral artery, basilar artery, or both with a superimposed dilation of a portion of the involved arterial segment
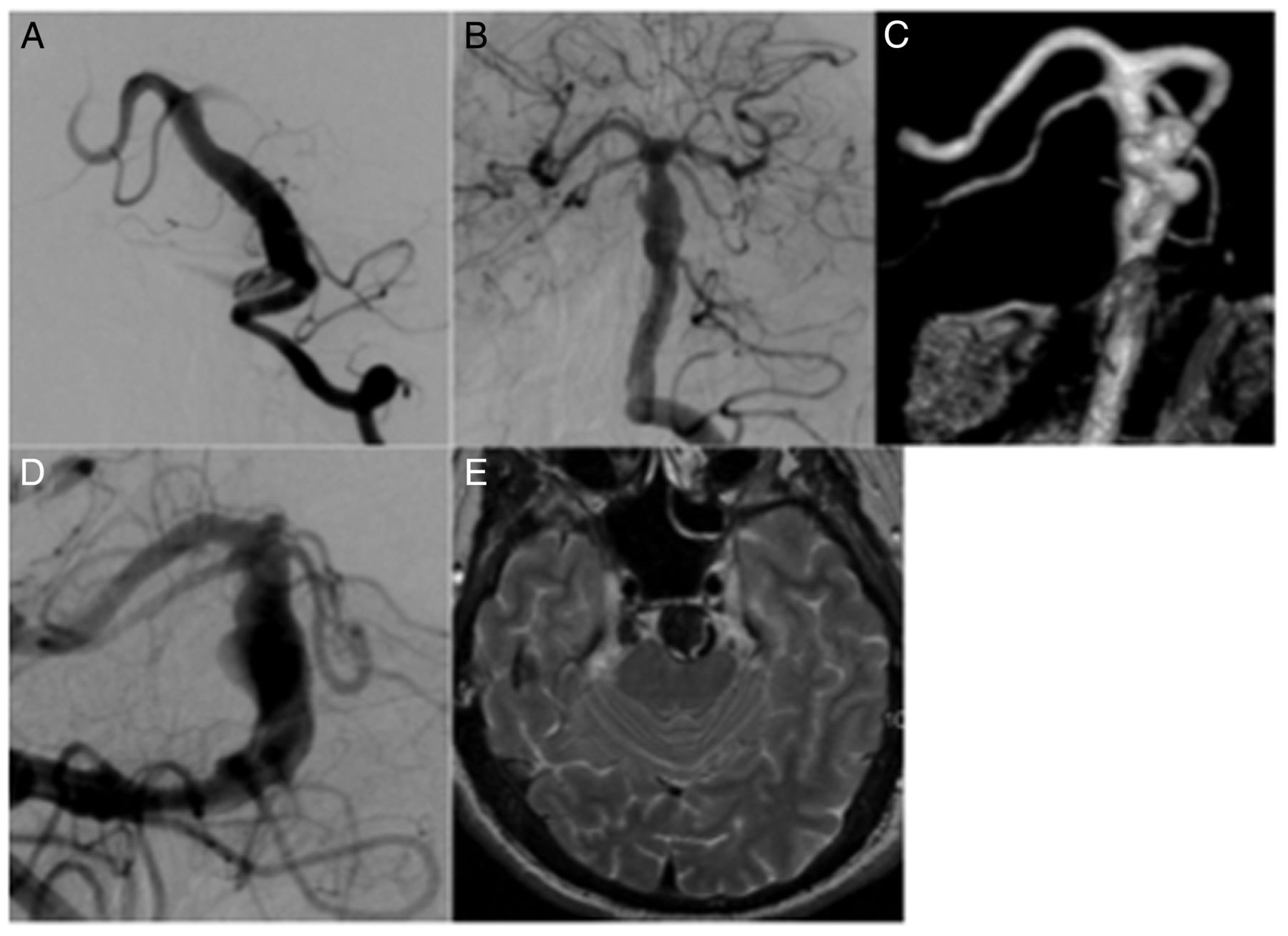
Examples of the different subtypes of aneurysm. (A) Dolichoectasia, smooth dilation of the basilar artery. (B, C) Fusiform dilation of the distal basilar artery. This aneurysm shows partial thrombosis on the MRI (not shown). (D, E) A transitional aneurysm of the basilar artery which is grossly dilated with a more focal abnormality that also shows thrombosis on MRI.
This anatomic classification was chosen since the recent work of Nasr et al27 has demonstrated a marked difference between these aneurysm subtypes with regard to their propensity to enlarge as well as the Kaplan-Meier survival curves for each of these aneurysmal subtypes. We therefore feel it is important to classify these aneurysms appropriately in order that we can determine if treatment may alter the natural history of the disease.
Imaging characteristics
The maximum diameter of the vessel was measured on axial imaging at the point of maximal dilation. For those patients with MRI prior to intervention, note was made of: (1) the presence of thrombus within the aneurysm; (2) the presence of T1 hyperintense signal within the aneurysmal wall; (3) the presence of mass effect on the nearby structures of the posterior fossa; and (4) any infarctions seen within the territory of the posterior circulation seen on either T2/FLAIR sequences or diffusion-weighted imaging sequences. These characteristics were also shown to be more common in different aneurysmal subtypes and were therefore included in our evaluation.
Endovascular treatment
All treatments were performed under general anesthesia. Two commercially available FDS were used: Pipeline embolization device (PED; Medtronic) and p64 (Phenox). Patient informed consent was obtained before the procedure in all cases. The selection of FDS was dependent upon the operators' judgement.
All patients received dual antiplatelet therapy (aspirin 75 mg daily and clopidogrel 75 mg) prior to the treatment. The effectiveness of the antiplatelet regime was tested using the Multiplate analyser (Roche). The post-procedural antiplatelet regime consisted of clopidogrel continued for 12 months or longer following treatment and aspirin continued for life. Ticagrelor was substituted for patients non-responsive to clopidogrel.
All procedures were performed via the right common femoral route using a 6 Fr access system as standard and were performed under heparin anticoagulation with a 5000 IU bolus dose at the start of the procedure and subsequent 1000 IU bolus doses every hour to maintain the activated clotting time between 2 and 2.5 times compared with the baseline value.
Procedural assessment and follow-up
Patency and flow characteristics within the parent artery and aneurysm were assessed on follow-up catheter angiography. MRI was performed in most patients.
Neurological examinations were performed to rule out potential ischemic or hemorrhagic complications in the postoperative period (<24 hours post-procedure) and at each subsequent follow-up.
IRB approval was not required for this study.
Results
Patient population
We identified 56 patients with 58 aneurysms (two patients had bilateral aneurysms of the vertebral arteries) who met our inclusion criteria (table 1). Just over 80% of patients were men and the mean±SD age at first treatment was 63.5±9.96 years (range 49–86). Patients who were symptomatic from the aneurysm (n=22) accounted for 37.9% of patients, with the rest presenting incidentally or for reasons thought not to be related directly to the aneurysm. At presentation, 50 patients had an mRS score of ≤2 with the remaining six patients presenting with an mRS score of ≤5.
Baseline characteristics of patients
Imaging characteristics and anatomic localization
The most common anatomic location of aneurysms in our cohort was vertebrobasilar (44.8%) with vertebral location the second most common location (29.3%) and basilar the third (18.9%) (tables 1 and 2). Location extending from the vertebral artery into the posterior cerebral arteries and extending from the basilar artery into the posterior cerebral arteries was relatively uncommon.
Imaging and anatomical characteristics of patients
The mean±SD maximal diameter of the aneurysms was 11±5.48 mm (range 5.5–30 mm). The maximal diameter of 25 aneurysms was ≥10 mm (43.1%).
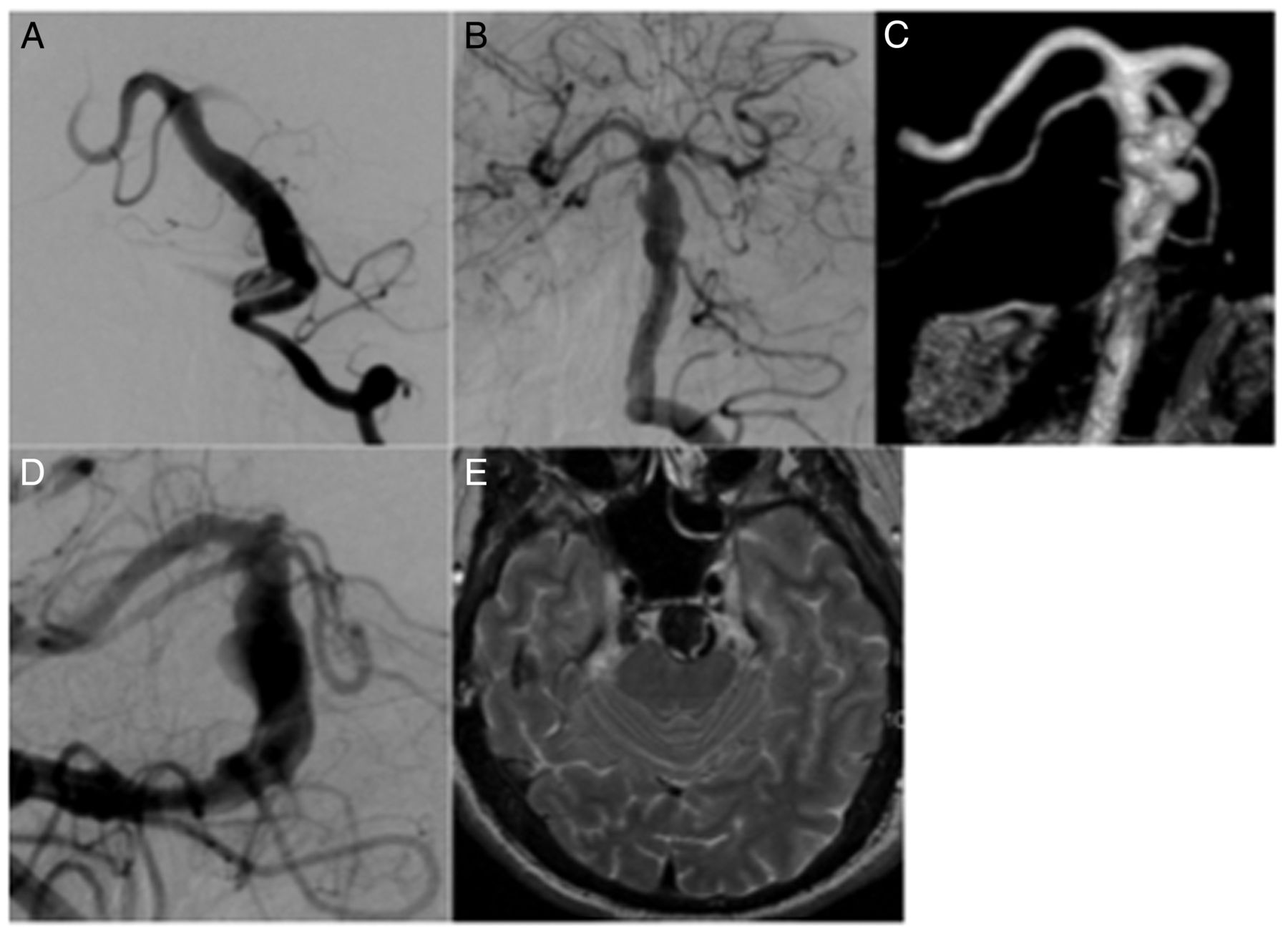
The majority of aneurysms in our cohort were transitional, with 28 aneurysms (48.2%) having this anatomic classification. There were 24 fusiform aneurysms (41.3%) and six were dolichoectactic (10.3%). Of the dolichoectactic aneurysms, four (66.6%) involved only the basilar artery, the majority of fusiform aneurysms (n=17, 70.8%) involved only the vertebral artery (figure 2) and, of the transitional aneurysms, 21 (75%) were vertebrobasilar in location.

A patient with an asymptomatic V4 fusiform aneurysm (A, white arrow). Two telescoped Pipeline embolization devices were placed in situ with stagnation of contrast medium seen in the aneurysm at the end of the procedure (B, white arrow). A follow-up angiogram performed 4 months after the procedure confirmed closure of the aneurysm and patent vertebrobasilar system (C).
Transitional aneurysms were the largest of the three subtypes with the maximum diameter seen in the basilar (13.6 mm, range 7–19 mm) and vertebrobasilar locations (13.5 mm, range 5.5–20 mm). For fusiform aneurysms the basilar location showed the largest maximal diameter (11.7 mm, range 8.5–17 mm) and, for dolichoectasia, disease affecting both the vertebral and basilar arteries showed the largest diameter (11.5 mm, range 7–16 mm).
Most patients (n=53) had MRI at initial presentation. This was performed to assess the presence of mass effect, infarction, intra-aneurysmal thrombus, and any other intracranial pathology that may preclude treatment. Patients with transitional aneurysm subtypes were seen to have mass effect on neighboring structures, T1 hyperintensity within the wall of the aneurysm, thrombus and posterior circulation territory infarcts more frequently than either the fusiform or the dolichoectactic subtypes. Conversely, these features were least common among patients with dolichoectasia.
Treatment and follow-up
All patients were treated with FDS of the aneurysmal segment (table 3). None of the patients had coils placed in the aneurysmal sac (if present). In disease that crosses the vertebrobasilar junction, after treatment with FDS, coil occlusion of the contralateral vertebral artery is required in order to stop the otherwise persistent endoleak around the new flow diverter construct. This is an essential part of the treatment plan. In total, 338 FDS were implanted in the 56 patients (163 p64 stents, 175 PEDs).
Treatment and imaging outcome of patients
Fusiform aneurysms of the basilar artery and transitional aneurysms of the vertebrobasilar arteries required the most FDS in order to reconstruct the vessels (average 8.3 and 8.2, respectively; figure 3). In circumstances that required multiple telescoped FDS, up to 19 were used to treat a basilar fusiform aneurysm in a single patient whereas significantly fewer were used for disease that was confined to the vertebral artery (mean 2.8, range 1–3). Treatment was carried out in a multistage process with up to five treatment sessions required in some patients. The more complicated aneurysms required more procedures (mean 3.66 for basilar fusiform aneurysms, 1.86 for vertebrobasilar transitional aneurysms).

A patient with symptoms of mass effect from a vertebrobasilar transitional aneurysm (A) underwent treatment with 16 telescoped Pipeline embolization devices (B). The procedure was noted to be technically difficult but there were no procedural complications. Follow-up angiography performed 16 months after the procedure showed good reconstruction of the vessel with only a small remnant aneurysm (C). There was no evidence of pontine infarction on MRI.
The last angiographic follow-up was performed at a mean of 25.2 months (range 1–72 months). In our cohort nine patients died and three had no angiographic follow-up. Of the remaining patients, complete restoration of normal angiographic appearance was obtained in 66.6% of those with dolichoectasia (figure 4) with only minor flow in the remaining patient with angiographic follow-up. In patients with fusiform aneurysms there was complete aneurysm occlusion in 18 patients (75%) with a minor remnant seen in three patients (12.5%) and an unchanged appearance in one patient (4%). There was one death and one patient without angiographic follow-up in this group. In the patients with transitional aneurysms, five were completely occluded (17.8%) (figure 5), with seven showing only minor remnants (25%). In five patients there was still a major remnant although in all of these aneurysms flow reduction could be seen on angiography. In two aneurysms there was no change in the appearance of the aneurysms although flow into the aneurysmal sac had been reduced.

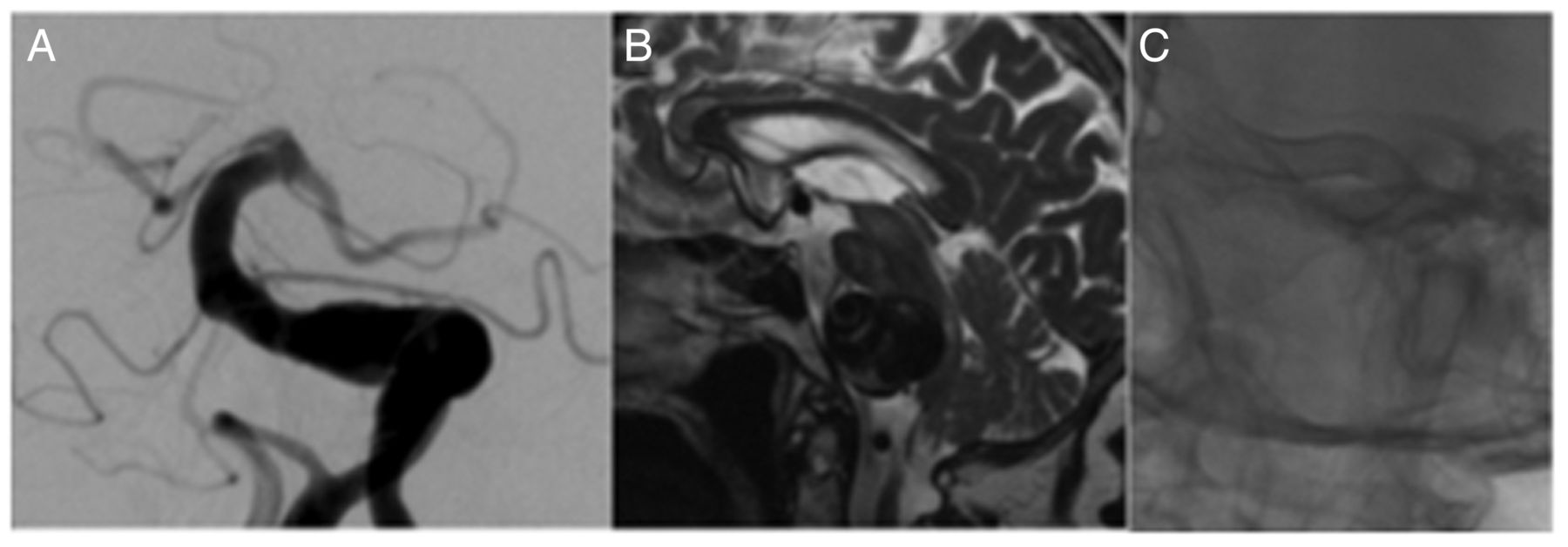
(A, B) A patient with dolichoectasia of the basilar artery (7 mm) treated with telescoped Pipeline embolization devices showed no progression of the disease on the follow-up angiogram performed at 14 months.

(A, B) A patient with a transitional basilar artery aneurysm 4 months after treatment with three telescoped Pipeline embolization devices showing complete reconstruction of the vessel with no further filling of the aneurysm.
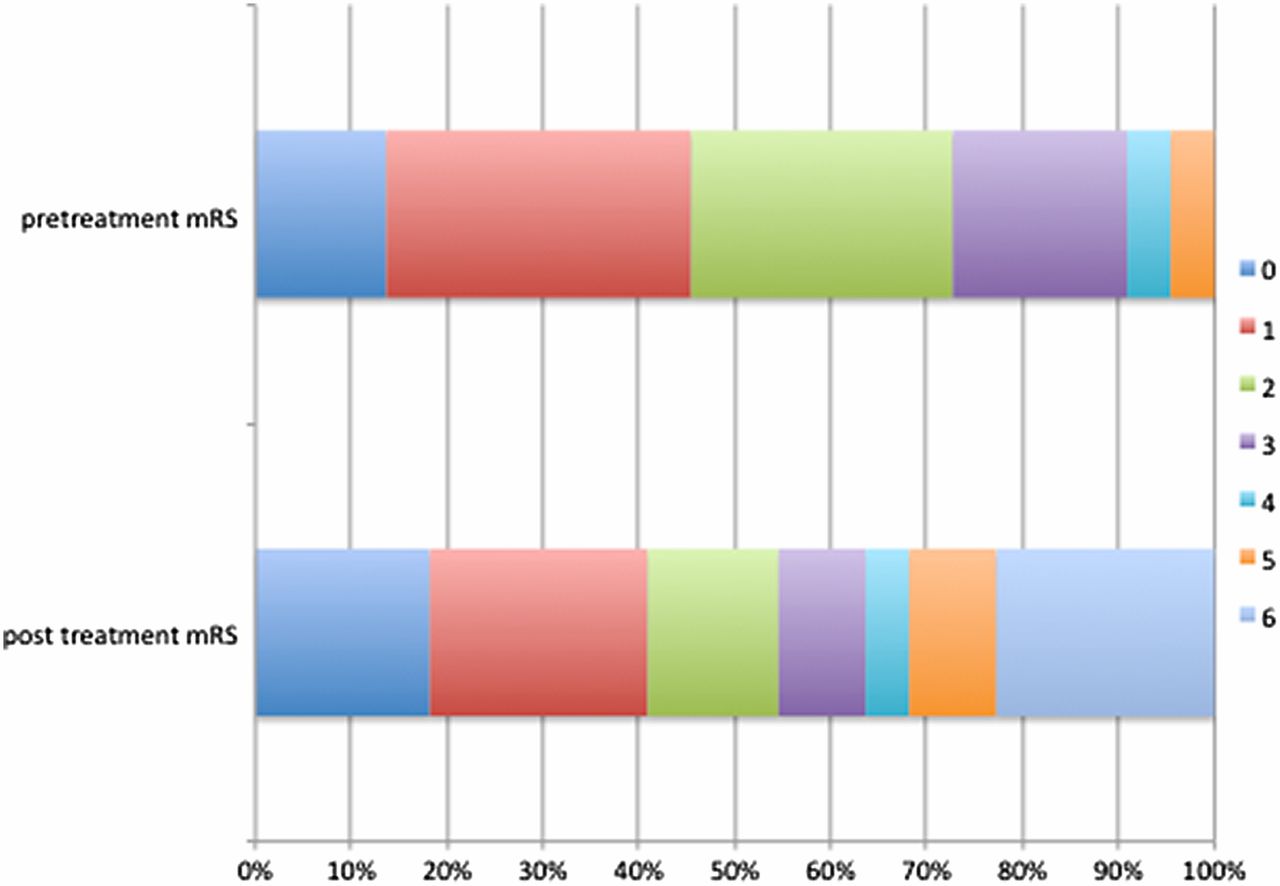
The initial and final mRS score of patients was recorded and analysed according to the initial presentation of patients (eg, whether or not the aneurysm was symptomatic at presentation). All patients who were initially asymptomatic presented with a mRS score of ≤2 and 82.8% of patients had a final mRS score of ≤2 (figure 6). However, in the symptomatic group, 72.7% of patients presented with a mRS score of ≤2 and only 54.5% had a mRS score of ≤2 at last follow-up (figure 7). Similarly, the incidence of a mRS score of 6 was just over twice as high in the symptomatic group compared with the asymptomatic group (22.7% vs 11.1%).
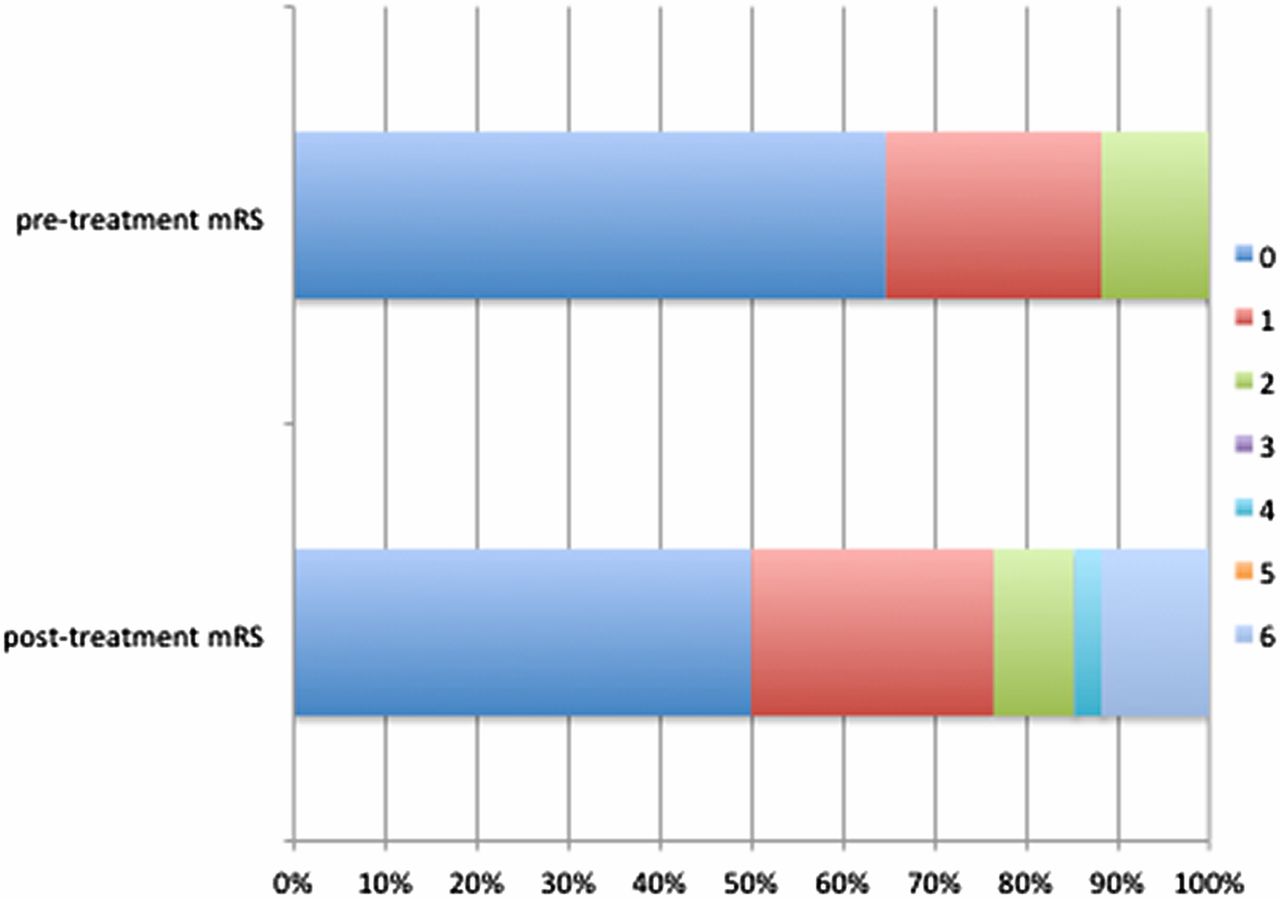
Breakdown of the modified Rankin Scale (mRS) score pre- and post-intervention for patients who did not present with symptoms related to the aneurysm.
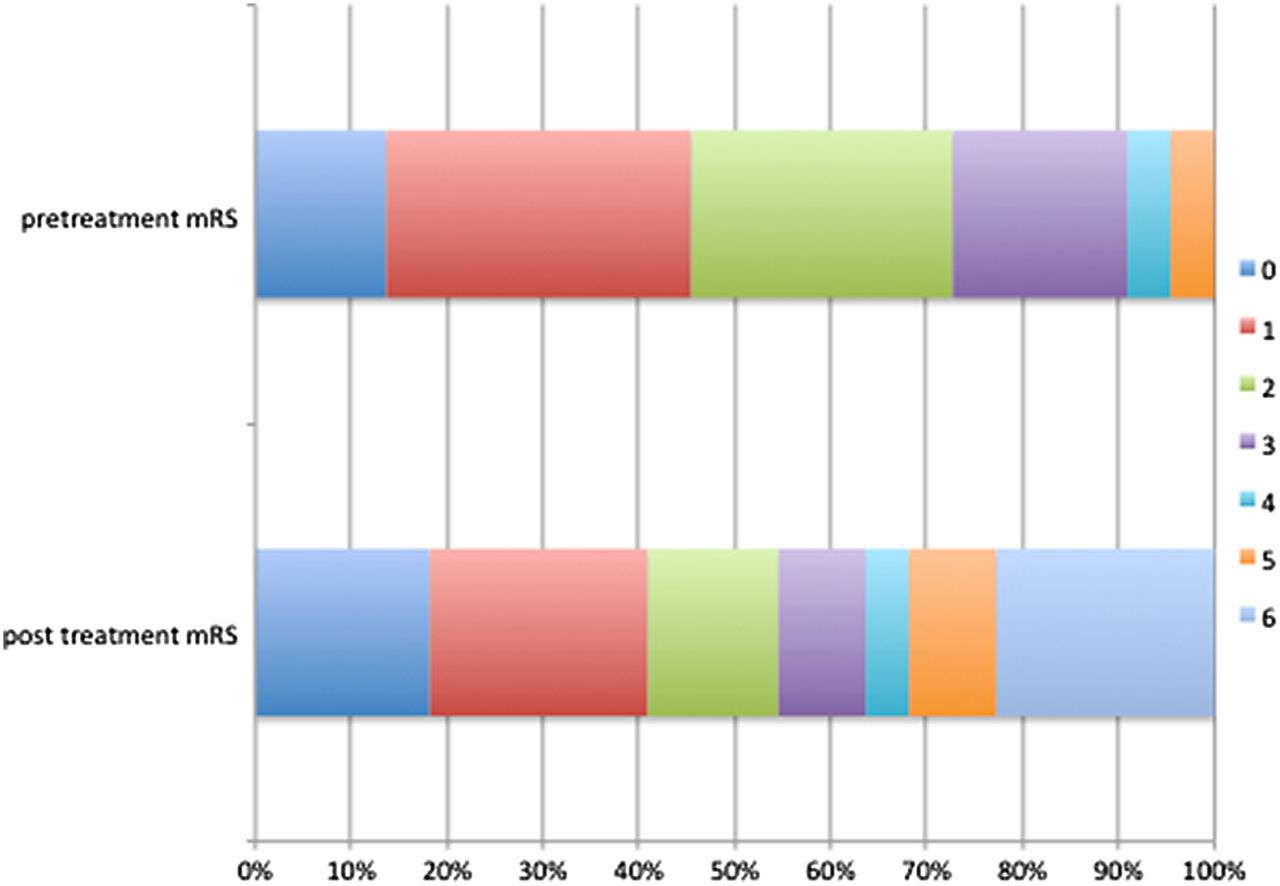
Breakdown of the modified Rankin Scale (mRS) score pre- and post-intervention for patients who presented with symptoms related to the aneurysm.
Complications and deaths
Seven patients had ischemic symptoms, one of whom inappropriately stopped taking clopidogrel which resulted in thrombosis of the superior cerebellar arteries bilaterally and the left posterior cerebral artery and a final mRS score of 5. Four of these patients had a final mRS score of ≤2 with the remaining two patients having a mRS score of 4. One patient had a traumatic intraventricular hemorrhage and one other patient had a cerebellar hemorrhage. The overall complication rate was 15.5%.
Nine patients in our cohort (15.5%) died, five of whom were symptomatic at presentation (figures 8 and 9), which represents death in 22.7% of patients who were symptomatic at presentation. In-stent thrombosis occurred in three patients, secondary to stopped medication in one patient, inappropriate use of ibuprofen which antagonized aspirin in another, and loss of platelet inhibition secondary to a platelet transfusion required for uncontrollable inguinal hemorrhage in another. In the remaining patients there was one fatal subarachnoid hemorrhage, two cases of progressive mass effect (one in which the patient refused to have the contralateral vertebral artery coil occluded following FDS treatment resulting in persistent endoleak and aneurysm enlargement; figure 10), two ischemic events, and one patient died of unrelated causes.

A patient who presented with recurrent posterior fossa strokes was found to have a transitional vertebrobasilar aneurysm (A). He underwent treatment with 18 telescoped Pipeline embolization devices that extended from the P1 segment to the vertebral artery (B). Flow through the Pipeline devices into the aneurysm and distally into the posterior cerebral arteries could be demonstrated at the end of the procedure (C).

The same patient as in figure 8 acutely deteriorated 24 hours after the procedure. An angiogram confirmed patent basilar artery and good flow distally (A). MRI digital-weighted imaging and ADC showed restricted diffusion in the pons (B, C). A T2-weighted MRI scan performed 5 days later showed a pontine infarction (D) and the patient died shortly thereafter. ADC, apparent diffusion coefficient.
A patient who presented with symptoms of mass effect from a partially thrombosed vertebrobasilar transitional aneurysm was initially treated with five telescoped Pipeline embolization devices placed in the left vertebral artery. The patient was due to have coil occlusion of the contralateral vertebral artery but refused further treatment and later died from progressive mass effect.
Discussion
Non-saccular aneurysms of the vertebrobasilar tree are characterized by elongation, dilation and/or tortuosity of the vessel. The end appearance, which can be striking, is likely due to a variety of different processes and this may account for the difference seen in the natural history and prognosis. Flemming et al6 reported the most thorough longtidunal evaluation with 159 patients and 719 patient years. In this study, which excluded dissecting aneurysms, the lesions were defined radiologically as fusiform, dolichoectactic, or transitional (see earlier for definition). Using this classification, 57% of patients in the Flemming cohort had dolichoectasia, 25% had a transitional aneurysm, and 18% had a fusiform aneurysm with 20.8% having an indeterminate type. In this cohort the transitional and fusiform types were more likely to be symptomatic with dolichoectatic aneurysms appearing more benign in clinical course. After age adjustment, fusiform type, transitional type and basilar involvement all had increased HRs for mortality (HR 7.7, 3.56, and 8.77, respectively). Furthermore, asymptomatic patients did not often become symptomatic, with stroke seen in 7.8%, mass effect symptoms in 3.1%, and hemorrhage in 1.6%. Mizutani et al28 proposed a different classification in 1999; however, they also showed that dolichoectactic aneurysms found incidentally had no significant neurological sequelae in follow-up and neither group reported a transformation from dolichoectasia to fusiform type. Recently Nasr et al27 published their analysis of the imaging characteristics associated with growing and ruptured non-saccular and dolichoectatic aneurysms of the vertebrobasilar tree. They showed that, while transitional aneurysms (56.3%) and fusiform aneurysms (24.4%) were the most likely to grow, dolichoectactic aneurysms also grew (8%) during the follow-up period (mean 40 months for dolichoectactic aneurysms). These results are similar to those of Passero and Rossi10 who found that approximately 5% of dolichoectactic aneurysms progressed (defined as either increasing tortuosity and/or enlargement) over a 5 year follow-up period. The study by Nasr et al27 also showed a significant difference in the Kaplan-Meier survival curves for the various subtypes, with approximately 90% survival at 100 months for patients with dolichoectasia and less than 30% for those with transitional morphology.
The natural history of these lesions is extremely variable and is dependent upon their initial presentation, which in all likelihood is also related to their morphological appearances. Flemming et al6 found that the ischemic stroke risk was higher than the risk of hemorrhage and the rate of infarction related to the aneurysms rose from 2.7% at 1 year to 15.9% at 10 years. The risk of a recurrent stroke, for patients initially presenting with stroke, was calculated as 6.7% per year (median time 1.73 years). Symptomatic lesions, previous ischemia secondary to the aneurysm, and transitional aneurysmal type were all seen to increase the factors for stroke (HR 16.2, 3.88, 3.2, respectively). Similarly, 18.8% of patients with transitional aneurysms in the cohort of Nasr et al27 developed new infarcts. For dolichoectactic aneurysms the risk of infarction is not negligible with 14.7% in the Nasr et al cohort having new infarctions. The exact cause of the ischemia is not fully elucidated; however, several mechanisms have been put forward. These include occlusion of the small perforating vessels caused by the significant distortion of the parent basilar artery, embolization of thrombus within the parent artery, and/or in situ thrombus formation within the small perforating vessels as well as the parent artery.
Compressive symptoms were seen in 22% of patients in the cohort of Fleming et al6 and approximately three-quarters of these patients had only mild or no disability. At 1 year only 46% of patients had mild or no symptoms and, importantly, 7.5% who did not initially have compressive symptoms developed them. The growth of aneurysms is associated with development of compressive type symptoms and, in the Mayo Clinic cohort, approximately half of all patients demonstrated enlargement, which was statistically associated with the transitional and fusiform subtypes, larger size (15 mm vs 8 mm), and symptomatic presentation. Furthermore, T1-weighted high signal within the vessel wall was more common in enlarging aneurysms and, in the Nasr et al cohort, 54% of aneurysms that enlarged showed T1 hyperintensity compared with only 20% of those without enlargement. Aneurysm growth also affects mortality, with a 5 year mortality of enlarging aneurysms of 56.5% compared with 3.7% for stable aneurysms.18
As with other aneurysmal pathologies, rupture is also a risk although it appears that the risk of rupture is less than that of ischemia/compression. In the cohort of Nasr et al27 rupture was seen in 12.5% of patients with a transitional aneurysm, 6.7% of those with fusiform aneurysm, and 1.3% of those with dolichoectasia. They also showed that, for those aneurysms that were ≥10 mm, the annual rupture rate was 6.8% compared with 2.5% for those <10 mm. Similarly, in the cohort of Flemming et al6 the annual risk of rupture for fusiform and transitional aneurysms was 2.3% while that of dolichoectatic aneurysms was 0.4%. As with compressive symptoms larger size was also associated with rupture and, in the multivariate analysis of Passero et al,11 a median basilar artery diameter of 6.8 mm was associated with intracranial hemorrhage.
Given the prognosis, it is no wonder then that management options have been aggressively sought. Surgical treatment of these lesions often involved either flow reduction if inadequate collateral supply was available, flow reversal if adequate collateral supply was available, or trapping with hematoma decompression for lesions that presented with acute mass effect. In the series published by Drake and coworkers,29 ,30 63% of patients who had flow reduction had an excellent/good outcome with 74% of those undergoing flow reversal having an excellent/good outcome. Similarly, 71% of patients who had trapping and thrombectomy achieved good outcomes.30 As might be suspected, the likelihood of success following ligation is related principally to the supply from the posterior communicating arteries (PCom), with a 6.7% chance of ischemia in patients with at least one large PCom (>1 mm) compared with 43% in patients with two small PComs (<1 mm). In the case of poor collaterals, bypass surgery can be performed prior to flow reversal/reduction and this is often achieved via a superficial temporal artery to superior cerebellar/posterior cerebral artery bypass. Kalani et al31 reported their series of 11 patients using these bypass techniques and, despite the fact that the mortality at 1 month was 45%, the remaining patients achieved an average mRS of 2.5 (mean follow-up 71.6%). Vessel sacrifice can also be achieved endovascularly. For example, Leibowitz et al32 reported their results of 13 cases, 10 of whom represented fusiform aneurysms of the vertebrobasilar system. In six patients flow reduction was attempted via dominant vertebral artery occlusion for patients with either vertebrobasilar junction or basilar aneurysms. Four of the patients died, one patient deteriorated clinically, and the other remained stable. The remaining four patients had disease confined to the vertebral artery and these patients all improved clinically. Similarly, Sluzewski et al33 reported six cases of basilar fusiform aneurysms treated with bilateral vertebral occlusion. Of these cases, the three patients that presented in good condition did well postoperatively and the three patients that presented in poor condition had a poor postoperative outcome. Again, these authors noted that the presence of large PComs was predictive of a good functional outcome.
The advent of FDS heralded a significant advancement in the management of intracranial aneurysmal disease. This was initially met with great enthusiasm in the neurointerventional community and it was believed that the ability to reconstruct diseased vessels would offer a particular advantage for the treatment of fusiform aneurysms of the posterior circulation.
In 2012 Siddiqui et al25 reported their experience of treating fusiform vertebrobasilar aneurysms. In their case series FDS were used to treat seven patients, all of whom also received dual antiplatelet therapy. Similar to many of our cases, several telescoped stents were used (3–9 stents). In this relatively small series, four of the seven patients died and a further patient had severe neurological disability. The remaining two patients had a good outcome and the authors concluded that the treatment of vertebrobasilar aneurysms with FDS carries a significant morbidity and mortality. Similar poor results were also reported by Raphaeli et al16 who reported 25% mortality. Better results were reported by Chalouhi et al34 who used the PED to treat three aneurysms with no reported complications or mortality at follow-up of 5.5 months. More recently, Munich et al35 published their series of 12 patients who were treated with FDS. Excluding the two patients that presented with SAH, seven patients showed complete occlusion with one case showing persistent filling and an endoleak. One patient in this series died, although this was secondary to acute respiratory distress and pneumonia. There were no cases of acute in-stent thrombosis in this series. Phillips et al26 published their series of 32 patients with an overall rate of permanent neurological complications of 9.4% (3/32). However, they reported that all three patients had only mild residual symptoms and good a clinical outcome with a mRS score of 1 and a return to independent living and work. The aneurysm occlusion rate in this series was 96% at >1 year follow-up, but it is important to note that this study did not deal exclusively with non-saccular aneurysms, with 12 of 32 aneurysms classified as berry aneurysms. Natarajan et al36 also recently published their series of 12 patients, only one of whom suffered a perforator territory infarction with poor clinical outcome (mRS 4). There were no deaths in this cohort and the results of this study are considerably better than previously reported by the same group in 2012.25 The improvement in the results is attributed to several factors:
A strict antiplatelet regimen with confirmation of the therapeutic effect of the antiplatelet therapy prior to the intervention.
Patient selection: the authors note that patients in this latter cohort presented earlier than those in the series of 2012, with only 25% of the patients in the most recent series presenting with ischemic symptoms but none had evidence of ischemia on MRI, therefore in this series the patients presented earlier than in the original series. The authors also state that patients presenting with acute ischemic symptoms from brainstem infarction or compression carry a bad prognosis. This may be due to already compromised perforator ostia as well as a larger number of devices required to treat these vessels.
A decreased number of flow diverters was used in the latter series and this is at least in part because longer PEDs have become available that allow easier reconstruction of the diseased vessel.
Adjunctive coiling was used in 50% of the cases and the authors now place coils in all the aneurysmal sacs if possible. They believe that the addition of coils in the aneurysmal sac helps to act as a scaffold for the PED and prevents foreshortening of the PED construct. Furthermore, they believe that the addition of coils will help protect against hemorrhagic complications and promote thrombus formation within any saccular components of the aneurysm.
We concur with some of these findings and believe that early management prior to infarction or compressive symptoms is extremely important to achieve a good clinical outcome. In our data the mortality was double that in patients who were symptomatic at presentation (22.7% vs 11.1%). We also agree with these authors with regard to a strict antiplatelet regimen because in-stent thrombosis or thromboemboli are a significant risk, as highlighted by several of our cases. Platelet function is tested routinely in our clinical practice. Additionally, since 2016 we have added direct oral anticoagulants (eg, 2×100 mg dabigatran daily) for patients with large fusiform or transitional type aneurysms involving the basilar trunk. We believe that coils within an aneurysmal sac may be useful but, in our experience, do not appear to be necessary and this needs to be based on individual anatomy. The number of FDS required to obtain a good result is difficult to determine. This will be, at least in part, based on the longitudinal extent of the disease. The target of the treatment should be to redirect flow away from the diseased vessel wall and this, in our opinion, is most important at the level of a saccular aneurysm. Furthermore, as is discussed later, neoendothelialization commences from the site of contact with the parent artery. We therefore believe that it is important to land the FDS in a portion of the vessel that demonstrates a normal appearance, both at the proximal and distal end. We believe this will assist neoendothelialization. A summary of the published literature is provided in table 4.
Summary of the published literature on the use of flow-diverting stents in posterior circulation fusiform aneurysms
The recent work of Kadirvel et al47 is important to acknowledge when considering fusiform aneurysms. In this elegant animal study it was shown that the formation of neointima is required to cause complete exclusion of aneurysms from the circulation, and this process of neointimal formation begins at the site of contact between the FDS and the parent artery. The process then proceeds from the site until it covers the aneurysmal neck. During this process only scattered inflammatory cells were seen on the FDS struts that cover the aneurysmal neck. If this process is similar in fusiform aneurysms, and there is no reason to our knowledge to suspect that it is not, then it stands to reason that longer diseased segments will require a much longer time to neoendothelialize. With regard to antiplatelet medication, this means that a tailored approach is required with some patients likely to require lifelong double antiplatelet medication. This is likely to be true for those with non-saccular aneurysms, which may endothelialize very slowly. Some evidence to support this view recently came from Szikora et al48 who performed a histopathological analysis of five deceased patients treated with FDS in both the anterior and posterior circulation for fusiform aneurysms. In three patients the flow diverter had been present for over 6 months yet in only one patient was neoendothelialization and intimal hyperplasia identified, and this was only seen on the section of flow diverter that was in the normal artery proximal to the aneurysm. In the remaining patients a thin layer of fibrin without smooth muscle cells was seen covering the inner layer of the flow diverter. This small but important study appears to support the work of Kadirvel et al, although further evidence is required. Neoendothelialization may not occur even after 12 months, however the angiogram can demonstrate lack of contrast entering the aneurysm.48 It is important to realize that lack of contrast entering the aneurysm does not mean endothelialization of the flow diverter has occurred. Under these circumstances, a lack of platelet inhibition could result in either thrombosis of the flow diverter or distal embolism. Therefore, it is important to tailor the antiplatelet regime to the patient and the disease process. Long segments of disease may require lifelong dual antiplatelet medication.
The telescoping method used in our patients was similar to that described previously by Siddiqui et al,25 and gas been modified during the last 7 years. In general, we aimed to obtain maximal coverage at the site of maximal diameter and looked for flow redirection into the FDS construct and away from the vessel wall. We prefer telescoping from proximal to distal with about 30% overlap of the implanted FDS. The diameter of the most proximal stent should be slightly larger than the diameter of the landing zone (eg, 4 mm). Subsequent FDS should have the same or larger but never smaller diameters, since smaller diameters will result in FDS displacement. Since the PED comes with a heat pretreatment while p64 does not, the coverage of the unrestrained PED is less than with p64. This aspect influences which implant will be used: PED for less and p64 for more coverage. A combination of PED and p64, devices with non-matching braiding patterns, will result in more coverage than telescoping of devices of the same kind. These technical aspects leave plenty of space for the intuition of the operator. The procedure is usually stopped as soon as a hemodynamic effect becomes visible through repeated catheter angiography. The patient returns for repeat angiography and MRI after approximately 6–12 weeks to observe for flow changes and changes in size of the aneurysm. If no significant flow redirection has occurred compared with the pretreatment angiography, then more FDS are placed inside the construct. Similarly, if an adequate amount of flow redirection into the FDS has occurred, then coil occlusion of the contralateral vertebral is performed (if required). This procedure is repeated until a satisfactory degree of flow redirection into the FDS construct has occurred. In some cases stagnation of flow between the FDS and the aneurysmal wall could be seen almost immediately and, in these cases, the procedure was stopped at this point with repeat MRI and angiography performed after 3 months. If the follow-up digital subtraction angiogram revealed continued flow through the FDS into the aneurysm, which is mostly confined to certain focal points rather than affecting the entire length of the implants, additional FDS were deployed. The aim remains the gradual reconstruction of a smooth vessel lumen with a maximum diameter of 4.5–5 mm, avoiding both proximal and distal endoleaks as well as contrast exit at any point of the FDS construct.
Gradual vessel reconstruction obviously allows for the development of collateral brainstem circulation, eventually with no opacification of pontine basilar artery branches but without signs of brainstem ischemia, neither clinically nor on MRI. In our experience, gradual adaption of the local circulation through staged FDS implantation, confirmed dual anti-aggregation, and mild oral anticoagulation are key.
In our experience, disease of the basilar trunk and disease that crosses the vertebrobasilar junction can be the most difficult to treat. In addition to the flow diverters, coil occlusion of the contralateral vertebral artery is required to prevent a persistent endoleak around the flow diverter.49 This is important since continued flow from the contralateral vertebral artery between the FDS construct and diseased wall may result in disease progression, as was seen in one of our patients who refused occlusion of the contralateral vertebral artery. Furthermore, we are unsure of the changes in hemodynamic stress that will be exerted on the diseased wall by flow between the FDS construct and diseased segment, although we do not believe this would be conducive to healing. Whether the coil occlusion should be performed before the flow diverter is implanted, simultaneously, or afterwards is open to conjecture and we have no experience to promote a particular chronological order. We favor implanting the flow diverters initially and then, at a later date, coil occluding the contralateral vertebral artery as the flow diverters will prevent distal migration of the coils. We have also seen that, despite dense coil packing, flow through the contralateral vertebral artery may continue and therefore newer endovascular closure devices such as the UNO (Covidien)50 should be considered as alternatives for vessel occlusion, although our experience with these devices is limited (figure 11). Furthermore, in some cases where the aneurysm sac is positioned at or very close to the anterior inferior cerebellar artery (AICA) or ACIA/posterior inferior cerebellar artery (PICA), there is persistent filling of the aneurysm via the flow into these arteries (figure 12). Therefore, in this anatomic disposition, a combined surgical and endovascular procedure with surgical bypass of these arteries followed by flow diversion may be an alternative strategy, although we have no experience of this.
A patient with a vertebrobasilar transitional aneurysm (A) treated with 14 flow diverting stents (5 Pipeline embolization devices, 9 p64 devices) and coiling of the contralateral vertebral artery. There has been good reconstruction of the vertebral and basilar artery with a decrease in the aneurysmal filling seen on follow-up angiography (B, 22-month angiogram following initial treatment; C, 28-month angiogram). However, despite dense coil packing in the contralateral vertebral artery, a persistent leak into the aneurysm can be seen through the coil ball mass (D) warranting repeat occlusion of the vertebral artery.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
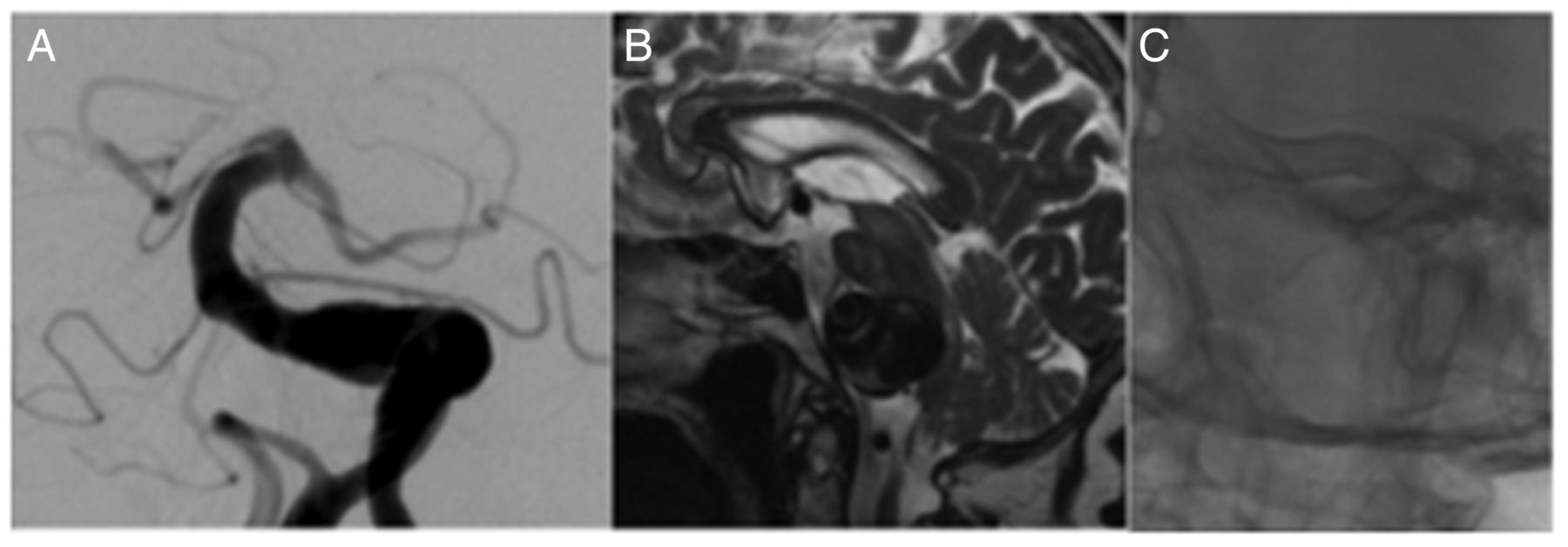
A patient was incidentally found to have dilation of the basilar artery on routine MRI (A). At this point the patient refused further investigation. The patient had repeat MRI 26 months later (B) and the aneurysm had significantly increased in size with mass effect and small pontine infarction. Angiography performed at this time revealed a transitional vertebrobasilar aneurysm (C). The patient was treated with a flow-diverting stent and coil occlusion of the contralateral vertebral artery. A follow-up angiogram performed 24 months later shows good reconstruction of the basilar artery but persistent filling in the region of a large anterior inferior cerebellar artery/posterior inferior cerebellar artery (D, white arrow). A repeat angiogram after a further 6 months shows slightly slower but persistent filling (E). An MRI performed at the same time showed no significant increase in the aneurysm size or mass effect but increasing thrombus within the aneurysm (F).
A major difficulty in these cases comes from the timing of the treatment. In asymptomatic patients one cannot be reliably sure that the aneurysm is stable unless serial imaging is performed. This inherently carries a risk that the patient will become symptomatic either with new infarctions or progressive mass effect and the consequent deterioration in operative outcome. If one opts for an aggressive treatment strategy, then one may treat patients with otherwise stable aneurysms. This is not in itself a problem, especially for patients with fusiform or transitional subtypes as well as those with basilar involvement, since we know these carry a poor prognosis overall. For dolichoectasia, where the risk of growth is relatively low, regular serial imaging could be considered in the first instance and, as soon as growth is seen, treatment could be considered. Additionally, if the results of Kadirvel et al47 and Szikora et al48 are accurate, then it stands to reason that treating shorter diseased segments will likely result in a more rapid exclusion of the aneurysm from the circulation as bridging of the aneurysm neck with neointima will occur more rapidly.
Overall, a criticism of the previously reported studies is that they have not clearly defined the aneurysms, and yet it is now clear that location, aneurysmal subtypes, MRI characteristics, and clinical presentation all have a major impact on the prognosis of the disease. Our study is the first to analyse non-saccular aneurysms treated with FDS in this manner in order to gain a greater understanding of which aneurysms should and should not be treated. A detailed analysis of the morphology of the aneurysm (subtype, size, side branches, etc) as well as assessing for both clinical and radiological signs of, for example, ischemia or mass effect will help guide treatment plans and hopefully improve patient outcomes in this often aggressive disease.
Limitations
Our study has several limitations. It is retrospective in nature and has a relatively small number of patients with varying aneurysms in different locations. Similarly, the staging of treatments was based on individual parameters and not on a predetermined timescale. MRI is not complete and, in order to determine if treatment of these pathologies is of benefit, longer-term follow-up is required.
Conclusion
Flow diversion represents a promising treatment option for non-saccular aneurysms of the posterior circulation, but longer-term studies are required. We propose early treatment prior to the development of symptoms and when the maximum diameter and length of the diseased segment is minimized. Both transitional and fusiform aneurysmal subtypes should be managed aggressively given their poor prognosis; however, a ‘watch and wait’ strategy could be used for dolichoectactic disease with treatment commenced as soon as enlargement is seen.
References
Footnotes
Twitter Follow Marta Perez at @MartaAguilarPe2
Contributors PB and MAP: data gathering, manuscript preparation. OG and HB: review, editing. HH: overall review, study design. SF: guarantor.
Competing interests MAP and PB serve as proctors and consultants for phenox GmbH, with moderate financial compensation. HH is a co-founder and shareholder of phenox GmbH. The other authors have no potential conflict of interest.
Provenance and peer review Not commissioned; externally peer reviewed.