Article Text

Abstract
Background Venous sinus stenting is an emerging treatment for patients with idiopathic intracranial hypertension and evidence of venous stenosis. Stents placed across the transverse and sigmoid sinuses often cover the vein of Labbé (VOL), a major anastomotic vein draining the cerebral hemisphere. The patency of the VOL after stenting and its clinical implications are poorly understood.
Methods A retrospective analysis was performed of a prospectively collected database of patients undergoing venous sinus stenting. Pre- and post-stent angiography were compared to assess changes in VOL patency, clinical and radiographic outcomes.
Results The study cohort comprised 56 patients. The stent covered the VOL in 92.9% of cases. Thirty-two cases with VOL coverage had evaluable angiograms immediately after stent placement. Among these, VOL filled normally in 75.0%, exhibited diminished caliber with normal transit time in 3.1%, filled sluggishly in 18.8%, and was occluded in 3.1%. Follow-up was assessed in patients with at least 3 months' angiographic follow-up (46 patients, mean 7.2 months). Of these, normal filling was seen in 71.7%, diminished caliber in 26.1%, and sluggish filling in 2.2% of cases. Neither stent coverage of the VOL nor its patency immediately after stenting or at follow-up correlated with stent-adjacent stenosis. There were no neurological sequelae from coverage of the VOL or alteration of its drainage pattern.
Conclusions In the majority of venous stenting cases involving the transverse and sigmoid sinuses, the VOL remains widely patent. Complete VOL occlusion rarely occurs after stenting and may not result in clinical sequelae. Stent coverage of the VOL should not deter the therapeutic use of venous sinus stenting.
- Angiography
- Hydrocephalus
- Intracranial Pressure
- Stenosis
- Stent
Statistics from Altmetric.com
Introduction
Venous sinus stenting (VSS) has become increasingly used for the treatment of patients with idiopathic intracranial hypertension (IIH) who have stenosis of a dural venous sinus with a trans-stenosis pressure gradient.1–5 Most commonly, intracranial venous stenosis occurs at the transverse–sigmoid sinus junction (TSJ) or at the distal transverse sinus (TS).6 The vein of Labbé (VOL) is the largest and most important anastomotic vein of the temporal cortical venous system and typically drains into the distal TS or TSJ.7 ,8 Venous stents spanning the proximity of the TSJ often cover the ostium of VOL and any other large cortical draining veins as they enter the dural venous sinus. Intracranial venous stents have been reported to have high long-term patency rates, with low incidences of in-stent stenosis and thrombosis.7 ,9–11 Instead, stenosis after VSS occasionally occurs in the segment of the venous sinus adjacent to the stent (stent-adjacent stenosis, SAS). VOL coverage may contribute to residual elevated venous pressure, which may in turn lead to a higher rate of VSS failure and SAS.
Coverage of the VOL during VSS and its consequences have not been widely investigated.7 Therefore, the aims of our study are: (1) to assess the patency of the VOL immediately after stenting of the transverse and sigmoid sinuses and at angiographic follow-up; (2) to determine the effects of VOL coverage and patency on the rate of SAS after VSS; and (3) to assess the clinical significance of VOL coverage during VSS.
Methods
Patient selection, diagnostic and procedural details
We performed an institutional review board approved retrospective review of a prospectively maintained database of all patients who underwent diagnostic cerebral angiography and venography for possible venous sinus stenosis at the University of Virginia from February 2014 to July 2016. All patients who underwent placement of intracranial venous stents were reviewed for eligibility. Patients who underwent stent placement in the transverse and/or sigmoid sinuses were included in the study cohort. Inpatient and outpatient medical charts and imaging were reviewed for patient characteristics, presenting symptoms and signs, procedural findings, and outcomes.
We have previously described our criteria for diagnosis, VSS treatment, and follow-up.11 Briefly, angiography was offered to patients with signs and symptoms suggestive of IIH, including severe headaches, visual disturbance, and evidence of increased intracranial pressure by lumbar puncture or intracranial pressure monitoring. Patients who were found to have evidence of ≥50% intracranial venous sinus stenosis associated with a trans-stenosis pressure gradient of ≥8 mm Hg on diagnostic venous manometry were offered VSS. VSS was also offered to some patients with severe symptoms and evidence of significant intracranial venous sinus stenosis, even if the trans-stenosis pressure gradient was <8 mm Hg. In four cases in which multiple segments of stenosis were seen, longer stent constructs, spanning from the superior sagittal sinus (SSS) through the dominant sigmoid sinus, were placed.
Our VSS procedure has been described in detail in a previous report.11 VSS was performed using Zilver biliary (Cook Medical, Winston-Salem, North Carolina, USA), Protégé Everflex peripheral (Covidien, Dublin, Republic of Ireland), or Precise carotid (Cordis, Hialeah, Florida, USA) self-expanding bare metal stents. All patients were placed on dual antiplatelet therapy (aspirin 325 mg and clopidogrel 75 mg daily) prior to the VSS procedure. Aspirin (ASA) and P2Y assays were checked on the morning of the procedure, and patients who were subtherapeutic were administered either clopidogrel 150 or 300 mg (for P2Y >208) or ASA 600 mg (for ASA >551). Patients were maintained on dual antiplatelet therapy for at least 1 month, and then monotherapy with aspirin 325 mg daily for at least 3 months after the procedure. Follow-up angiography was performed 3 months after VSS, except in cases of early recurrence or worsening of symptoms.
Evaluation of VOL patency and SAS
Evaluation of VOL patency was performed by retrospective review of diagnostic cerebral angiography in the venous phase. Images and fluoroscopic loops were reviewed to evaluate venous anatomy and contrast transit time. VOL was identified on pre-procedure diagnostic angiography. Classification of VOL filling after stent placement was made in comparison with baseline and was divided into four categories: normal filling; diminished caliber with normal transit time; sluggish flow, which was associated with diminished caliber; and occluded, if no flow was observed. SAS was defined as venous sinus stenosis occurring distal to a previously placed stent, requiring additional VSS. Within the venous system, proximal is defined as closer to the heart and distal is defined as further from the heart.
Statistical analysis
Data are presented as mean (range) for continuous variables and as frequency for categorical variables. The comparison of outcomes was performed using Pearson's χ2 and Fisher's exact tests, as appropriate. p Values<0.05 were considered statistically significant. Statistical analysis was carried out with GraphPad Prism V.7.0 (GraphPad, San Diego, California, USA).
Results
During the study period a total of 80 patients underwent VSS. Of these, 56 patients underwent placement of stents spanning from the transverse to sigmoid sinus and were included for analysis. Analysis of long-term VOL patency was performed for patients with angiographic follow-up of at least 3 months (n=46 evaluable patients). The mean duration of angiographic follow-up was 7.2 months (range 3–23 months).
Table 1 summarizes the patient demographics and angiographic findings of the venous stenoses. A total of 79 stents were placed in the 56 patients included in the study cohort, with a mean number of stents per patient of 1.4. The ostium of the VOL was covered by the stent in 52 patients. One patient received bilateral TS stents at one procedure and the VOL was covered on both sides; the total incidence of stent coverage of the VOL was 53 of 57 stents placed (93.0%).
Summary of patient demographics and angiographic findings
Table 2 details the patency of the VOL immediately after VSS and at follow-up. Immediately following VSS, venography was performed in 32 cases. Normal filling of the VOL was seen in 24 cases (75.0%), diminished caliber of the VOL with normal transit time was seen in one (3.1%), sluggish flow of the VOL with diminished caliber was seen in six (18.8%), and the VOL was occluded in one (3.1%). Among 19 patients with normal filling of the VOL immediately after VSS in whom there was an evaluable follow-up diagnostic angiogram, 17 maintained normal flow (89.5%) at follow-up.
Status of VOL before and after venous sinus stenting
Over time, flow through the VOL tended to partially improve in patients with altered drainage patterns. Of the six cases with sluggish flow immediately after VSS, four improved at follow-up, with diminished flow but normal transit time, and one patient improved to normal VOL filling. One patient with initially sluggish filling of the VOL went on develop VOL occlusion at follow-up. The patient with occlusion immediately after stent placement improved and was seen on follow-up angiography to have diminished flow but normal transit time. While >20% of patients had evidence of sluggish or occluded VOL, none of these patients experienced neurological sequelae from alterations in VOL drainage pattern or VOL occlusion.
We compared the patency of the VOL between patients who developed SAS requiring an additional VSS procedure and those who did not (table 2). Among 32 patients in which immediate post-stent angiography was performed, SAS was seen in 9 patients (28.1%); among 50 patients with follow-up angiography, SAS was seen in 12 patients (24.0%). Overall, SAS occurred in 15 patients (26.7%). SAS occurred in 7.1% of cases in which the stent covered the VOL and in 6.7% of cases in which the stent did not cover the VOL (p>0.999). In some cases, venography only was performed at either stent placement or follow-up, explaining the difference in denominator for these time points. In all cases, SAS occurred distal to the initial stent, either within the TS or SSS. There were no cases of in-stent stenosis or thrombosis. There were no significant differences between the patients with or without SAS requiring additional VSS in coverage of the VOL (p>0.999), or in VOL drainage patterns immediately after VSS (p=0.831) or at follow-up (p=0.231). Representative cases of normal and compromised filling of the VOL after VSS are depicted in figures 1 and 2, respectively.

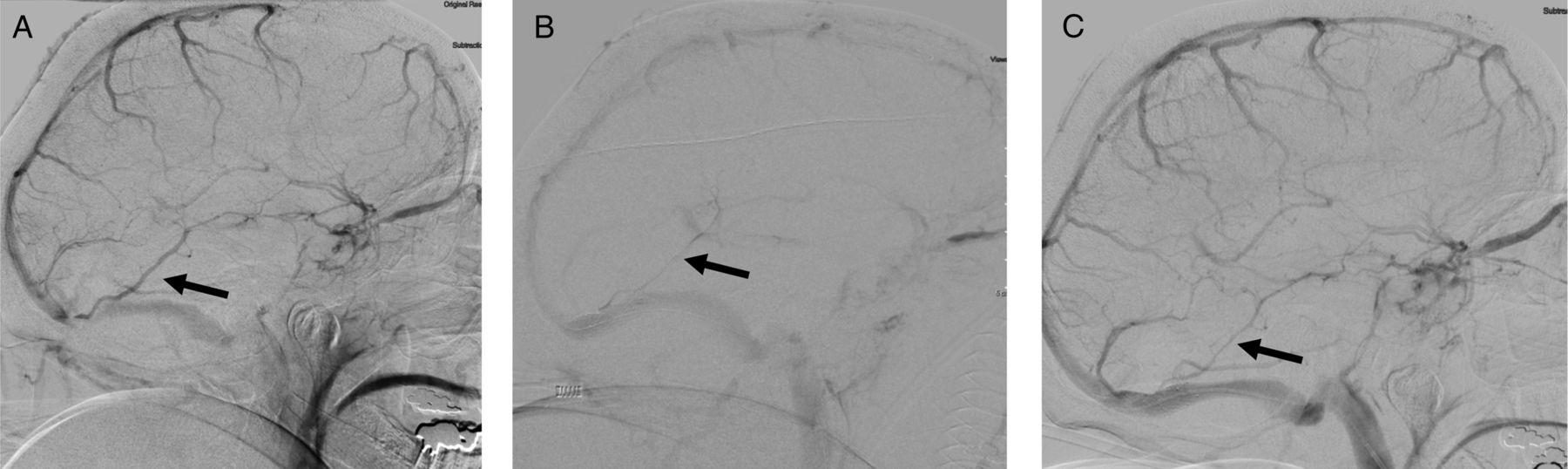
A patient with IIH was found to have elevated mean venous pressure and a focal stenosis at the right transverse–sigmoid sinus junction (TSJ), with an associated pressure gradient of 45 mm Hg. (A) Diagnostic angiography, lateral view of a right internal carotid artery (ICA) injection in the venous phase, performed during diagnostic investigation, shows the vein of Labbé (VOL) (arrow). (B) Post-stenting angiography, lateral view of a right ICA injection in the venous phase, performed immediately after placement of a stent spanning the right TSJ, shows normal filling of the VOL with normal transit time. (C) Follow-up angiography performed 6 months after stent placement, lateral view of a right ICA injection in the venous phase, shows normal filling of the VOL with normal transit time.
{kind=link}
{kind=link}
A patient with IIH was found to have elevated mean venous pressure and a focal stenosis in the dominant distal right transverse sinus, with an associated pressure gradient of 16 mm Hg. (A) Diagnostic angiography, lateral view of a right internal carotid artery (ICA) injection in the venous phase, shows the vein of Labbé (VOL) (arrow). (B) Post-stenting angiography, lateral view of a right ICA injection in the late venous phase, performed immediately after placement of a stent spanning the right transverse–sigmoid sinus junction, shows diminished caliber of the VOL, with sluggish flow and delayed transit time. (C) Follow-up angiography performed 6 months after stent placement, lateral view of a right ICA injection in the venous phase, shows improved filling of the VOL with persistently diminished caliber of the vessel.
Discussion
VSS is becoming an increasingly used treatment option for intracranial venous stenosis in the setting of IIH and related pathologies.1 ,6 ,12 Although other therapies are available, VSS is a reasonable alternative that may address a key pathophysiologic component in patients with IIH, demonstrable venous sinus stenosis, and an associated trans-stenosis pressure gradient. Most venous stents placed across the TSJ cover the ostium of the VOL and many other large cortical draining veins as they enter the dural sinuses,7 ,8 but the effect of this on the drainage pattern of the VOL has not been well characterized. Thrombosis or occlusion of the VOL, especially in the acute setting, can lead to life-threatening complications including venous infarction, hemorrhage, and seizures.13–17 These complications have not, however, been reported after VSS. Nevertheless, the results of our study indicate that stent placement does cause both immediate and long-term hemodynamic changes in the cortical and dural venous systems, which can lead to a change in the VOL drainage pattern in a moderate proportion of cases.
Our results are in contrast to a recent series which reported no changes in the drainage pattern of the VOL after VSS.7 Despite anticoagulation, the VOL did demonstrate changes immediately and at follow-up in 25% and 29% of cases in our study cohort, respectively. All patients received a standard anticoagulation regimen, and additional antiplatelet agents were administered for patients who were subtherapeutic based on ASA and P2Y levels. Although initially requiring patients to continue indefinitely on ASA 325 mg daily, we have not observed any cases of in-stent stenosis or stent thrombosis and have therefore begun limiting the requirement for antiplatelet coverage to a total of 3 months. Additionally, changes in drainage patterns occurred between stent placement and follow-up, typically with increased flow within an initially sluggish and small VOL. It is likely that the vessel remained open and demand-related changes may have led to increased filling over time. Despite these hemodynamic changes, we found no correlation between changes in VOL drainage pattern and SAS requiring additional VSS in our analysis, indicating that compensatory drainage patterns may develop. Furthermore, despite covering the dominant VOL in 71.4% of cases, symptomatic VOL occlusion did not occur in any case in our series.
The venous phase of the cerebral angiogram is often more difficult to interpret, and the ability to image small cortical veins remains suboptimal in some cases. Stents commonly used in VSS procedures include peripheral biliary, iliac, and carotid bare metal stents. These generally vary between an open cell and a semi-closed cell design, with similar degrees of vessel coverage between stent designs. Among patients with diminished caliber or sluggish flow after VSS, we did not find any significant differences between patients who received open cell or semi-closed cell stents. In the majority (78.6%) of cases in our series, the ostium of the VOL was very close (<1 cm) to the area of stenosis. Theoretically, atheroma from the area of stenosis may be pushed into the ostium of the VOL in these cases by the stent as it expands. Among the patients with VOL >1 cm from the area of stenosis, all patients had normal VOL filling at follow-up compared with 66.7% of those with VOL <1 cm from the stenosis. This difference did not reach statistical significance (p=0.167).
As with all retrospectively analyzed data, our report is subject to the limitations of potential selection and inclusion biases as well as abbreviated follow-up in some cases. We did not perform post-stenting control arteriography in 43% of cases as venography was often performed immediately following stent placement. This may skew our findings regarding VOL patency immediately after VSS. Nevertheless, our results do suggest that hemodynamic changes after VSS can result in both immediate and delayed alterations in the drainage pattern of the intracranial venous system. Further studies are necessary to discern the long-term effects of VOL coverage by venous stents and the neurological consequences of changes to VOL drainage patterns.
Conclusions
Stent coverage of the ostium of the VOL occurs in the majority of VSS procedures involving the transverse and sigmoid sinuses. In our cohort, stent coverage of the ostium of the VOL caused changes in the venous drainage pattern in the VOL in 25% of cases initially, and in 28.5% of cases on follow-up angiography. No significant correlation was found between altered venous drainage and clinical or procedural outcomes.
References
Footnotes
Contributors DMSR conceived the study, performed data analysis, drafted the manuscript, and approved the final version of the manuscript. DD and TJB assisted in data analysis, critically revised the manuscript, and approved the final version of the manuscript. CJ-C assisted in writing the manuscript, critically revised the manuscript, and approved the final version of the manuscript. RWC oversaw data collection and analysis, critically revised the manuscript, and approved the final version of the manuscript. KCL contributed to the design of the study, oversaw data collection and analysis, critically revised the manuscript, and approved the final version of the manuscript.
Competing interests None declared.
Ethics approval University of Virginia Institutional Review Board for Health Sciences Research.
Provenance and peer review Not commissioned; externally peer reviewed.