Article Text

Abstract
Background Some patients undergoing dural sinus stenting for idiopathic intracranial hypertension (IIH) develop clinical and hemodynamic failure (recurrence of the pressure gradient) owing to stent-adjacent stenosis.
Objective To characterize factors associated with hemodynamic failure, and to describe outcomes of patients after repeat stenting.
Materials and methods We reviewed the initial and follow-up clinical, venographic, and hemodynamic data in 39 patients with IIH treated over 17 years with stenting. Thirty-two had follow-up angiographic and hemodynamic data at 1–99 months (mean 27.6, median 19.5 months). Eight patients were treated with 12 repeat stenting procedures, including extended stenting into the superior sagittal sinus (SSS).
Results All patients had an initial successful hemodynamic result with the pressure gradient reduced from 10–43 to 0–7 mm Hg. 10/32 patients (31.3%), all women, developed new stenoses in the transverse sinus or posterior SSS above the stent with a recurrent pressure gradient. 7/9 patients with pure extrinsic stenosis of the transverse-sigmoid junction pre-stenting developed new stenoses and hemodynamic failure. All patients with hemodynamic failure who were restented had early and mid-term documented hemodynamic success at 1.7–50 months. They were free from papilledema at 3.8–50 months after the last restenting, and 11.5–99.5 months after initial stent placement (mean 45.3, median 38.5 months).
Conclusions Pure extrinsic compression of the transverse-sigmoid junction and female gender were strongly associated with hemodynamic failure. Eight patients with hemodynamic failure who were restented had successful control of papilledema, including 4/4 who had extended stenting into the SSS.
- Intervention
- Intracranial Pressure
- Stenosis
- Stent
- Vein
Statistics from Altmetric.com
Introduction
Dural sinus stent placement in the transverse sinus and transverse-sigmoid junction uniformly provides initial control of papilledema in patients with idiopathic intracranial hypertension (IIH) who have papilledema and visual disturbance.1–3 Development of a new stent-adjacent stenosis in the transverse sinus above the stent has been noted in 11.5%,4 21.7%,5 and 35.7%6 of patients undergoing stent placement for IIH. Concurrent narrowing of the posterior superior sagittal sinus (SSS) has been reported in one patient.6 Comparison of pre-stenting clinical and venous manometric parameters in patients who were re-treated with those of patients with continuing hemodynamic success has been reported by two groups.4 ,7 There were differences in age, body mass index (BMI), opening pressures (OPs) on lumbar puncture (LP), mean SSS pressures, and pressure gradients between the SSS and the internal jugular vein.
Our clinical protocol is to perform follow-up angiographic and venous manometric studies on all patients after stent placement. We have observed a higher incidence of stent-adjacent stenosis than those reported by most investigators, and found that the intracranial venous pressure gradient recurs across the new stenosis. We have called this phenomenon ‘hemodynamic failure’. We have also found different factors associated with hemodynamic success versus failure.
Concurrent narrowing of the posterior SSS can occur as part of the failure anatomy. Most patients with hemodynamic failure have been treated with restenting of the transverse sinus or shunting.4–11 We have treated eight of 10 patients with hemodynamic failure with restenting, including extended stenting into the SSS. To our knowledge, stenting into the SSS for this condition has been described in one patient with a 3-month hemodynamic follow-up (Abraham MG, personal communication, 2016).6
We aimed to analyze the factors associated with hemodynamic failure after the initial stent placement, and to describe our experience with the use of stenting to treat patients with hemodynamic failure for whom maximum medical therapy had failed after the initial stent procedure.
Materials and methods
Study design and sample
This study was reviewed and approved by the Colorado multi-institutional review board. We assembled a retrospective cohort of 39 consecutive patients treated with 51 stent placement procedures between February 1999 and July 2016. There were 28 women and 11 men, ranging in age from 16 to 62. All patients had a history of papilledema. Thirty-seven of 39 patients had papilledema at the time of stenting, with or without optic atrophy; 27/28 women and 4/11 men had headache. Duration of symptoms ranged from 3 weeks to 20 years (median 24 months). All patients had had LPs before stenting. OPs were 30–60 cm H2O in 30, 25–29 cm H2O in five; four others had OPs recorded in their charts as ‘elevated’.
Mean BMI was 33.68 (median 33.9). BMI was ≥30.0 (obese) in 26/39 patients (66.7%) and >25.0 (overweight+obese) in 34/39 (87.2%).
Patient selection criteria for initial stent placement were (1) diagnosis of IIH; (2) presence of documented papilledema; (3) lumbar puncture opening pressure (LP OP) ≥25 cm H2O; (4) presence of stenoses at both transverse-sigmoid junctions or at a single transverse-sigmoid junction if the contralateral sinus was absent; (5) a pressure gradient of ≥10 mm Hg across the transverse-sigmoid stenosis. Hemodynamic success both initially and at follow-up was defined as reduction of the pressure gradient to <10 mm Hg. Criteria for repeat stenting were (1) redevelopment of a recurrent pressure gradient >10 mm Hg and (2) recurrence of papilledema, significant visual disturbance, or severe new headache.
Clinical procedures
The procedures were initially performed under general anesthesia but more recently with monitored awake sedation after we modified our technique from our previous report.12 We now leave a 7F Shuttle sheath (Cook Inc, Bloomington, Indiana, USA) in the internal jugular vein. We measure the pressure gradient initially between the internal jugular vein just below the jugular foramen and the anterior SSS using a 0.027 microcatheter. For stent placement we advance a softer, lower-profile conduit catheter, either a Navien 072 (Medtronic Neurovascular, Irvine, California, USA) or Neuron 070 (Penumbra, Inc, Alameda, California, USA), through the Shuttle sheath into the transverse sinus over the inner coaxial 0.027 microcatheter. This is tolerated by most patients without need for general anesthesia, which we now use infrequently. The stent is then advanced into position through the conduit catheter. Since 2010 we have stented the full length of the transverse sinus into the upper sigmoid sinus, as also advocated by Ahmed et al.4 We have used Zilver stents (Cook, Inc) exclusively since 2007. For treatment of the patients with hemodynamic failure, we restented the transverse sinus in four and extended stents into the SSS in four.
Follow-up
Patients are followed up by our neuro-ophthalmology service every 4–12 weeks until the papilledema has resolved and visual function is stable, and at least annually until their syndrome resolves. Our angiographic protocol is to perform the first follow-up study at 6 months after stenting unless there is suspicion of an early hemodynamic failure, then at 2 years, then at least every 5 years unless new symptoms develop. Patients with hemodynamic failure are followed up at 3 months after restenting and every 6–12 months after that, until we document that the restenting was hemodynamically successful for at least 12 months.
Statistical analysis
To evaluate patient factors associated with hemodynamic failure, we used Wilcoxon–Mann–Whitney tests to evaluate differences in continuous variables and Fisher's exact tests to evaluate differences in categorical variables. We used a type I error rate of 0.05 for all tests. SAS V.9.4 software (SAS Institute, Cary, North Carolina, USA) was used.
Results
Technical success was achieved in all 39 patients with an initial gradient decrease between the torcular or SSS and the internal jugular vein to <10 mm Hg.
All patients had either narrowing at both transverse-sigmoid sinus junctions, or an absent or hypoplastic transverse sinus on the side opposite to the stented side. Thirty patients had a dominant sinus (23 right, 7 left). The dominant transverse-sigmoid sinus was stented except for one early case.
Pretreatment pressure gradients across the stenoses at the transverse-sigmoid junction ranged from 10 to 43 mm Hg, and pre-stent pressures in the SSS or the torcular varied from 18 to 49 mm Hg. The pressure gradients after stent placement varied from 0 to 7 mm Hg.
Hemodynamic success initially and at follow-up was defined as a pressure gradient of <10 mm Hg between the torcular or SSS above the highest stent and the internal jugular vein.
Complications
There were two major and three minor complications among the 39 patients during 51 stenting procedures. We have previously reported the major complication of a subdural hematoma and subarachnoid hemorrhage, managed with placement of a temporary external ventricular drain, after which the patient made a complete recovery.12 The other major complication was non-occlusive clot formation after post-stent percutaneous transluminal angioplasty at the lower end of the stent, which was successfully lysed with a 16-hour local infusion of tissue plasminogen activator. This patient had no clinical symptoms. One patient had two minor complications—a urinary tract infection and a syncopal episode during transfer to a chair the day after stent placement. Another patient awoke from anesthesia with transient disorientation, which was attributed to an idiosyncratic reaction to propofol. There were no permanent sequelae of any complication and no complications in the restenting procedures.
Clinical follow-up
The 39 patients had a total clinical follow-up of 1042.9 months. Mean follow-up was 26.7 months, median 15 months. One subject is due for his first follow-up at the time of this writing. Six patients had clinical follow-up at 0.5–5.5 months. Two of these were lost to follow-up after 1 month. Thirty-two patients had clinical follow-up ranging from 6 to 136 months, mean 32.3, median 21.4. Fifteen patients had follow-up >2 years, mean 54.9 months.
Documented resolution of papilledema occurred in 33 patients. Of the remaining six, direct examination was not available in two patients, but visual symptoms had disappeared and the follow-up transcatheter pressure gradients were 3 mm Hg in both. Two other patients had resolving papilledema at 0.4 and 1 month after stenting. One patient had no available follow-up information at 9 months after stent placement. Only one patient, who had hemodynamic failure and was not re-treated, had persistent papilledema. No other patient had further visual deterioration after stenting.
Headache resolved in one of four male patients who had initial headaches; three had persistent unchanged migraine headaches. One man, recently stented, has had no follow-up as yet. The six remaining men had no headaches before or after stenting. Among 28 women, one had no headaches. In the remaining 27, headaches were resolved in seven (25.9%), improved but persistent in 15 (55.6%), unchanged in five (18.5%). Thus, 74.1% of women and 27.2% of men with headaches had persistent headache in some form after stent placement.
Angiographic follow-up
Follow-up angiographic studies were performed in 32/39 patients (82.1%). Of the seven without a follow-up, one patient did not return, one moved to another city before angiographic follow-up, four had had stenting procedures within ≤6 months, and one at 9 months. Eighty-six follow-up angiograms and two CT angiograms were obtained at 1–99 months. Total angiographic follow-up was 893.9 months, mean 27.6, median 19.5.
All stents remained patent with no in-stent restenosis. All veins of Labbe remained patent. One patient with coagulopathy, previously reported,12 developed thrombosis of the sigmoid sinus below the stent 67 months after stent placement and 1 month after a stillbirth. This was successfully cleared using catheter-directed thrombolysis, with continued patency and hemodynamic success at 99 months and without papilledema at 136 months after stent placement.
Hemodynamic follow-up was available in 31 patients, 9 men and 22 women. The first patient in this series had angiographic follow-up at 60 months in another city without hemodynamic measurements, which showed stent-adjacent stenosis above the stented transverse-sigmoid junction. In clinical follow-up she had recurrent papilledema with LP OP of 36 cm H2O at 2.5 years after stent placement. She underwent multiple shunt procedures before and after stenting without relief of her papilledema. We classified this patient as having a hemodynamic failure despite the lack of hemodynamic measurements. We therefore analyzed follow-up hemodynamic and angiographic data in 32 patients, 23 women and 9 men.
Twenty-two of the 32 patients (68.8%) had hemodynamic success while 10 patients (31.3%), had hemodynamic failure with recurrence of a pressure gradient >10 mm Hg. Two had persistent filling defects in the transverse sinus above the stent, one a kink just medial to the stent, and seven a new stenosis above the upper end of the stent due to extrinsic compression. All 10 hemodynamic failures occurred in the 23 women (43.5% of women). Five of these redeveloped papilledema and another had rapidly worsening visual fields without an examination for papilledema. The recurrent gradients were higher than the initial gradient in four patients by 5–11 mm Hg, less than initial gradient in four patients by 3–12 mm Hg, and the same in one patient.
We evaluated differences between the success/failure groups (table 1). Patients who experienced hemodynamic failure were significantly younger (p=0.04), and had higher LP OP (p=0.02). They did not differ significantly with respect to SSS pressure (p=0.76), pressure gradient (p=0.79), BMI (p=0.17), or internal jugular vein pressure (p=0.32) in comparison with patients with hemodynamic success.
Comparisons of hemodynamic successes (n=22) with hemodynamic failures (n=10)
We analyzed the types of pre-stenting narrowing at the transverse-sigmoid sinus junction before stent placement in our entire 39 patient cohort and for the 32 patients with angiographic/hemodynamic follow-up (table 2). We classified the narrowing in the stented sinus as intrinsic (filling defect within the lumen), extrinsic (external compression of the transverse-sigmoid junction alone with no intrinsic filling defect), or extrinsic+intrinsic (external compression of the transverse-sigmoid junction with an intrinsic defect in addition).4 ,13 ,14 In the entire 39 patient cohort, 10/11 (90.9%) men had an intrinsic lesion, while 18/28 (64.3%) women had an intrinsic lesion, the majority of these (11/18) with an accompanying extrinsic stenosis.
Comparison of types of pre-stenting narrowings at the TS–SS junction(s) by gender and in hemodynamic successes and hemodynamic failures
Of the women who developed hemodynamic failure, 3/10 had extrinsic+intrinsic stenoses. Two of these had residual filling defects above the initial stent. One was shown in our previous report.12 One woman with extrinsic+intrinsic stenoses initially, had a high bifurcation of the SSS, with vertical segments of transverse sinus before they turned horizontally at the level of the torcular. The stent was positioned in the right transverse sinus with its upper end at the curve. She developed kinking of the sinus at the upper end of the stent at the junction of the horizontal and vertical segments of the transverse sinus with recurrence of the pressure gradient across the kink.
Nine patients, one man and eight women, had extrinsic compression. Seven of nine patients with extrinsic compression, all female, developed hemodynamic failure after stent placement. Three had initial stenting of the transverse sinus–sagittal sinus junction only. All three developed new narrowing of the ipsilateral transverse sinus, tapering from the torcular to the upper end of the stent (figure 1A, B). Two of them had restenting of the remainder of the TS to the torcular (figure 1C). The third was our first patient, described above. She had moved out of the state before we had experience with restenting.

Patient 18. Patient with idiopathic intracranial hypertension and papilledema. Recurrent stenoses after stenting. (A) Before the initial stent. Typical scalloped stenosis on the superior medial transverse-sigmoid junction (black arrowhead), indicating extrinsic compression. Transverse sinus has normal caliber. ΔP=22 mm Hg. Arrows show the sites of pressure measurement. (B) After the first stent. ΔP=1 mm Hg. Transverse sinus above the stent remains of normal caliber. (C) Hemodynamic failure 10.5 months after the first stent. New tapered narrowing of the right transverse sinus, maximum just above the stent (black arrowhead). ΔP=33.5 mm Hg. (D) After stenting of the entire transverse sinus with a second stent. ΔP=5 mm Hg. Posterior superior sagittal sinus remains of normal caliber (black arrowhead). (E) Second hemodynamic failure 7.5 months after the second stenting. New narrowing of the posterior superior sagittal sinus above the second stent (black arrowhead) with new pressure gradient. ΔP=16 mm Hg.
In 2010, after we detected the failure pattern of new narrowing of the TS above the stent, we modified our stent placement protocol. In 20/21 patients stented since then, the entire TS through the upper sigmoid was covered by the stent. Including the two patients who had stenting of the entire TS in two procedures, there were five women with initial extrinsic compression of the transverse sinus–sagittal sinus junction who underwent stenting of the entire TS (table 4). All of these subsequently developed new fusiform stenoses owing to extrinsic compression of the posterior SSS and contralateral TS with recurrence of the pressure gradient (figure 1D, E).
Statistical tests for differences in hemodynamic factors for all hemodynamic successes versus hemodynamic failures are presented in table 3. Patients with hemodynamic failure were more likely to be female (p=0.003) Angiographically they were more likely to have extrinsic stenosis (p=0.0002), than patients who did not experience hemodynamic failure.
Comparisons of hemodynamic failures (n=10) to successes (n=22)
Restenting
Eight of the 10 patients with hemodynamic failure underwent 12 repeat stenting procedures. Technical success was accomplished in 11/12 restenting procedures, with a decrease in the pressure gradient to <10 mm Hg. One technical failure was due to measurement of the poststenting gradient too close above the new stent (figure 2).
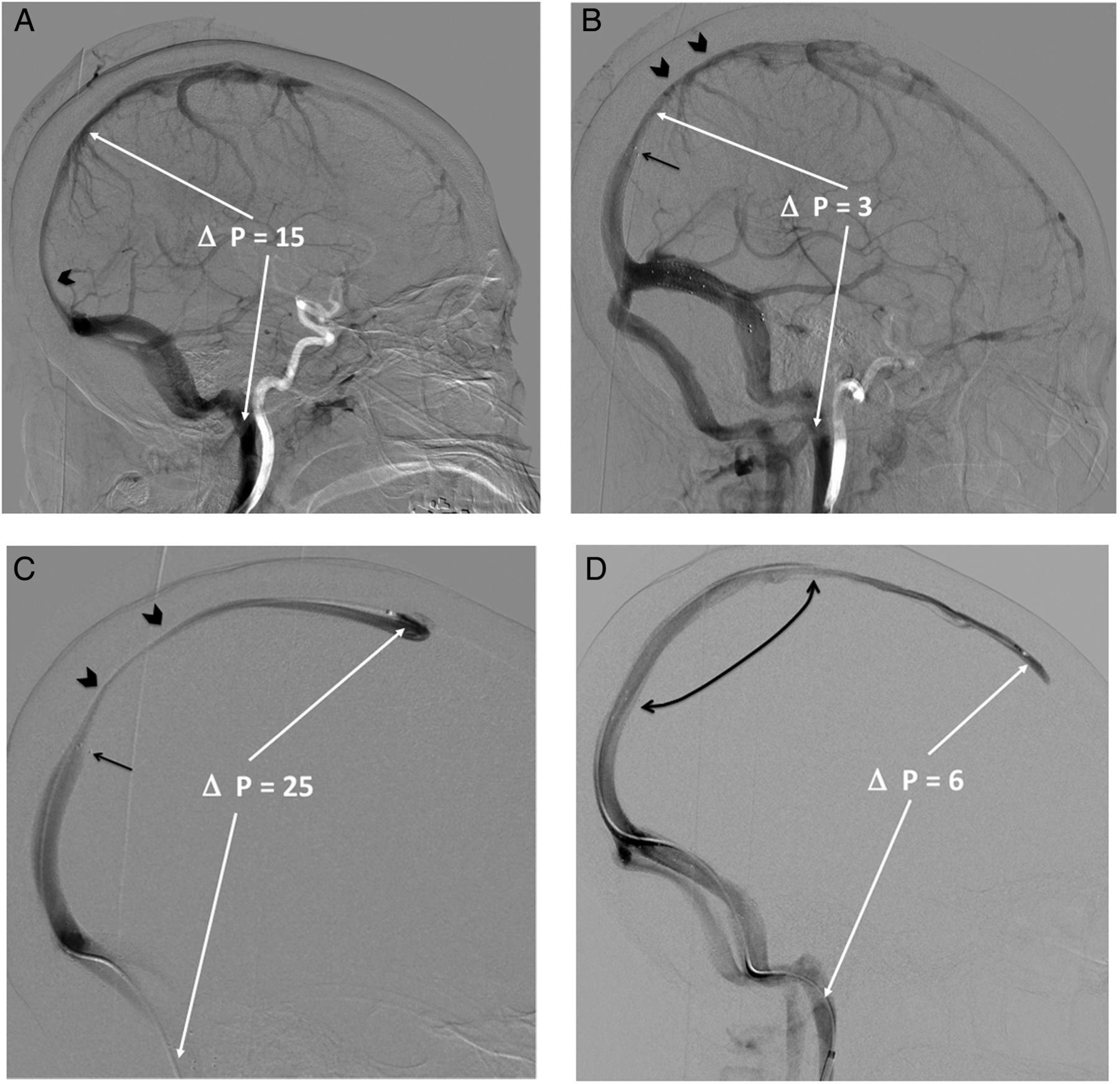
Patient 21. (A) Patient now 17 months after the first stent placement in entire transverse and upper sigmoid sinuses. Papilledema regressed after stenting but with permanent visual compromise in one eye. Patient was referred for urgent repeat study because of increasing visual disturbance without re-examination for recurrent papilledema. Venous phase of RICA angiography showing narrowing of the posterior superior sagittal sinus (SSS) due to extrinsic compression (black arrowhead) which had not been present initially. White arrows indicate the sites of pressure measurements. ΔP=15 mm Hg. (B) Immediately after the second stent deployment (upper end indicated by black arrow). ΔP=3 mm Hg with pressure measurement obtained above the uppermost stent. There is residual narrowing of the SSS above the point of pressure measurement (black arrowheads). In retrospect, the pressure gradient would probably have been measured as higher if pressure had been measured in the anterior SSS. (C) SSS venography 4 days after the second stent deployment. The patient's symptoms did not improve, prompting restudy. The degree of narrowing of the SSS (black arrowheads) has increased above the end of the upper stent (black arrow). Pressure gradient between the anterior SSS and the internal jugular vein measured 25 mm Hg. (D) 26 Months after deployment of another stent above the second stent (curved black arrow—ends of the third stent). Patient has no papilledema. SSS is widely patent. ΔP=6 mm Hg.
Two patients with a residual intrinsic filling defect in the transverse sinus above the initial stent underwent stenting of the remainder of the transverse sinus to the torcular, covering the residual defect. These two patients remained hemodynamic successes on follow-up angiography at 3 and 15 months after placement of the second stent, and free from papilledema at 8 and 44 months after placement of the second stent. One patient with kinking at the upper end of the stent had a normal pressure gradient at 6 weeks after the second stent placement in the contralateral mid-transverse+upper sigmoid sinus and was free from papilledema at 3.8 months after the second stenting.
Five restented patients had initial extrinsic compression (table 4). They had stenting of the entire TS in one or two procedures, then developed a new fusiform narrowing of the posterior SSS with a recurrent gradient. One of these had a pressure gradient of 16 mm Hg across the new narrowing (figure 1E), with an increase in her migraine headaches but no definite papilledema, so did not have restenting into the posterior SSS. The pressure gradient decreased spontaneously to 5 mm Hg at 24.5 months despite the lack of apparent change in the angiographic appearance of the narrowing. She had no visual disturbance but continuing headaches at that time.
Patients with extrinsic stenosis only
The other four patients with the full length of the transverse sinus stented had eventual extension of one to three stents through the new narrowing in the posterior SSS. In one of these, restenting into the posterior SSS across the new narrowing sufficed; the patient was free from papilledema and had a normal pressure gradient between the anterior SSS and the internal jugular vein 50 months after restenting. In the other three patients new stenoses developed in the SSS above the stent in the posterior SSS. In two of these, extension of stents into the mid-SSS in a second restenting procedure was successful (figure 2A–D).
One patient required stenting of the entire SSS (figure 3) in three restenting procedures. Initial stenting and two restenting procedures over 2 months failed to improve her papilledema. Each stenting procedure produced a normal pressure gradient; the elevated gradient then recurred within 4–6 weeks owing to a new stenosis in the SSS above the stent. Her papilledema continued and she had worsening vision loss. Shunting was considered but rejected. A third restenting procedure was performed via a right internal jugular access, extending into the anterior SSS. Pressure gradient between the anterior SSS and the right internal jugular vein remained normal (5 mm Hg) 1 month (figure 3D) and at a second measurement (4 mm Hg) 10.4 months after this stent placement. Her papilledema resolved by 3 months after the last stent, and remained resolved at the last follow-up 10 months after the last stent placement.

{kind=link}
{kind=link}
{kind=link}
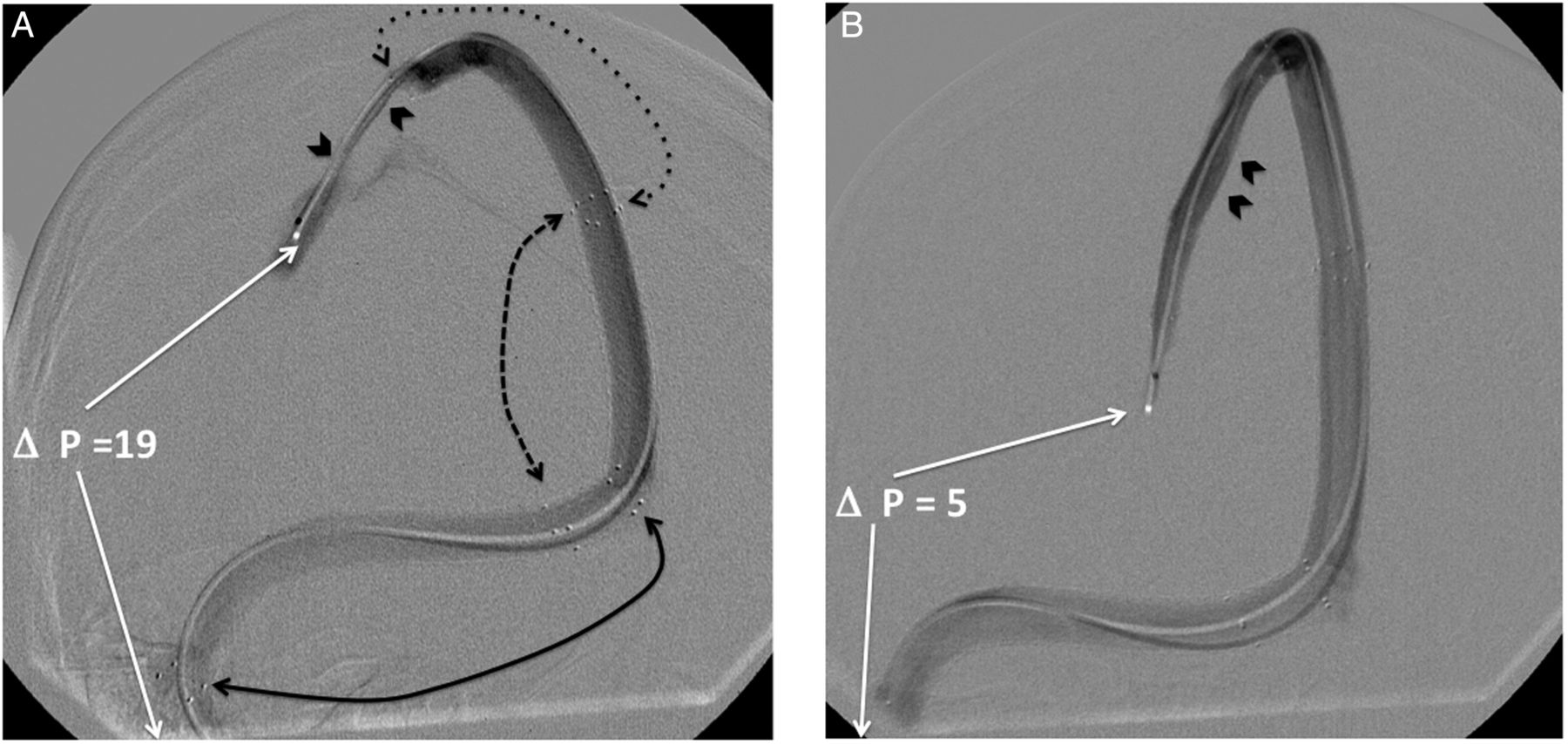
Patient 33. Patient s/p urgent optic nerve sheath fenestration with continued papilledema, worsening vision, and headache. She underwent three stent placements, and after each restenting developed hemodynamic failure within 4–6 weeks owing to development of a new narrowing above the upper end of the stent. There was a temporary decrease in the pressure gradient after each stenting, but papilledema did not regress. (A) 6 Weeks after second restenting to the mid-superior sagittal sinus (SSS). Black solid and dashed curved arrows show the ends of the three stents. There is a new focal narrowing of the SSS above the upper end of the newly placed stent (black arrowheads). Patient had continuing papilledema and headaches. ΔP between the anterior SSS and internal jugular vein (IJ) was 19 mm Hg. (B) SSS venogram 4 weeks after the patient underwent a third restenting extending into the anterior SSS. Her papilledema finally regressed after this restenting. There is no new or residual stenosis in the SSS. Arrowheads mark the location of the focal stenosis seen in (A). ΔP between the anterior SSS and the IJ was 5 mm Hg at four weeks, and 4 mm Hg with an identical venographic appearance at 10.4 months after the last restenting. Patient had no papilledema at 10 months after third restenting, but had continuing headaches. There was no control of papilledema until the entire SSS was stented.
In the eight restented patients, the time to the second stent placement ranged from 1.3 to 62 months (mean 16.3 months). The minimum time from stent placement with a normal post-stenting gradient to detection of a recurrent high gradient was 30 days. In the five restented patients with extrinsic-only compression, the mean time to second stent placement varied from 1.3 to 17.5 months.
Follow-up after restenting
To date, all eight patients who underwent one or more restenting(s) for hemodynamic failure were hemodynamic successes at the last hemodynamic follow-up, 1.7–50 months after placement of the last stent. The four patients with extension of the stents into the SSS have normal pressure gradients at 10.3, 23.5, 25.7, and 50 months after placement of the SSS stent(s). All restented patients are free from papilledema at clinical follow-up 3.8–50 months after the last stent. Patients with extension of the stent into the SSS are free from papilledema at 10, 24.7, 25.7, and 50 months after placement of the last stent.
From the initial stent placement, all eight patients with hemodynamic failure who were treated only with restenting have normal pressure gradients at hemodynamic follow-up of 12–98 months after the initial stent placement (mean 43.1, median 33.1 months), and are free from papilledema 11.5–99 months after initial stent placement (mean 45.3, median 38.5 months).
Discussion
This retrospective cohort study found that all dural sinus stents remained patent without in-stent restenosis. All veins of Labbe remained patent, as in the report by Levitt et al.15 Patients who experienced subsequent hemodynamic failure were significantly younger and had higher LP OP than patients who did not. A significantly higher proportion of patients with extrinsic stenosis experienced hemodynamic failure compared with patients with intrinsic stenosis. All failures occurred in women, and there was a statistically significant difference in hemodynamic failure by sex.
Development of a new stenosis after stent placement has been recognized by multiple investigators.3 ,5 ,6 ,12 ,16 Although in-stent stenosis occurs rarely,5 the majority of stenoses occur owing to collapse of the transverse sinus above the upper end of the stent.4–6 ,12 A review of 17 series by Starke et al3 summarized 185 patients. Six patients (3.4%) developed in-stent stenosis and stent-adjacent stenosis occurred in 19 patients (11.4%). In a recent series, Smith et al6 found an incidence of 35.7% of stent-adjacent stenosis in follow-up. Other series report re-treatment rates, which suggest hemodynamic failure, without indicating the associated angiographic findings. Satti et al17 in a recent meta-analysis found a repeat procedure rate of 10.3%. Three recent series noted re-treatment rates, of 16.7%,7 21.7%,5 and 33%.11 Digital subtraction angiographic follow-up of all or most stented patients has been performed by some investigators, including our group.5 ,6 ,9 ,12 Only one other group6 has reported follow-up intracranial pressure gradients. We found a higher proportion of new stent-adjacent stenosis in our patient cohort—31.25% overall and 43.5% among women—and documented their recurrent pressure gradients. We treated these patients with repeat stenting only, without shunting. Papilledema remains resolved in all restented patients with a normal pressure gradient in mid-term results.
Three of nine female patients with extrinsic+intrinsic stenosis (33.3%) developed hemodynamic failure. All of these could be attributed to operator error. In two, failure was due to an uncovered filling defect above the stent. Recurrent pressure gradients developed at 10.5 and 67 months after stent placement. These patients had their papilledema controlled with full-length stenting of the TS. These failures occurred before we began stenting the entire length of the transverse sinus to the upper sigmoid below the stenosis. This technique should eliminate hemodynamic failure due to this type of stenosis. A third patient with extrinsic+intrinsic stenosis had a high bifurcation of the SSS above the torcular, so that there were vertical and horizontal segments of both transverse sinuses. We had not encountered this anatomy previously in stent placement. She developed a kink at the stent junction with the vertical segment because the upper end of the stent was positioned too close to the curve, again an operator error.
In our 39 patients, intrinsic lesions were present in an overwhelming proportion of men (90.9%), and a majority of women (64.3%) with or without an accompanying extrinsic stenosis. All these patients had hemodynamic success after all the intrinsic lesions had been covered. If this observation is confirmed by other investigators, it suggests that patients with intrinsic stenoses, including nearly all men with IIH, should have a successful long-term outcome after stenting. We are aware of only one report, by Winters et al,18 of late hemodynamic failure in one patient with an initial intrinsic stenosis, a female subject who developed a new pressure gradient 5 years after stenting owing to development of a stent-adjacent stenosis of the medial transverse sinus from extrinsic compression. This was successfully restented.
Ten of 28 women (32.1%) and 1/11 men (9%) of our patient cohort had pure extrinsic stenosis, with no primary venous obstruction. These patients had a strikingly high hemodynamic failure rate—7/9 (78%)—due to new stent-adjacent stenosis. While all hemodynamic failures occurred in women, it may be that the differences in the frequency of hemodynamic failure between men and women in our population is due entirely to the rarity of pure extrinsic stenosis in men, most of whom have an intrinsic lesion (table 2). The one male subject with extrinsic-only compression had a BMI of 39.4. He had a normal pressure gradient (2 mm Hg) and persistent migraines 6 months after, and no papilledema 21 months after stenting. The remaining patients with extrinsic stenosis consist entirely of ‘typical’ patients with IIH—young and overweight women. Four of five of these eventually required extended stenting into the SSS to control their papilledema.
Two prior reports, with dissimilar results, discuss factors associated with hemodynamic failure. Ahmed et al4 restented 6/52 patients, all among 46 patients with papilledema. Five of 11 (45%) patients with extrinsic stenosis were restented, gender not specified. Patients who underwent restenting in comparison with those who did not, had higher mean lumbar cerebrospinal fluid (CSF) pressures, higher mean sagittal sinus pressures, and higher mean venous pressure gradients. Goodwin et al7 reported that three of 18 stented patients underwent subsequent CSF diversion. The patients with CSF diversion also had higher mean CSF pressures, but otherwise dissimilar clinical characteristics from the patient cohort of Ahmed et al—lower mean age, a higher BMI, but minimally lower initial pressures above the stenosis and pressure gradients across the stenosis. They did not report the type of pre-stenting stenosis. We found significant differences in age, LP OP, type of pre-stenting stenosis, and sex (tables 1 and 3). In all these experiences, there is more overlap of the clinical factors between the failure versus success groups than we found for the type of stenosis present at the transverse-sigmoid junction before stent placement.
The questions arise why stenting should be effective among patients who have no primary dural sinus obstruction, but rather whose dural sinus stenosis is due only to secondary extrinsic compression, and why stenting a new narrowing in a dural sinus previously documented to be of normal caliber should be effective. Ahmed et al16 and Halmagyi et al19 have suggested that impairment of CSF reabsorption, mainly at the level of the arachnoid villi in the SSS and other dural sinuses, is the common factor leading to development of the pseudotumor cerebri syndrome. Pickard et al20 demonstrated that pressure in the SSS and cerebrospinal fluid pressure are coupled. In an investigation of nine patients with IIH, CSF and SSS pressures were measured simultaneously. CSF pressure slightly exceeded SSS pressure. If CSF pressure was increased by infusing the CSF, the SSS pressure increased proportionally. If CSF pressure was decreased by drainage, the SSS pressure decreased proportionally down to central venous pressure, at which point it remained constant. This leads us to believe that normalization of pressure in the SSS is an important factor, perhaps the critical factor, in managing patients with IIH who have papilledema. The eight patients who had mid-term and long-term control of their papilledema all had normal pressure gradients between their SSS and their internal jugular vein.
We recommend that in all patients with IIH and papilledema who receive stent placement, the entire length of the transverse sinus extending into the sigmoid sinus should be stented. This will cover intrinsic lesions, which can be surprisingly subtle and difficult to detect, in that segment. Based on this early and limited experience, we cautiously recommend that extended stent placement may be a useful treatment in those patients whose entire transverse sinus has been stented, and who then develop hemodynamic failure due to narrowing of the posterior SSS. The extent of SSS which needs to be stented to maintain normal SSS pressures is an unanswered question. At last follow-up, normal SSS pressures were maintained with the upper end of the stent complex in the posterior SSS in one patient, in the mid-SSS in two patients, and in the anterior SSS in one.
We believe that extended stenting will prove to be a more durable and less costly treatment of hemodynamic failure than shunts, which have a high failure rate requiring revision.2 ,21 Ahmed et al8 have demonstrated that initial stenting is more economical than shunt placement. These investigators stated that since stenting became available they have not performed CSF shunting for pseudotumor cerebri.
This study had a number of strengths in addition to limitations. Compared with other studies and case series reporting outcomes for similar patients, with one exception,4 we had a relatively sizeable cohort of patients. Also, we had a reasonable follow-up time for many of the patients in our cohort, with angiographic confirmation of the anatomy and documentation of dural sinus pressures, including all restented patients. However, the small sample imposed low power to detect differences; we cannot be confident that no true differences existed between patients with/without hemodynamic failure for the variables in which there were no statistically significant differences. Although we lacked complete follow-up information for all patients, we do not suspect that those either lost to follow-up or awaiting follow-up, differed with respect to relevant clinical characteristics from those we reported.
Conclusions
We found the highest associations with hemodynamic failure to be pure extrinsic compression of the transverse-sigmoid junction pre-stenting, and possibly female gender. There were also significant differences in age and LP OP compared with patients who had hemodynamic success. Our experience to date suggests that extended stenting into the SSS maintains normal pressures in the SSS, and is associated with sustained relief of papilledema among patients whose new sinus narrowing secondary to external compression extends into the SSS. Because of the coupling of cerebrospinal fluid pressure and pressure in the SSS we believe that intracranial pressure also remains normal in these patients, even though no primary venous obstruction was present before stent placement.
References
Footnotes
Contributors Data acquisition and interpretation: DAK, JS, XH, QM, DEC, CDR, PSS, KEL, VSP, JLB. Drafting article: DAK, XH, DEC. Statistical analysis: KEL. Critical revision of article: DAK, QM, DEC, CDR, PSS, KEL, VSP, JLB. Reviewed manuscript as submitted: DAK, JS, XH, QM, DEC, CDR, PSS, KEL, VSP, JLB. Study supervisor: DAK.
Competing interests None declared.
Ethics approval Colorado multi-institutional review board.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement The authors agree to share any data on request. Any data from this study are available by contacting the corresponding author.