Article Text

Abstract
Following mechanical mitral valve replacement surgery, a 69-year-old woman had an ischemic stroke in the right middle cerebral artery territory. Mechanical thrombectomy showed the embolus to be a piece of chordae tendineae excised during the valve replacement surgery.
- Stroke
- Thrombectomy
- Technique
- Endoscopy
- Complication
Statistics from Altmetric.com
Background
Heart valve replacement surgeries have become an increasingly viable treatment for patients with severe valve degeneration for whom valve repair is not an option. Like most cardiac surgeries, mitral valve replacement surgery (MVR) comes with a risk of stroke. This risk increases with the addition of factors such as advanced age, persistent atrial fibrillation, and mitral annular calcification.1
Immediate sources of emboli following cardiovascular procedures can be foreign materials dislodged or left behind from the procedure. Foreign body emboli found following interventional surgery are often non-biological material such as guidewires2 and synthetic fibers.3 Such non-biological materials are not small enough to reach the cerebral vasculature and often result in pulmonary embolism. The most common sources of non-thrombotic organic emboli in the literature are fat, amniotic fluid, tumor, and gas bubbles, which more frequently result in pulmonary rather than cerebral embolism due to their size and origin.4 It is rare for non-thrombotic organic material to cause cerebral ischemia.
We present a patient who experienced an acute ischemic stroke due to a non-thrombotic organic embolus resulting in a large vessel occlusion as a complication of open heart MVR surgery. The organic embolus was successfully removed with mechanical thrombectomy using the ADAPT technique.5 ,6
Case presentation
A 69-year-old woman underwent open heart MVR surgery with a 27 mm St Jude bileaflet mechanical device in order to treat symptomatic mitral valve regurgitation caused by severe stenosis and calcification. She had no history of smoking, but had pre-existing atrial fibrillation and had previously undergone a mechanical aortic valve replacement with a 21 mm St Jude device. During extubation on postoperative day 0, the nurse noticed the patient had a left facial droop, dysarthria, and left-sided hemiplegia. A stroke code was called, and the patient was examined by the vascular neurologist who documented a National Institutes of Health Stroke Scale (NIHSS) score of 19.
Investigations
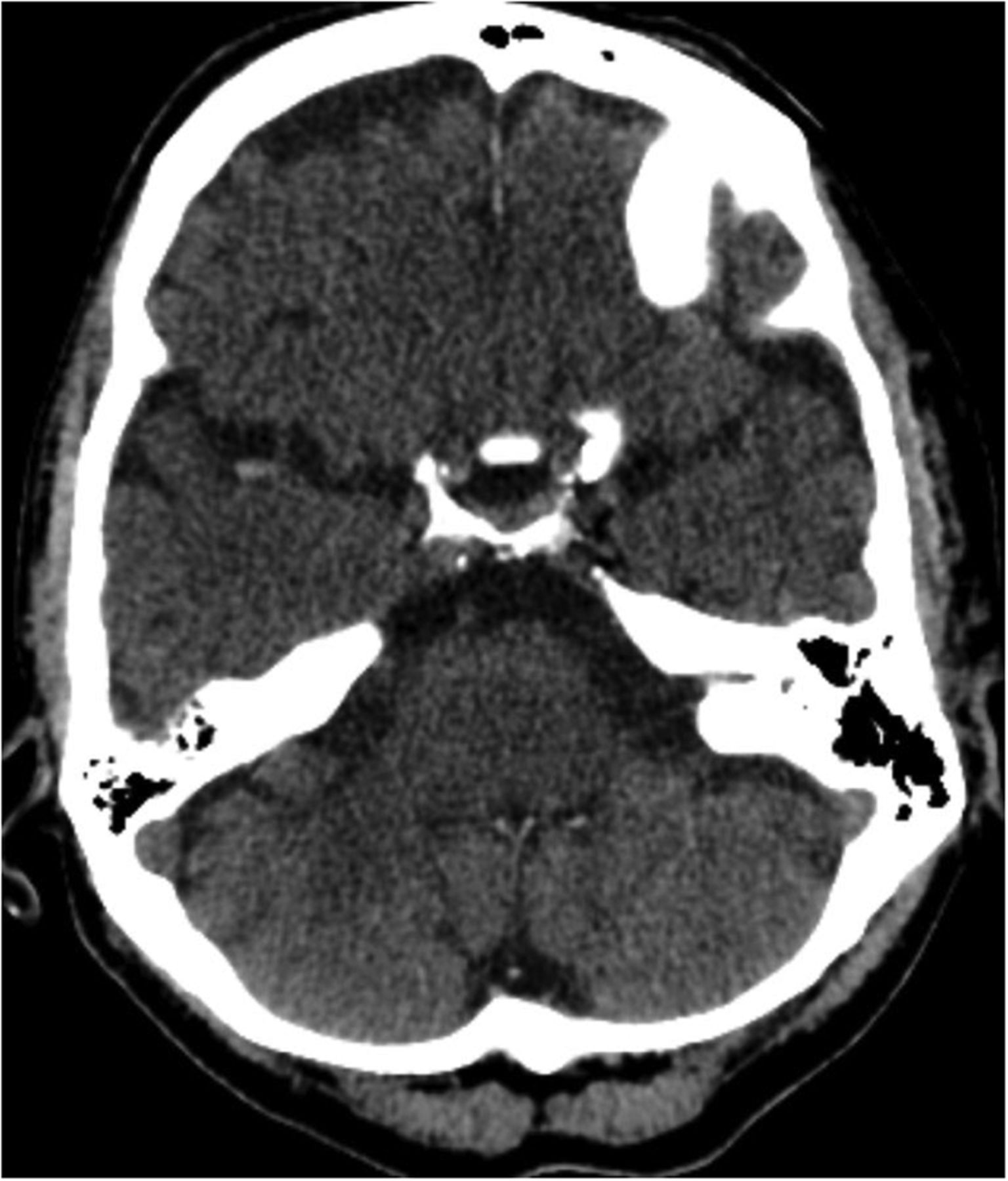
Non-contrast head CT showed a hyperdensity at the right middle cerebral artery (MCA) bifurcation but no hemorrhage (figure 1). CT angiography showed a nearly occlusive lesion at the bifurcation of the M1 segment of the right MCA, extending into the posterior M2 segment (figure 2).
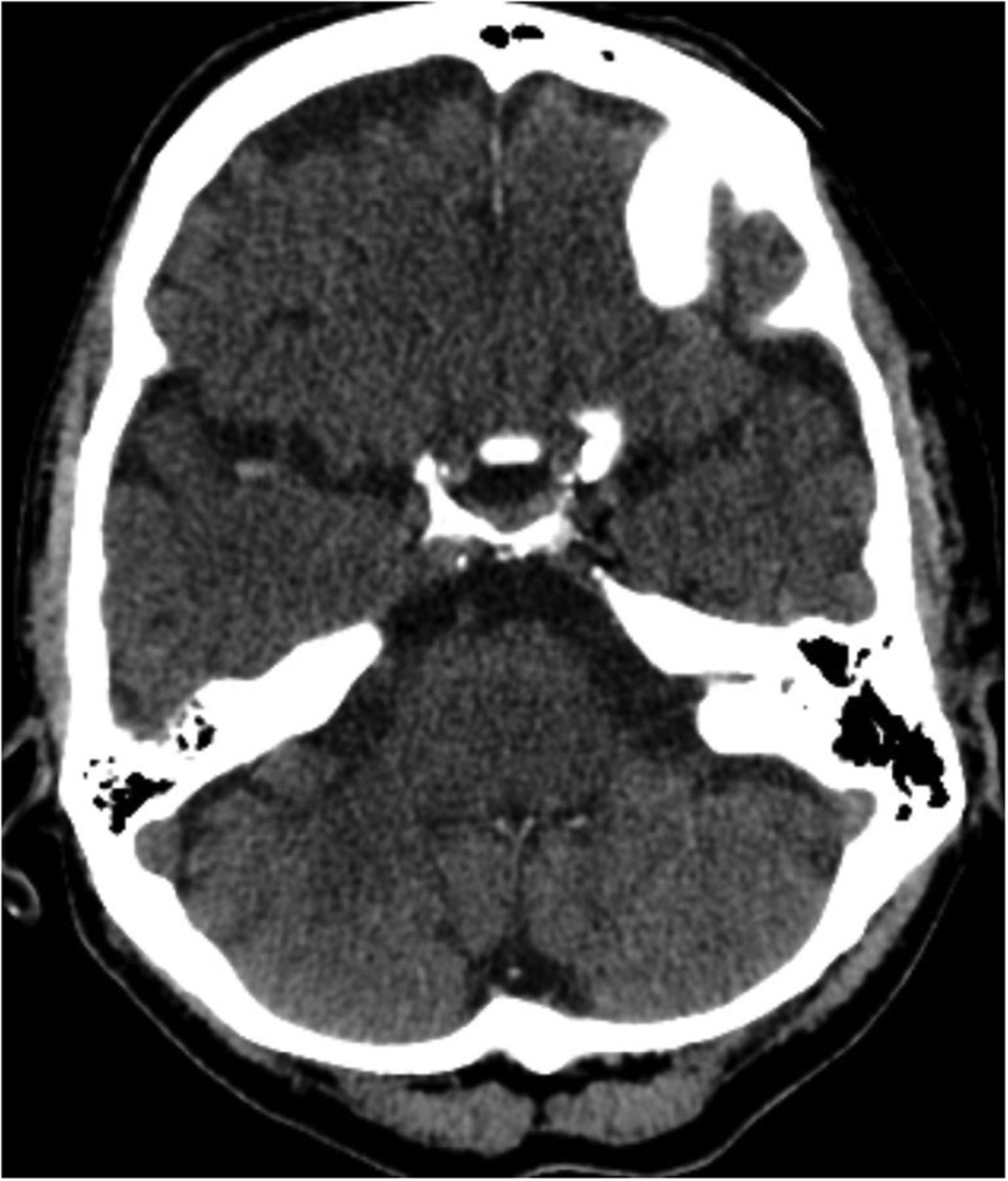
Non-contrast head CT showing a hyperdensity at the right middle cerebral artery bifurcation.

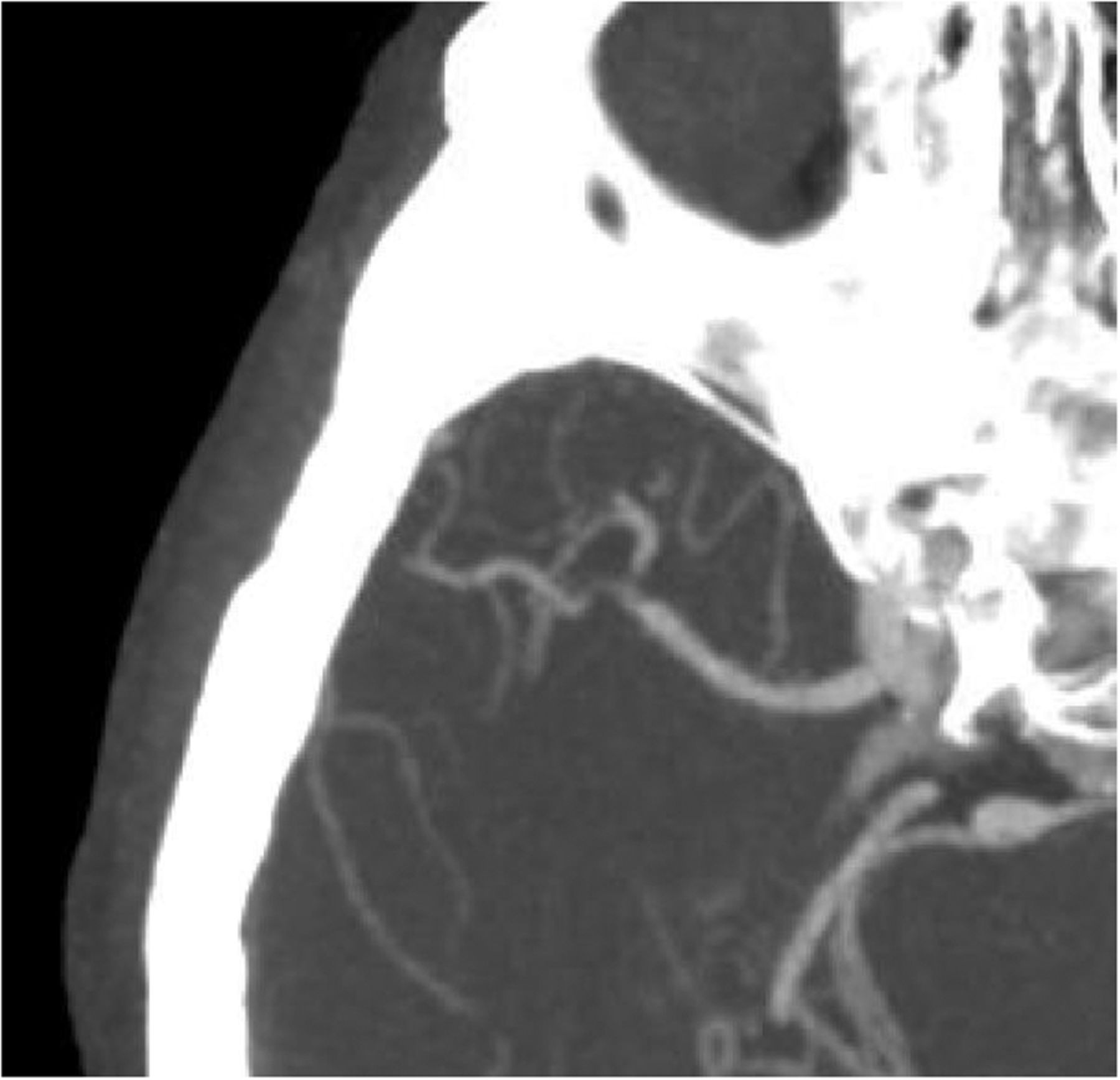
CT angiography showing a nearly occlusive lesion at the bifurcation of the M1 segment of the right middle cerebral artery, extending into the posterior M2 segment.
Treatment
The patient was unable to receive intravenous tissue plasminogen activator (tPA) because of her postoperative state, so she underwent immediate mechanical thrombectomy (figure 3). To this end, she was brought emergently to a biplane neuroangiographic suite (Axium Artis, Siemens, Germany). The procedure was performed under mild sedation using intravenous fentanyl only. After obtaining transfemoral access, an 8 F short sheath was placed, and a 90 cm Neuron MAX guide catheter (Penumbra, Alameda, California, USA) was placed in the right internal carotid artery. Of note, the time from symptom onset to groin puncture was 109 min. Subsequently, a 5MAX ACE 64 reperfusion catheter (Penumbra) was advanced into the right MCA over a Velocity microcatheter (Penumbra) over a Headliner 0.016 inch wire (MicroVention, Tustin, California, USA).
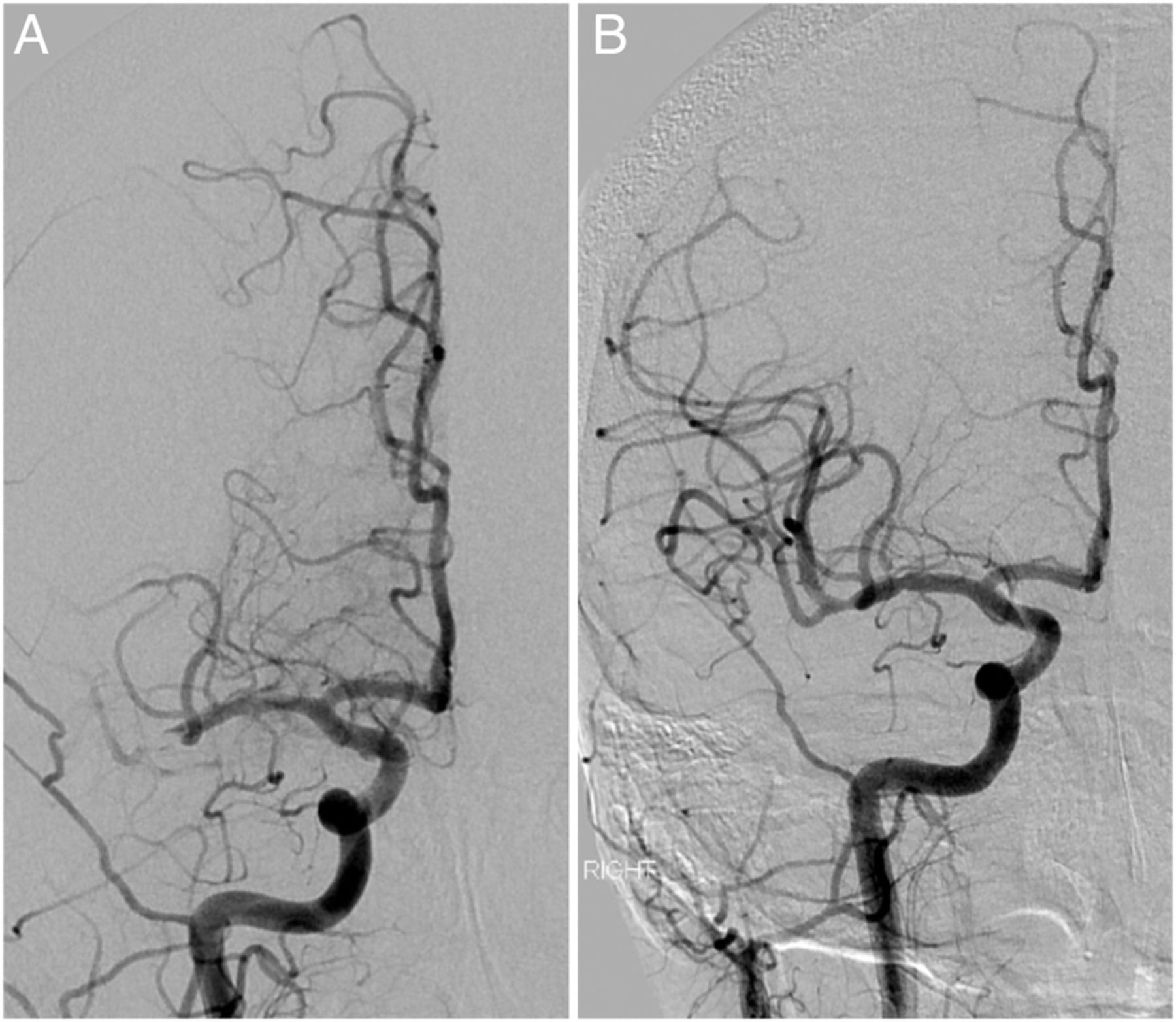
Digital subtraction angiography during a right common carotid artery injection showing (A) a nearly occlusive lesion at the distal aspect of the M1 segment of the right middle cerebral artery (MCA), extending into the posteroinferior M2 segment, and (B) restored blood flow to the entire MCA territory following embolectomy.
After removal of the Velocity and Headliner, direct aspiration was performed on the face of the occlusive lesion using the ADAPT technique.5 ,6 Despite 90 s of suction, no flow was noted in the aspiration tubing. The 5MAX ACE 64 was slowly retracted into the internal carotid artery and ultimately to the tip of the Neuron MAX. At this point, a 60 mL syringe was applied to the side port of the Neuron MAX and manual aspiration was performed during removal of the 5MAX ACE 64 (to which continuous aspiration was being applied). Despite strong manual suction on the syringe, no blood could be aspirated. At this point the occlusive lesion was suspected to be at the tip of the Neuron MAX. With maintained manual suction, the Neuron MAX was removed en bloc with the offending lesion, leaving the 8 F short femoral sheath in place. Final angiography showed Thrombolysis In Cerebral Infarction (TICI) 3 reperfusion, which was achieved 13 min after groin puncture.
The embolus removed from the MCA was not thrombotic material but rather a tan rubbery object approximately 8 mm in length. The specimen was sent to pathology for more detailed analysis, revealing that it was indeed not thrombotic material but primarily collagen with some elastin and endothelial cells, consistent with the make-up of cardiac chordae tendineae (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Gross specimen of chordae tendineae removed from the right middle cerebral artery. (B) Normal chordae in a Google image. (C) 10× magnification image of the chordae tendineae specimen.
Outcome and follow-up
Immediately following successful thrombectomy the NIHSS score was 12. Over a 2-day stay in the intensive care unit and 4 days total in the hospital, the patient continued to show dramatic improvement and the NIHSS score was down to 6 at discharge. She was then enrolled in an acute inpatient rehabilitation program. At 30-day follow-up, the patient had mild residual left-sided weakness and a modified Rankin Scale (mRS) score of 2. At 90 days she continued to improve to an mRS of 1.
Discussion
The main function of chordae tendineae is to connect the papillary muscles to the atrioventricular valves (in this case mitral valve), preventing valvular prolapse into the atria during systole. They are made up of parallel collagen and elastin fibers, yielding elasticity and high tensile strength.7 During valve replacement surgery, the chordae tendineae are excised along with the calcified valve leaflets. Preservation of the chordae tendineae and other subvalvular structures occurs in some MVR surgeries and has been found to improve left ventricle function compared with non-preservational surgery.8 In this case, chordal preservation was not attempted due to excessive valve calcification and subsequent degradation of the subvalvular apparatus. During excision, a piece of tendineae came free and was able to enter the bloodstream, becoming the offending embolus.
We believe this to be the first reported case of stroke following open MVR surgery involving embolization of heart tissue and the first involving chordae tendineae. Accounts of embolic debris generated by valve replacement are found more frequently in transcatheter aortic valve replacements (TAVR) and have caused several ischemic events similar to our case. In one such case, an approximately 1 cm segment of valve tissue caused a left MCA occlusion in a 78-year-old man immediately following TAVR, resulting in right-sided hemiplegia. The embolus was removed using a Penumbra ACE reperfusion catheter.9
Calcified material, valve tissue, pure collagenous material from the aortic wall, and thrombotic material have all been dislodged and become free emboli during TAVR cases.10 TAVR is more susceptible to dislodging emboli and causing cerebral ischemia due to the physical contact between the catheter and the likely diseased aortic arch and valve, as well as the direct flow of blood from the ascending aorta to the brain.
While less common, this case indicates that stroke due to large vessel occlusion caused by material dislodged during open MVR surgery is possible, and precautions may be considered. The use of mesh embolic protection devices placed at the brachiocephalic trunk and left common carotid artery have been successfully used during TAVR to decrease the incidence of periprocedural stroke from free emboli.10 Such devices may be useful in any cardiac valve repair and replacement procedure where tissue will be excised or inadvertently dislodged.
Additionally, this case is an important lesson in thrombectomy technique. Despite the application of continuous direct suction on the reperfusion catheter, the embolus could not have been removed safely without additional suction on the guide catheter and the presence of a short femoral sheath, which enabled complete removal of the guide catheter without loss of vascular access and potential embolization to the lower extremity.
Footnotes
Republished with permission from BMJ Case Reports Published 20 February 2017; doi:10.1136/bcr-2016-012951
Twitter Follow Yasha Kayan @yashakayan
Contributors All authors contributed to this case report.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.