Article Text

Abstract
Background Despite constant improvements in recent years, sufficient reperfusion after mechanical thrombectomy (MT) is not reached in up to 15% of patients with large vessel occlusion stroke (LVOS). The outcome of patients with unsuccessful reperfusion after MT especially after intravenous thrombolysis (IVT) use is not known. We investigated the influence of initial IVT in this particular group of patients with failed intracranial recanalization.
Methods We conducted a retrospective analysis of the Endovascular Treatment in Ischemic Stroke (ETIS) registry from January 2015 to December 2019. Patients presenting with LVOS of the anterior circulation and final modified Thrombolysis in Cerebral Infarction score (mTICI) of 0, 1 or 2a were included. Posterior circulation, isolated cervical carotid occlusions and successful reperfusions (mTICI 2b, 2c or 3) were excluded. The primary endpoint was favorable outcome (modified Rankin Scale score of 0–2) after 3 months. Secondary endpoints were safety outcomes including mortality, any intracranial hemorrhage (ICH), parenchymal hematoma (PH) and symptomatic intracranial hemorrhage (sICH) rates.
Results Among 5076 patients with LVOS treated with MT, 524 patients with insufficient recanalization met inclusion criteria, of which 242 received IVT and 282 did not. Functional outcome was improved in the MT+IVT group compared with the MT alone group, although the difference did not reach statistical significance (23.0% vs 12.9%; adjusted OR=1.82; 95% CI 0.98 to 3.38; p=0.058). However, 3 month mRS shift analysis showed a significant benefit of IVT (adjusted OR=1.68; 95% CI 1.56 to 6.54). ICH and sICH rates were similar in both groups, although PH rate was higher in the MT+IVT group (adjusted OR=3.20; 95% CI 1.56 to 6.54).
Conclusions Among patients with LVOS in the anterior circulation and unsuccessful MT, IVT was associated with improved functional outcome even after unsuccessful MT. Despite recent trials questioning the place of IVT in the LVOS reperfusion strategy, these findings emphasize a subgroup of patients still benefiting from IVT.
- stroke
- thrombectomy
- thrombolysis
- intervention
Data availability statement
The data used in this study are available from the corresponding author upon reasonable request.
Statistics from Altmetric.com
Introduction
Current guidelines for the treatment of large vessel occlusion stroke (LVOS) advocate ‘bridging therapy’, which consists of administration of intravenous thrombolysis (IVT), in the absence of contraindication, combined with mechanical thrombectomy (MT). Unfortunately, endovascular treatment results in insufficient recanalization in approximately 15% of cases.1–3 For these patients experiencing failed MT, the influence of IVT is unknown so far. Furthermore, the systematic use of IVT in combination with MT has now become a matter of debate since recent publications of randomized controlled trials (RCTs) DIRECT-MT, SKIP and DEVT have suggested noninferiority of direct MT compared with bridging therapy.4–7 The usual pros and cons for IVT are on the one hand providing recanalization of residual thrombi after MT and improving distal micro-vascularization permeability, but on the other hand, a potentially increased hemorrhagic complication rate.8 Previous studies revealed a benefit of using IVT associated with MT.9 10 However, these findings have not been confirmed so far with the results of the first RCTs.4–6 To date, there are no studies in the literature that have assessed the influence of IVT when recanalization after MT fails or is insufficient.
The aim of our study was to evaluate the impact of initial IVT for patients who subsequently experienced failure (final modified Thrombolysis In Cerebral Infarction (mTICI) score of 0, 1 or 2a) of intracranial recanalization with MT for large vessel occlusion of the anterior circulation.
Materials and methods
Population
We conducted a retrospective analysis of the prospectively maintained Endovascular Treatment in Ischemic Stroke (ETIS: ClinicalTrials.gov Identifier: NCT03776877) registry. ETIS is an ongoing multicentric observational registry collecting clinical, procedural and imaging data from consecutive patients receiving endovascular treatment for large vessel occlusion stroke. At the time of our study, nine French comprehensive stroke centers participated. The study period was January 2015 to December 2019. Local ethical committees had approved data collection and analysis. The data used in this study are available from the corresponding author on reasonable request.
Patients who underwent MT for proximal occlusion of the anterior circulation (tandem or intracranial internal carotid artery or M1 and/or M2 segments of the middle cerebral artery), with insufficient final revascularization (final mTICI 0, 1 or 2a), combined or not with initial IVT, were included.
Posterior circulation, anterior cerebral artery and isolated cervical carotid artery occlusions were excluded. Favorable final recanalization (final mTici 2b or 2 c or 3) were also excluded.
Treatment
IVT was administered within 4.5 hours after onset according to international guidelines, using recombinant tissue plasminogen activator in the absence of contraindications. The indications for MT were based on the timeframes, imaging data, global comorbidities and standard guidelines. MT was performed depending on the patient’s condition and local protocol.
Collected data
Trained research nurses assessed the modified Rankin Scale (mRS) score at 90 days, during face-to-face interviews or via telephone conversations with the patients, their relatives or their general practitioners. Favorable outcome was defined as a 90-day mRS score of 0–2. Reperfusion failure was defined as final mTICI 0, 1 or 2a. Procedural complications (dissection, embolism in a new territory (ENT) and arterial perforation) and 90-day mortality rates were recorded. Intracranial hemorrhage (ICH) was assessed according to the ECASS II classification. Symptomatic intracranial hemorrhage (sICH) was defined as neurological deterioration (NIHSS worsening ≥4 points or death) along with ICH.
Statistical analysis
Continuous variables are expressed as mean (SD) in the case of normal distribution or median (IQR) otherwise. Categorical variables are expressed as number (percentage). Normality of distributions was assessed using histograms and the Shapiro-Wilk test. Baseline characteristics were described according to the treatment: no IVT versus IVT.
We assessed the impact of IVT treatment on main outcomes (favorable, excellent, death, any ICH, sICH, procedural complications) using a logistic mixed model and taking into account center effect. We used multivariable logistic mixed models to adjust the association between IVT and main outcomes on the following prespecified confounding factors: age, antithrombotic use, initial National Institutes of Health Stroke Scale (NIHSS) and Alberta Stroke Program Early CT (ASPECT) scores, occlusion site, delay between onset to puncture, direct admission, mRS pre-stroke score <2 and center. A comparison of overall distribution of mRS (shift analysis with mRS 5 and 6 grouped) was performed with the GLMM model using a multinomial distribution and a cumulative logit link function in univariate and multivariate analyses (adjusted on prespecified factors cited above); common OR for one point improvement was derived from this model as effect size.
Finally, we assessed heterogeneity in association with IVT treatment and main outcomes (favorable, excellent, death, any ICH, sICH, procedural complications) across mTICI score (0+1 vs 2a) by including an interaction term in logistic mixed models.
Statistical testing was performed at the two-tailed α level of 0.05. Data were analyzed using the SAS software package, release 9.3 (SAS Institute, Cary, NC).
Results
Study population
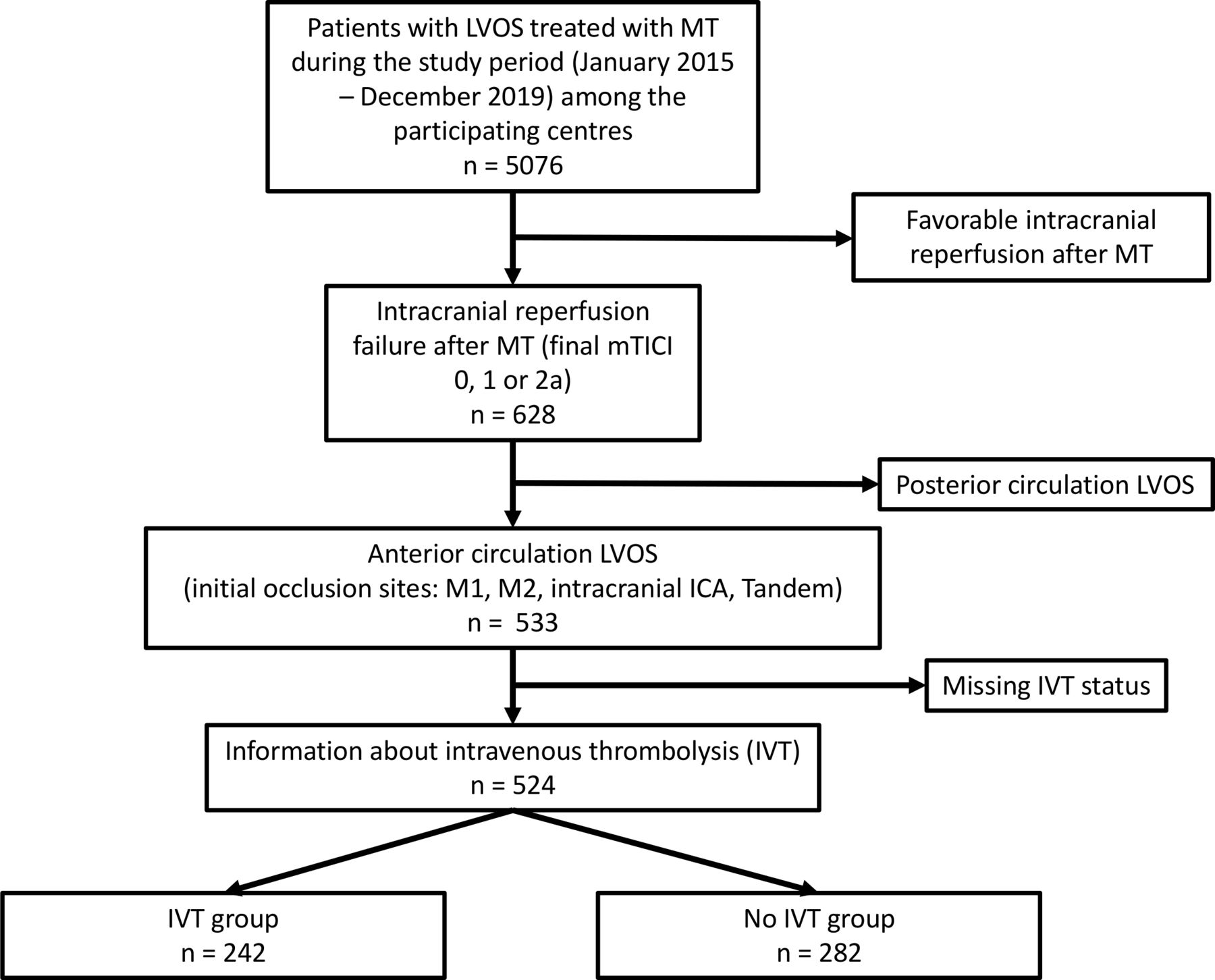
From January 2015 to December 2019, among 5076 patients who were treated with MT in the nine participating comprehensive stroke centers, we included 524 patients (10.3%) with insufficient revascularization who met aforementioned inclusion and exclusion criteria (study flowchart, figure 1). Among these patients, IVT was administered in 242 and 282 were not treated with IVT. Baseline characteristics of patients are presented in table 1. The main baseline characteristics were as follows: mean age 69.3±16.5 in the no IVT group and 68.2±15.2 in the IVT group, pre-stroke mRS <2 rates were 84.4% and 92.7%, respectively, median initial NIHSS were 17 (IQR=13–21) and 17 (IQR=12–20), respectively, median initial ASPECT scores were 7 (IQR=5–8) and 7 (5–8), respectively, and time from onset to puncture were 256 min (IQR=187–350) and 269.5 min (199–329), respectively. Wake up stroke (43.6% vs 23.1%) and pre-stroke anti-thrombotic therapy (47.1% vs 28.7%) were more frequent in the non-IVT group. The reasons for non-administration of IVT were: outside the time window (n=99; 36.26%), curative anticoagulant therapy (direct oral anticoagulant or heparin; n=39; 14.28%), INR >1.7 (n=28; 10.26%), non-intracranial hemorrhagic risk (n=37; 13.55%), extended cerebral infarction (n=23; 8.42%), previous recent ischemic stroke on imaging (n=14; 5.13%), thrombocytopenia (n=4; 1.47%), uncontrolled high blood pressure (n=4; 1.47%), intracranial hemorrhagic lesion (n=9; 3.30%), operator’s decision (n=7; 2.56%), and other (n=9; 3.30%) (data were missing for 9 patients).

Study flowchart. IVT, intravenous thrombolysis; LVOS, large vessel occlusion stroke; MT, mechanical thrombectomy; mTICI, modified Thrombolysis in Cerebral Infarction.
Baseline characteristics according to use of intravenous thrombolysis prior to endovascular treatment in patients with recanalization failure
Primary outcome
As shown in table 2, the primary outcome was achieved for 12.9% (n=33) of patients in the no IVT group and 23% (n=47) of patients in the IVT group (unadjusted OR=2.02; 95% CI 1.24 to 3.31; p=0.005). After adjustment of confounding factors, the multivariate analysis almost reached statistical significance because the adjusted OR was 1.82 (95% CI 0.98 to 3.38; p=0.058). Furthermore, shift analysis demonstrated a significantly positive impact of IVT on clinical outcome (see figure 2) (adjusted common OR 1.68; 95% CI 1.10 to 2.57; p=0.005).

{kind=link}
{kind=link}
Distribution of modified Rankin Scale score at 90 days according to use of intravenous thrombolysis prior to endovascular treatment. cOR calculated for one-point improvement in modified Rankin score using a mixed ordinal logistic regression model (with modified Rankin Scale score of 5 and 6 grouped) adjusted on prespecified factors such as age, antithrombotic use, initial NIHSS and ASPECT score, occlusion site and delay between onset to puncture, direct admission and mRS pre-stroke score<2 and including center as random effect. Scores range from 0 to 6, with (0) indicating no symptoms, (1) no clinically significant disability, (2) slight disability (patient is able to look after own affairs without assistance but is unable to carry out all previous activities), (3) moderate disability (patient requires some help but is able to walk unassisted), (4) moderately severe disability (patient is unable to attend to bodily needs without assistance and unable to walk unassisted), (5) severe disability (patient requires constant nursing care and attention), and (6) deaths. ASPECT, Alberta Stroke Program Early CT; cOR, common odds ratio; IVT, intravenous thrombolysis; NIHSS, National Institutes of Health Stroke Scale.
Outcomes according to use of intravenous thrombolysis prior to endovascular treatment in patients with failure of recanalization
Secondary outcomes
Mortality rates were similar in both groups (37.3% vs 40.2%; adjusted OR 0.88; 95% CI 0.53 to 1.47; p=0.63). The rate of any ICH did not differ between groups (55.4 vs 51.8%; adjusted OR 1.34; 95% CI 0.85 to 2.09; p=0.20). Parenchymal hematoma (PH) rate was significantly superior in the IVT group (17.0 vs 11.9%; adjusted OR 3.20; 95% CI 1.56 to 6.54; p=0.005). Symptomatic ICH rate was higher in the IVT group even if the difference did not reach significance (16.8 vs 12.1%; adjusted OR 1.89; 95% CI 0.97 to 3.67; p=0.062). Per procedural complication rates were similar between groups (22.0 vs 25.8%; adjusted OR 1.25; 95% CI 0.76 to 2.06; p=0.22). Per procedural complication details are provided in online supplemental table 1.
Supplemental material
Subgroups analysis
The potential heterogeneous effect of IVT was explored through subgroups analysis. No significant difference regarding benefit of IVT according to reperfusion grade (mTICI 0 to 1 vs 2a) was observed regarding primary endpoint (all p-het >0.05) (online supplemental figure l).
Discussion
We found that, for cases of failed MT for LVOS of the anterior circulation, initial IVT was associated with improved clinical outcome at 3 months. However, initial IVT also seemed to be associated with an increased PH rate.
Potential positive effects of IVT in the setting of associated MT have previously been discussed in the literature. Several hypotheses about the complementary roles of IVT and MT are commonly proposed. First, the direct pharmacological effect of IVT on proximal thrombus lysis favoring arterial recanalization whatever the result of MT, the direct lytic role on potential distal thrombus fragments and facilitation of clot removal reducing the number of required MT passes are obviously plausible and mostly mentioned.9 10 Then, a significant reduction in the occurrence of infarct in new territories has also been reported after IVT combined with MT in comparison with MT alone.11 Interestingly, in a preclinical study, Desilles and colleagues also demonstrated that IVT was associated with microvascular network repermeabilization improvement and patency maintenance.12 Consequently, IVT might also promote reperfusion when endovascular recanalization failed.13 Yet, recent RCTs raised strong evidence of non-inferiority of MT alone compared with combined IVT and MT.4–6 Interestingly, the DIRECT-MT trial reported an increased rate of pre-MT reperfusion and improved final reperfusion rates, reinforcing the possibility of persisting benefit of IVT for selected patients and indications. These findings also raise the question of the potential negative impact of skipping IVT for patients in whom MT will unfortunately fail to reach intracranial reperfusion. Among these 9.9% (SKIP study) to 20.6% (DIRECT-MT) of MT failures (final mTICI <2 b) in recent RCT trials, it would be of interest to specifically explore the influence of IVT status on outcomes. To date, these data are not available, which reinforces the interest in our study as this point is underreported.
At the time of questioning the place of IVT among the treatment algorithm of LVOS, our results also raise discussion about the relevance of complementary fibrinolytic or antithrombotic drugs according to the final reperfusion obtained with standard MT. The literature about pharmacological and mechanical rescue therapies in the setting of failed MT is growing.14–18 In particular, studies about complementary fibrinolytic treatments have been published with promising results.18 19 As experimental studies revealed encouraging pharmacological therapeutic targets,20–23 the possibility of improving antithrombotic and/or fibrinolytic strategies should not be neglected. Our findings, which are in line with the available literature, urge the development of a standardized rescue strategy for cases of thrombectomy failure.
Regarding adverse events, even if the difference relating to sICH did not reach significance, the PH rate was significantly higher in the IVT+MT group. PH and sICH rates were quite high among our population. However, it is important to note that we only included patients with failed intracranial recanalization, which is a major prognosis factor often associated with increased rate of intracranial hemorrhage.24 25 Nevertheless, this consideration should incite careful indication criteria to be maintained for IVT or potential in situ anti-thrombotic medications. Endovascular periprocedural complication rates were comparable between groups.
Several limitations of our study should be pointed out. First, even if our study population was substantial, statistical analysis may lack power. Second, several clinical characteristics were not balanced between the two groups. As expected, comorbidities were more frequent in the no IVT group (history of stroke, history of ischemic heart disease, antithrombotic treatment), potentially resulting in bias. However, multivariate adjusted analyses were used to moderate the influence of such confounding factors. Still, other confounding factors may have played a part. Unfortunately, hemodynamic and biological data that could have influenced outcomes were not widely available.
Conclusion
Our study revealed that in patients who experienced failure of MT for stroke due to large vessel occlusion of the anterior circulation, IVT was associated with improved functional outcome at 3 months. Despite recent RCTs questioning the place of IVT in the acute therapeutic strategy for LVOS and because the subgroup experiencing failed MT cannot be determined prior to endovascular treatment, this study argues against withholding IVT in this population.
Data availability statement
The data used in this study are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
ETIS (ClinicalTrials.gov Identifier: NCT03776877) is an ongoing multicentric observational registry collecting clinical, procedural and imaging data from consecutive patients receiving endovascular treatment for large vessel occlusion stroke. Local ethical committees had approved data collection and analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @BenjaminMaierMD, @jildazz
Collaborators On behalf of the Endovascular Treatment in Ischemic Stroke ETIS- Research Investigators: FOR : Michel Piotin, Raphael Blanc, Hocine Redjem, Simon Escalard, Jean-Philippe Desilles, Delvoye François, Stanislas Smajda, Benjamin Maier, Hebert Solène, Mikael Mazighi, Mikael Obadia, Candice Sabben, Seners Pierre, Raynouard Igor, Ovide Corabianu, Thomas de Broucker, Eric Manchon, Guillaume Taylor, Malek Ben Maacha, Thion Laurie-Anne, Lecler Augustin, Savatovsjy Julien. FOCH: Adrien Wang, Serge Evrard, Maya Tchikviladze, Nadia Ajili, Bertrand Lapergue, David Weisenburger-Lile, Lucas Gorza, Géraldine Buard, Oguzhan Coskun, Arturo Consoli, Federico Di Maria, Georges Rodesh, Sergio Zimatore, Morgan Leguen, Julie Gratieux, Fernando Pico, Haja Rakotoharinandrasana, Philippe Tassan, Roxanna Poll, Sylvie Marinier. LYON : Norbert Nighoghossian, Roberto Riva, Omer Eker, Francis Turjman, Laurent Derex, Tae-Hee Cho, Laura Mechtouff, Anne Claire Lukaszewicz, Frédéric Philippeau, Serkan Cakmak, Karine Blanc-Lasserre, Anne-Evelyne Vallet. BORDEAUX: Gaultier Marnat, Florent Gariel, Xavier Barreau, Jérôme Berge, Patrice Menegon, Igor Sibon, Ludovic Lucas, Stéphane Olindo, Pauline Renou, Sharmila Sagnier, Mathilde Poli, Sabrina Debruxelles, François Rouanet, Thomas Tourdias, Jean-Sebastien Liegey, Pierre Briau, Nicolas Pangon. NANTES : Romain Bourcier, Lili Detraz, Benjamin Daumas-Duport, Pierre-Louis Alexandre, Monica Roy, Cédric Lenoble, Hubert Desal, Benoît Guillon, Solène de Gaalon, Cécile Preterre. NANCY : Benjamin Gory, Serge Bracard, René Anxionnat, Marc Braun, Anne-Laure Derelle, Romain Tonnelet, Liang Liao, François Zhu, Emmanuelle Schmitt, Sophie Planel, Sébastien Richard, Lisa Humbertjean, Gioia Mione, Jean-Christophe Lacour, Nolwenn Riou-Comte, Gérard Audibert, Marcela Voicu, Ionel Alb, Marie Reitter, Madalina Brezeanu, Agnès Masson, Adriana Tabarna, Iona Podar, Sarah Guy, Fatiha Bechiri. LIMOGES: Francisco Macian-montoro, Suzanna Saleme, Charbel Mounayer, Aymeric Rouchaud. MONTPELLIER : Vincent Costalat, Caroline Arquizan, Cyril Dargazanli, Grégory Gascou, Pierre-Henri Lefèvre, Imad Derraz, Carlos Riquelme, Nicolas Gaillard, Isabelle Mourand, Lucas Corti, Federico Cagnazzo, Adrien ter Schiphorst. RENNES : Eugene Francois, Stéphane Vannier, Jean-christophe Ferre, helene Raoult, Thomas Ronziere, Maria Lassale, Christophe Paya, Jean-Yves Gauvrit, Clément Tracol, Sophie Langnier-Lemercier. PITIE-SALPETRIERE : Yves Samson, Charlotte Rosso, Anne Leger, Sandrine Deltour, Frederic Clarencon, Eimad Shotar. Kremlin-Bicêtre : Laurent Spelle, Christian Denier, Olivier Chassin, Vanessa Chalumeau, Jildaz Caroff, Olivier Chassin, Laura Venditti. Sainte ANNE : Olivier Naggara, Wagih Ben Hassen, Grégoire Boulouis, Christine Rodriguez-Régent, Denis Trystram, Basile Kerleroux, Guillaume Turc, Valérie Domigo, Catherine Lamy, Julia Birchenall, Clothilde Isabel, François Lun, Wassim Farhat, Matthieu Zuber, Olivier Heinzlef. TOULOUSE : Alain Viguier, Christophe Cognard, Anne Christine Januel, jean-Marc Olivot, Nicolas Raposo, Fabrice Bonneville, Jean François Albucher, Lionel Calviere, Jean Darcourt, Philippe Tall, Guillaume Bellanger, Louis Fontaine. CAEN : Emmanuel Touze, Charlotte Barbier, Romain Schneckenburger, Marion Boulanger, Julien Cogez, Sophie Guettier. BREST : Serge Timsit, Jean-christophe Gentric, Julien Ognard, Francois Mathias Merrien. ROUEN : Ozlem Ozkul Wermester, Evelyne Massardier, Chrysanthi Papagiannaki. BAYONNE: Frédéric Bourdain, Bernady Patricia, Lagoarde-Segot Laurent, Cailliez Hélène, Veunac Louis, Higue David. STRASBOURG: Wolff Valérie, Dr Pop Raoul, Beaujeux Rémi, Mihoc Dan-Sorin, Manisor Monica. VANNES: Le Bras Anthony, Evain Sarah, Le Guen Arnaud. PAU : Richter Sebastian, Hubrecht Regis, Demasles Stéphanie, Barroso Bruno. PERPIGNAN : Denis Sablot, Geoffroy Farouil, Maxime Tardieu, Philippe Smadja, Sabine Aptel, Ian.
Contributors CR, GM, BM, BG, RB, BL, IS acquired the data, analyzed the results, drafted the manuscript and critically reviewed the manuscript. MK and JL performed statistical analysis and analyzed the results. AC, MM, RB, FG, JC, ON, FE acquired the data and critically reviewed the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Outside this work: JL reports grants from Stryker, Penumbra and Microvention. MM reports personal fees from Acticor Biotech, Air liquide, Amgen and Boerhinger.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.